![]()
© Crown copyright 2024
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at www.gov.uk/official-documents.
Any enquiries regarding this publication should be sent to us at [email protected].
ISBN 978-1-5286-4685-7
E03066671 05/24
Attitudes to risk go to the heart of the matters this Inquiry is tasked to look into.
More than one politician giving evidence accepted that a first duty of a state is to keep its citizens safe. They were right to do so. It is clear that unless the safety of citizens is regarded as a first consideration there may be harm, and that harm might have been avoidable.
In today’s society risk, meaning the possibility of physical or mental injury, is ubiquitous and inescapable. Almost everything we do comes with the possibility of some adverse consequence of one form or another. Driving a car risks injuring other people, as well as the driver and any passenger, but the purpose of driving it would be defeated if the existence of these risks required cars to be banned. Instead, action can be taken to reduce the likelihood of risks – by such as airbags, better car design, more effective braking, speed limits where appropriate, and by taking individually protective steps such as wearing seat belts. Where the harm that might happen is not that of accidental injury, but of disease, or of a consequence of medical treatment, the principle “first do no harm” may be engaged. However, any treatment will come with some consequences, just as a decision not to treat actively may also do. Those consequences may be serious. It is why pharmaceuticals distributed in the UK will come with a product leaflet pointing out risks which might transpire. They do not aim to stop a person taking the medicine, but to enable clinicians to alert people to what might be an unwanted consequence: that person can then make their own choice whether to take the medicine, and run those risks, or to decline it.
Whether it is necessary to take precautions against a risk depends on the balance to be struck between the magnitude of the risk on the one hand, and the importance of the purpose to be achieved by running it on the other, taken together with the practicability and cost of preventative measures. The assessment will take into account whether alternatives offering less risk are available. Care may need to be taken that any precaution does not itself cause unreasonable risk.
The magnitude of the risk is a combination of the likelihood that what is feared will occur, coupled with its seriousness if it does. Thus, catching the common cold, especially in winter time, is highly likely to occur, but the infection is unlikely to be of any great severity if it does. If the risk is that of flu, it is less likely to occur, but more serious if it does: and in that case, for those who are particularly vulnerable to serious damage to their health if they do catch flu, there are vaccinations to ward against it. A small chance of a more deadly illness occurring – for instance cancer caused by the use of some industrial solvents – would be a risk of much greater magnitude, even though much less likely to occur.
In just the same way, it may be very rarely that a bolt on the wing or body panel of an airliner is left loose when it should be tight, especially when thinking about the number of flights taken every day, worldwide, without that being known to happen. But the consequence of leaving it loose is a risk that the airliner might crash. A small chance of that serious risk plainly requires preventative action to be taken. It does not need to wait for an accident to happen before it occurs, if it can be foreseen that it might. In short, the magnitude (or size) of a risk is not simply a question of counting the number of cases there has been, but the foreseeability they may arise and the gravity of the harm if they do.
The Inquiry has centrally concerned the risks of three diseases by name – hepatitis (of two principal sorts, B and C, undistinguished one from the other for the first 20 years or so of the NHS); AIDS (HIV being the virus which led to it); and vCJD. The magnitude of those risks is now undoubted.
Looking some 70 years ago, though, hepatitis (“serum hepatitis”, as the mixture of what was largely B and C was then called) was seen as a definite risk of transfusion, and it was already recognised that it could be a serious condition (see the chapter on Knowledge of Risk Before 1970). It was thus already seen to be of some magnitude. The importance of the purpose was to be achieved depended on the need for the intended transfusion, or treatment: and (as will be seen) some protective measures were taken. An issue in respect of hepatitis, discussed in later chapters, is whether many health professionals became so inured to their patients running the risk that those measures did not go far enough, quickly enough; whether alternatives were available which carried no or less risk; and whether those people who had to face the risk (the patients) were told by their treating clinicians enough of what was known about the risk to enable the patient to make their own judgement about running it.
When it was realised, after it became possible to test for the presence of Hepatitis B virus, that another as yet unidentified virus (“non-B”, or “non-A non-B”) was responsible for a greater proportion of the hepatitis which had followed transfusion or the taking of blood products, the magnitude of the risk it posed was thought debatable by many health professionals. Whereas Hepatitis B was undoubtedly potentially serious, it was unclear to them that this was also true of the unidentified virus. If it had not been serious, then the practicability and cost of protective measures against it would come into question. Whether such an assumption was an appropriate way of approaching the risk which the unidentified virus posed is considered further in the chapter Hepatitis Risks 1970 and After.
With AIDS, the issue at first was centrally that of the magnitude of the disease. First, did treatment for bleeding disorders or transfusion risk causing the disease (or was the cause something entirely different)? Second, if it did, was the magnitude of the risk sufficient to call for a protective response? There was little doubt, from mid 1981 onwards, that AIDS itself was a very serious disease. A risk of suffering it, therefore, would almost unarguably be of significant magnitude: thus, even if the chances of treatment causing or transmitting it were slim, protective measures or alternative means of meeting the purpose of giving the treatment would be called for. The issues which arose (at least until 1984, as later chapters reveal) were whether there was in truth any real risk from the treatment; and if so, whether the chances of treatment causing AIDS were so slim that the risk could properly be regarded as requiring little or nothing to be done to protect against them.
In assessing the chances of occurrence of infection, it must be remembered that it is of the nature of many diseases that an infection which causes symptoms recognisable by a patient may be caused by events some time previously. The lag time between infection and the occurrence of the obvious ill effects of it may be short – but it might be months and even years. In assessing the likelihood that that disease will eventuate, regard must be had to the fact that what is coming out of the tap may not be the full extent of what is in the pipeline. If a disease takes two years to show itself, then one has to go back two years to see what the cause is. If that is identified, then it may also be true that that has been the cause of other infections throughout the entire two-year period, which have yet to show themselves.
In an epidemic, where cases of a disease being transmitted from one person to another multiply exponentially, it will follow that the number of transmissions two years ago will be far less than they were a year ago, and the rate of transmissions a year ago far less than they were six months ago, and the rate six months ago far less than now. To look at the number of individual cases of disease which have, by now, shown themselves is to look at the incidence of infections two years ago: it does not give an accurate picture of the risk of transmissibility to anyone newly exposed to its transmission, nor is it an accurate reflection of the number of cases that will emerge over the next two years. They will be escalating, exponentially, unless something happens to prevent this.
The Observer on 1 May 1983, [1] expressed these ideas concisely in everyday language in relation to AIDS when it said: “The disease, characterised by a collapse in the body’s ability to fight infection, is a medical time-bomb for Britain. Although only fifteen cases have been reported since it first crossed the Atlantic in December 1981, many more people could be harbouring it, for the incubation period is up to three years.” In other words, the risk that requires a response is the risk of what may be coming.
In assessing the degree of likelihood of the infection as part of judging the magnitude of the risk, it should also be borne in mind that one reason why diseases sometime seem to emerge suddenly in parts of the world new to them is the modern ease and speed with which people cross borders, travelling distances in hours that once took weeks or months. There is danger in thinking that a disease is somewhere else, and not here, when there is no basis to do so. The chapter on the Knowledge of the Risks of AIDS amply demonstrates this in the context of this Inquiry: AIDS was too often regarded either as an “American problem” or “more of an American problem”, which might have been true at the time if one looked at the number of reported cases in North America, but actually said nothing about the risk it might happen here. The question to ask should have been “Is there any reason to think it will not come to the UK?” Epidemics can be exported, or refuelled, from around the world.
If, then it is reasonable for protective measures (or alternatives) to be called for, what can be said about their timing and nature? First, it is elementary that a response to a real risk that a disaster might occur should not wait. What must be addressed is the risk, not the certainty or near certainty, of damage; and the time for addressing it is before damage occurs. Speed of reaction to risk is of the essence.
As to the nature of the response, if a risk appears to be real, and if that risk is one of sufficient magnitude, then it is a fallacy to suppose that the response should be “all or nothing” – that is, if the risk cannot be eliminated, it must be tolerated. There is a real value in reducing the risk.
Two examples of this may be drawn from the subject of the Inquiry. First, that of Hepatitis B. Once it was identified and a test made available for it in about 1970, a universal screening test for donations was quickly introduced by 1972. This was not sensitive enough at first to identify more than around a third of the infective units. Nonetheless, though this lack of sensitivity was known, a universal test was introduced in the UK (at some expense, as well as at some further cost in human resource). To incur that expense (of time, effort and money) was nonetheless an appropriate reaction, when combined with attempts to improve the quality of the test. It was (rightly) thought valuable to reduce the risk even to the limited extent achieved by the test.[2]
So, too, in 1998 a decision was taken to reduce a risk which was by then only theoretical: that plasma might transmit the prion which caused vCJD to develop in the brain. The removal of white blood cells from plasma (“leucodepletion”) was adopted. This precaution looks, on available current evidence, to have significantly reduced the risk of plasma products transmitting the infective prion which caused the condition. Yet at the time it was taken there had been no known case of transmission of vCJD by blood. If government had waited until the first case was reported, more cases might have followed than actually did.
These are two examples of responses to risk which may fall short of complete elimination of the risks involved, but were nonetheless (rightly) considered appropriate by the authorities at the time.
Identifying that there was real risk would, in the cases of both hepatitis and HIV, lead to the obvious answer that it was a risk of significant magnitude, given the seriousness of the consequences of infection. The importance of running that risk, coupled with the availability of protective measures and alternatives, then called for evaluation. An issue in this Inquiry has been that the purpose was said to be ensuring that people with bleeding disorders received treatment which was life-saving; an approach which begged the question whether there were safer alternatives which had less risk which were also life-saving, and/or other measures which would reduce the risk even if there were no suitable alternative.[3] The same is true for transfusion as a treatment: whilst it can obviously be life-saving, the evidence before the Inquiry indicates that transfusions were also often given in circumstances where there was no threat to life.
Summing up, after identifying a real risk to health safety what is critical in the process is acting with speed to address it:
A successful system of identifying and reacting to risks of sufficient magnitude to justify a reaction thus involves constant vigilance, “horizon scanning” and the taking of urgent coordinated action in response. It also will demand a way of assessing whether the consequences involved in taking that urgent action in response to the risk (the “knock-on” effects) are themselves not unreasonable, and do not create worse problems than they solve.
So far as biological threats to people in the UK are concerned, such an approach demands a system of public health capable of achieving this. One of the paradoxes of a good public health system is that there will seem to be no need for it – if it succeeds in identifying and taking steps which will ward off the emergence in the UK of a threat which is real, then it may seem that there has been nothing to worry about. The public may wonder what the point is of spending money when it seems there has never been a case of any such infection.
It is not always easy to identify whether the risk is of a kind which can be ignored, which is why it has never emerged, or whether the system to prevent it taking hold has worked. The sense of security into which a good public health system may lull the population may thus, paradoxically, lead to the complacency about it which is its worst enemy. One of the lessons from the account which follows is that the UK, as a nation, had become too complacent about the risk of infectious diseases, and not sufficiently concerned about resourcing public health.
I regard it as a very important principle in relation to the way risk is handled that so far as practicable those whose safety is at risk should be told this is the case, in sufficient detail and with sufficient clarity for them to understand what the risk is and what they may do to prevent or reduce it, and indeed to allow them to decide for themselves whether they choose to face the risk at all. When considering patient safety, this involves issues of communication, and consent, which are addressed in the next chapter on Consent.
The risks which this Report goes on to consider are those of transmission through blood, and blood products. The blood services of the four nations of the UK form a front line of our protections so far as future risks from blood are concerned. All have now adopted the same, systematic approach to their evaluation and management: a Risk-Based Decision-Making Framework which aims to ensure that the wellbeing of transfusion recipients is central to blood safety decision-making, as well as helping to align resources with health outcomes and to produce evidence-based decisions.[5] It applies eight general principles,[6] seeks to define when risks may be tolerable in light of the benefits gained by running them, and states a policy as to how they should be assessed. Where a risk is identified, this approach involves first identifying the options for dealing with it, next assessing these measures and the risk itself, and then addressing whether the risk is intolerable, tolerable or acceptable.[7] In the light of this assessment, risk management options are determined and scored so as to come to a recommended decision as to what should be done. Where there is insufficient evidence to make a risk-based decision it does not preclude the use of the “precautionary principle”.
The narrative which follows shows the value of a systematic approach to addressing risk. Readers will see that a system was needed, designed with careful unpressured forethought, agreement and patient involvement, which provided sufficient flexibility to allow for coping with the risks discussed here. A proper system to protect against future risks must be capable (as the Risk-Based Decision-Making Framework is) of dealing with the several different ways in which risks of different magnitudes can emerge. It has come too late to affect what happened: but it is encouraging to see that the transfusion services now have a much better system for dealing with risks arising from and through blood than was the case before the mid 1990s.
This chapter however ends with the simple message with which it began. Safety – of the health of populations, of groups within them, and of individuals within those groups – is the starting point. And that centrally involves recognising and reacting to risks to safety so as to reduce or eliminate those risks as far as is practicable.
The fundamental principle of patient consent can be shortly stated. Medical treatment can only be given to a person with their consent.[8] That consent must be informed: in other words, the patient must have been given sufficient information about the risks and benefits of treatment, alternative treatments and the right to refuse treatment. [9] That principle is well understood. It is founded in ethical norms: [10] in particular the principle of autonomy: “by knowingly considering, and then accepting rather than rejecting a proposed course of action based on adequate information, a patient expresses their autonomy and their responsibility for the decision, while also accepting the expertise of the clinician.”[11]
Since that principle has been so poorly respected in the context of the treatment with blood and blood products that has infected so many people,[12] this chapter considers the principle in a little more detail.
Consent is more than the patient simply agreeing to or refusing what is proposed, it “should be voluntary, denoting an absence of control by others, and informed, requiring sufficient information and understanding to allow autonomous choice. Three elements of consent therefore include agency (capacity), liberty (absence of coercion), and autonomy.” In considering coercion, “one can effectively coerce someone without intending to do so, particularly if one holds a position of power and operates within a context where the other person is disempowered by their circumstance or role.”[13]
If material risks are not explained, “the patient is denied an effective choice”;[14] if information about risks of reasonable treatment alternatives is withheld, “then the patient cannot make an informed selection and is more reliant on the paternalistic considerations of the clinician in choosing on their behalf.”[15]
The Inquiry’s medical ethics expert group told the Inquiry that “respect for autonomy has always been an ethical cornerstone of medicine”.[16] Autonomy involves the concept of self-determination (“that each of us has our own life that we should be free to fashion and shape as we see fit … each of us should be free to live our lives according to our own values and choices”[17]) and it may be said to embrace too the concept of dignity.[18] Not being informed “fundamentally undermines your autonomy because you are denied the opportunity of real choice.”[19]
In the 1970s interest in medical law and ethics was, the expert group said, renewed. The influential 1979 publication Principles of Biomedical Ethics[20] set out four principles: autonomy (protecting the rights of individuals to make their own choice); justice (fairness, equity and equality), beneficence (doing good); and non-maleficence (expected benefits should outweigh expected harms). In the UK, Professor Ian Kennedy’s highly influential Reith Lectures in 1980[21] called for a greater role for ethics and characterised the “so-called therapeutic privilege” (that a doctor may withhold information from the patient if in the doctor’s judgement it is not in the patient’s best interests to know) as “clearly a device created by doctors to do what is in the best interests of doctors”.[22]
These principles found their expression in guidance and other publications relevant to the time period under consideration by the Inquiry.[23] They were not new: as the ethical experts said, the principles are fundamental. Thus, a booklet produced by the Medical Defence Union (“MDU”)[24] in or around 1953 explained that: “It is not sufficiently widely known by practitioners that, in law, consent must be given by a patient before an examination can be conducted or treatment administered”.[25] The booklet continued:
“To obtain consent it is necessary for the practitioner to explain carefully to the patient in non-technical language the need for an examination to arrive at a diagnosis or decide on the line of treatment. The character and the likely results of the treatment should be outlined to the patient in such terms that he can appreciate fully what is proposed and what may ensure. A practitioner, aware of the uncertainties of treatment, should avoid sweeping promises; and should not minimise the risks that may be inherent in the procedure he proposes … The consent thus obtained must be genuine consent; not merely an apathetic acquiescence but a real expressed willingness by the patient to undergo the treatment after he had its nature, its risks and its objective clearly explained.”
The MDU’s 1966 memorandum Consent To Treatment began with a quotation from a 1912 decision by the US courts: “No amount of professional skill can justify the substitution of the will of the surgeon for that of his patient”.[26] It recorded the right of the patient not to submit themselves to medical treatment if they do not wish to do so. The MDU emphasised the importance of consent, and of informing the patient of the nature and effect of the treatment and its risks: “If an inadequate or misleading explanation is given there is the danger that the apparent consent obtained will be held to be ineffective.”[27]
In 1970 the British Medical Association (“BMA”)[28] published guidance entitled Medical Ethics.[29] This guidance said relatively little about informed consent[30] but it described the basis of the relationship between doctor and patient “as that of absolute confidence and mutual respect.”[31] It may be thought inherent in the idea of “mutual respect” that a patient be provided with sufficient information regarding the risks of treatment, and the availability of other treatments, to enable them to give properly informed consent.
In 1980 the BMA published its Handbook of Medical Ethics which expressly addressed consent to treatment in these terms: “The patient’s trust that his consent to treatment will not be misused is an essential part of his relationship with his doctor, but for a doctor to touch a patient without consent is an assault. Consent is valid when freely given if the patient understands the nature and consequences of what is proposed. Assumed consent or consent obtained by undue influence is valueless.” It explained that: “The onus is always on the doctor carrying out the procedure to see that an adequate explanation is given.”[32] An amended version of the Handbook of Medical Ethics published the next year added that “Doctors offer advice but it is the patient who decides whether or not to accept the advice.”[33]
In autumn 1981 the World Medical Association adopted the Declaration of Lisbon on the Rights of the Patients. These rights included “the right to accept or to refuse treatment after receiving adequate information”.[34]
In 1988 the BMA published a revised ethics handbook – Philosophy & Practice of Medical Ethics. This discussed consent, and the underlying ethical principles, in more detail than previous handbooks.[35] On consent, it said this: “The basis of any discussion about consent is that a patient gives consent before any investigation and treatment proposed by the doctor. Doctors offer advice, but the patient decides whether to accept it. Before a patient can consent the options have to be presented in such a fashion as to allow a decision to be made. Consent must involve the ability to choose.” Referring to implied consent (for example “in attendance for an inoculation which implies that the patient expects the inoculation”) the handbook noted that this does not absolve the doctor from explaining any risks.[36]
Addressing the question of paternalism, the handbook identified it as being “in direct conflict with the principle of autonomy”. Although “the concept of autonomy is not new, it is now becoming a central influence on the expectations of patients. In the past many patients would accept without question decisions made by their doctor. Today, patients are more critical.” The handbook identified “truth telling” as “another principle by which people address medical ethics”: “the doctor and the patient are bound by an unspoken, unwritten agreement which is based on the patient’s ability to trust his doctor. Truthfulness is therefore seen as important because it is a moral imperative in itself and on utilitarian grounds produces a good social relationship.”[37]
In August 1990 the Department of Health published a Guide to Consent for Examination or Treatment[38]: a similar guide (A Guide to Consent to Examination, Investigation, Treatment or Operation) was published in Scotland in October 1992.[39] These too emphasised the right of the patient to give or withhold consent and the entitlement of the patient to receive sufficient information in a way they could understand about any proposed procedure, possible alternatives and any substantial risks so that they could make a balanced judgement.
Medical Ethics Today: Its Practice and Philosophy was published in 1993 by the BMA as “a practical guide which reflects contemporary ethical thinking.”[40] It contained detailed guidance on the issue of consent. It referred to the relationship between doctor and patient as: “based on the concept of partnership and collaborative effort … the basic premise is that treatment is undertaken as a result of patients being actively involved in deciding what is to be done to them”.[41] It advised that “As a prerequisite to choosing treatment patients have the right to receive information from doctors and to discuss the benefits and risks of appropriate treatment options.”[42] Further:
“Some people see the purpose of consent as chiefly being the provision of a defence for doctors against legal liabilities … In the BMA’s view, respect for others and their rights lies at the heart of the issue of consent. A feature of our present society is the emphasis on the value and dignity of the individual. It is said that principles of inherent natural rights dictate that each person who is competent to do so should decide what happens to his or her own body. The patient exercises this autonomy by deciding which treatment option to accept. The decision is based on information given by the clinician. For consent to be valid, the patient must know what options are available and have the ability to choose.”[43]
In 1995 the World Medical Association’s Declaration of Lisbon was expanded to provide that:
The 1995 Declaration of Lisbon also created a right for the patient to receive information about themselves recorded in any part of the medical records and to be fully informed about their health status, including the medical facts and their condition.[44]
1995 also saw the issue by the General Medical Council (“GMC”)[45] of Good Medical Practice, which sought to articulate the fundamental duties of a doctor registered with the GMC. Those duties included: making the care of the patient the doctor’s first concern; listening to patients and respecting their views; providing information to patients in a way they can understand; and respecting the rights of patients to be fully involved in decisions about their care and to refuse treatment.[46]
The GMC published its first specific guidance on consent in November 1998: Seeking patients’ consent: the ethical considerations. This explained that “Patients must be given sufficient information, in a way that they can understand, in order to enable them to exercise their right to make informed decisions about their care.”[47]
Some of the evidence which the Inquiry has received suggested that clinicians’ approach to consent[48] in the 1970s and 1980s reflected a culture of medical paternalism. Whilst it is no doubt correct that, to some extent at least, “medical decision-making was previously paternalistic” and that it is “now recognised that decision-making should be shared and that informed patients should have the power to decide what happens to their lives”,[49] that is neither an excuse nor a defence for a failure to ensure that people treated with blood or blood products were given information about the risks of viral transmission, such that they could give (or withhold) consent on an informed basis. Nor does it justify the multiple examples which the Inquiry has heard of people being tested for HIV or hepatitis without their knowledge or consent.
Whilst guidance relating to clinicians has over time become more detailed, the underlying ideas and principles have not. The degree of articulation of those principles may have shifted over the years, but the principles themselves predate the events with which this Inquiry is concerned. Judged against stable and consistent “fundamental moral principles”, “past behaviours and practices, that may have been unchallenged or standard practice at the time, may still be considered morally questionable.”[50] Although “people may have been operating in line with contemporary moral norms, their actions can be challenged where we can identify relevant fundamental moral values which should have been respected, irrespective of time or place.”[51]
The descriptions given in the chapter on People’s Experiences show what too often happened: that people were not given adequate information about risks, or about alternatives; that too often doctors made decisions for, rather than with, patients; that clinical freedom was misunderstood as allowing doctors the freedom to decide what their patient’s treatment should consist of; and that the guidance this chapter has recorded as having been set out consistently since 1953 was not followed. It also demonstrates the consequences of this, not just in terms of the infections that followed but in the significant and destructive loss of trust that patients then had in their doctors.
Almost from the dawn of human civilisation, blood has held a special significance. Before the principles of circulation became known, societies appreciated that blood was critical to life. We speak of “lifeblood”. Or say “It’s in the blood...”
Blood has held a significance that goes beyond it being seen as necessary to sustain life. It has been associated throughout time with the way in which that life is lived; with the central character of a person. There has been a sense that personalities are linked to blood – “hot-blooded”, or someone who acts “in cold blood”.
It is an easy step from thinking that blood dictates human characteristics and behaviour to thinking that if only blood could be replaced by better blood it would benefit recipients. They might then show some of the desirable characteristics of the animal or human from which the blood came, or find their own illnesses cured. The origins of blood transfusion to improve health lie in this instinctive sense that blood can convey beneficial characteristics.
It can be easy to overlook the other side of the coin: that someone else’s blood may contain undesirable characteristics too.
If blood is taken out of the body it will in most cases quickly coagulate. If however it is mixed with a suitable anticoagulant it will settle in a test tube into three portions. At the top will be a straw-coloured fluid called plasma. This is the major component of blood by volume (about 55%). At the bottom will be tightly packed red blood cells (amounting to 45% by volume). Between them is what is known as the “buffy coat” (less than 1%). This contains platelets and white blood cells.

Red blood cells are produced in the bone marrow. What gives them their distinctive red colour is the iron in the haemoglobin they contain. This important protein carries oxygen from the lungs to all parts of the body, and carries carbon dioxide as a waste product away from the tissues and back to the lungs for oral and nasal exhalation. Though described as “cells”, red blood cells do not contain a nucleus, nor do they contain mitochondria. [52] They are very tiny – small enough to pass through the narrowest of blood capillaries. If red blood is lost, it may take some time progressively to replace the loss: to the extent that blood donors providing a pint (just over half a litre) of whole blood are not asked to donate again within 12 weeks (if male) or 16 weeks (if female).[53]
Platelets (thrombocytes) are fragments of bone marrow cells, which again contain no nucleus. They are naturally sticky, and play an important role in the control of bleeding, described further below.
White blood cells (leucocytes) help to fight infections and so help the immune process. They consist of granulocytes, monocytes, and lymphocytes.
Granulocytes[54] make up about two thirds of the white cells. They consist of three kinds: neutrophils, which engulf foreign particles such as bacteria, which they then destroy with their powerful digestive enzymes; eosinophils, which are concerned with parasitic infection, and with allergic reactions; and basophils, which are responsible for inflammatory reactions and produce compounds such as histamine and serotonin which coordinate immune responses.
Monocytes, which are the largest of the white cells, are the scavengers of the blood circulation. They go for the damaged red cells and larger particles often found around chronic infections, and are able to enter tissue spaces and clear from them the debris of both infections and the bodily response to them.
Lymphocytes are central to many of the Inquiry’s concerns. They play an important role in the immune system, more fully described below.
Plasma contains thousands of proteins, performing a wide range of functions. What has been described as the “classical plasma proteins” include albumin, clotting factors, immunoglobulins and fibrinogen.[55]
The clotting process is the body’s response to a loss or threatened loss of blood. It begins when the lining of a blood vessel is damaged. Platelets in the blood (contained in the buffy coat) are activated in a process which eventually leads to them sticking together in clumps to form a plug at the site of injury. Clotting factors respond in a cascade – always in the same order – to form fibrin strands from the fibrinogen in the blood. These strands strengthen the platelet plug: fibrin in effect sticks the platelets together in a way which prevents further loss of blood.
The essence of the immune system lies in its ability to recognise “self” from “foreign” and to tackle “foreign” material. A molecular structure which leads to an immune response is known as an “antigen”.[56] Two of the most important parts of this immune response, cells (lymphocytes) and antibodies (immunoglobulins), are found in blood.
Lymphocytes make up about 30% of the white cells. They are mostly very small and travel throughout the body, sampling the surrounding environment. They originate in the bone marrow, where they separate into two different classes: B lymphocytes and T lymphocytes. (The T indicates that this class of lymphocytes matures in the thymus, a small ductless gland just below the throat at the top of the chest, whereas the B indicates an origin in the bone marrow.)
T cells are classified into three main groups: killer cells, helper cells, and suppressor cells. Each T helper cell carries a number of molecular structures on its outer surface, including a T cell receptor.
Where such a T cell receptor recognises a specific antigen presented to it, it will bind with it. The interaction is like that of lock and key, initiating an immune response. There are a multitude of potential antigens, all different; but to meet them there is also a multiplicity of T cells, some of which will have the appropriate receptor to enable them to bind to the antigen.
When a helper T cell first locks on to an antigen, it proliferates into two general subtypes, one of which will activate killer T cells to bind with and kill the infected target cell, so as to begin its destruction; the other of which will cause B cells to proliferate, differentiate, and produce antibodies. The antibodies float free and themselves bind to and neutralise (or destroy) antigens.[57]
Following recognition of the antigen, the B lymphocyte not only rapidly produces copies of itself to produce more antibodies but also produces memory cells which can induce a secondary immune response if there is contact with the same pathogen in the future. These memory cells are important in speeding up the response to any future attack by an identical pathogen, which is necessary because the process just described takes quite a time to develop into an effective response.
Thus there are different parts to an immune response, mediated by different components of blood. There is the response in which T cells themselves attack and kill the foreign bodies carrying the relevant antigen (“the cell-mediated response”) and one in which the antibodies which the B cells have produced attack the antigens (the “antibody-mediated response”, also known as the “humoral response”).
In summary, the helper T cells (CD4 T cells) work by triggering a response when faced with an antigen, for example, from a pathogen. Killer cells (CD8 T cells) respond by attacking the tagged pathogen and neutralising it. Suppressor cells regulate CD4 activity, “turning it off” when sufficient immune response has been achieved.[58]
In a healthy individual, the proportion of CD4 T cells (which are more numerous) to CD8 T cells varies, but is generally between 1.5 and 4 to 1. This is described as a ratio of (for example) 1.5:1, or 4:1.
When a person is first exposed to HIV, a virus which attacks CD4 T lymphocytes,[59] there is generally a drop in the number of CD4 T cells, since HIV targets those cells and depletes their numbers. By contrast, CD8 T cells generally increase by around 40%, although their ability to neutralise the virus will wane over time as there are simply fewer CD4 T cells to trigger an effective immune response.
An inverted CD4:CD8 T cell ratio is thus an indication of serious problems: if HIV therapy is initiated in a timely manner, the ratio will generally return to normal. However, if it is delayed the body’s ability to create new CD4 T cells weakens, and if and when this happens the ratio may never normalise.[60]
Before there was certainty that a virus was the cause of AIDS, a significant sign that AIDS might be about to develop in an individual was such an inverted T cell ratio or a low absolute CD4 T cell count.[61]
In the mid 17th Century Sir Christopher Wren (the famous architect) used a hollow goose quill attached to a bladder to perform intravenous injections on dogs. There were apparently no ill effects. It was not long before his friend Richard Lower experimented with the direct transfer of blood between two dogs using a system of hollow goose quills and tubing.[62] That was in 1666.[63] The first transfusion was then attempted from an animal (a lamb) to a human (a boy suffering a fever), by Dr Jean-Baptiste Denis (physician to King Louis XIV) in France.[64] It was followed shortly after by a presentation at a meeting of the Royal Society by Richard Lower. In front of the lecture theatre he transfused the blood of a lamb into a human, Arthur Coga, who suffered from a malady. Arthur Coga survived without ill effect: history does not record what happened to the lamb.[65] Dr Denis conducted a handful of further transfusions, but one recipient died. The public outcry that followed resulted in blood transfusions being banned by the French parliament and the practice discredited.[66]
It was nearly 140 years later before the practice of transfusion began again. A significant number of maternal deaths occurred through haemorrhage during and after childbirth. In 1818 Dr James Blundell (an obstetrician) became interested in transfusion to treat postpartum haemorrhage which would otherwise prove fatal. He eventually succeeded and thereafter repeated the procedure.[67]
The first article about inherited bleeding disorders was published in 1803 and the term “haemophilia” was first used in 1828.[68] Samuel Lane at St George’s Hospital, advised by Dr Blundell, performed the first transfusion successfully to treat haemophilia in 1839.[69] Dr Blundell’s work was replicated in Edinburgh, with a successful transfusion to a woman with severe uterine bleeding in 1845.[70] All transfusions were direct – the donor being connected by tubing to the recipient with no intermediate bladder, or bottle, and no intermediate storage. There could be no storage for very long, since if blood were taken out of the body and left to stand for any length of time it would begin to coagulate.
Two significant advances occurred just after the start of the twentieth century. Success in transfusion had been hit and miss, since the recipient could react seriously, and sometimes fatally, to it. Then in 1901 Dr Karl Landsteiner discovered blood groups.[71] People’s blood can be classified as falling into one of four groups: A, B, AB, or O. Blood group A has A antigens on the red blood cells, with anti-B antibodies in the plasma; blood group B has B antigens on the red blood cells with anti-A antibodies in the plasma; blood group AB has both A and B antigens but no antibodies; and blood group O has no antigens but both anti-A and anti-B antibodies in the plasma. These differences mean that someone with blood group A cannot safely receive blood from someone with group B, and vice versa.
Because blood group O has no antigens, it may be given to anyone, regardless of their blood group, without being seen as foreign by the recipient’s immune system and creating a devastating immune response. It is known as the “universal donor” blood group. Almost half of the UK population has blood group O. Blood group AB is known as “universal recipient” because it has no antibodies.[72] Once the system became known it was apparent why a number of recipients had reacted so badly to receiving transfusions of blood, and doctors soon learned how to “group” blood, and to know what transfusions to avoid.
The second significant development was the discovery a few years later that sodium citrate could be used as an anticoagulant.[73] On 27 March 1914 came a first tentative use of citrated blood which had been taken from a donor shortly before.[74] The feasibility of indirect transfusion was thus established. This would eventually enable red blood to remain effective for around 21 days, during which it could be used for indirect transfusion.
The First World War led to further advances. The importance of keeping a fighting force on its feet, and treating casualties to preserve life as far as possible, led to direct transfusions being conducted near the front line. Though citrated blood was not used extensively, its use did increase especially towards the end of the War.[75]
A further lesson from war was that the principal cause of death following a severe wound was not so much loss of red blood, but the effects of post traumatic shock. Shock caused by haemorrhage or overwhelming infection is characterised in most cases by a weak pulse, low blood pressure and cold sweaty skin. Its effect is to reduce blood flow through the small vessels or capillaries. Circulating volume is not maintained. Without that, the organs of the body may lack the oxygen necessary to avoid being damaged irretrievably. The use of plasma counteracted these symptoms.[76] This was centrally because of the albumin present in significant quantities in plasma. This acted as a volume expander. Giving a seriously wounded serviceman plasma thus was more effective at first to maintain life than restoring the lost red blood cells to his circulation.
In due course, this led to a focus on the use of plasma on its own to treat traumatic shock, and in turn this led to the use of albumin once that could successfully be separated from plasma.
Following the First World War, and the recognition that transfusions could keep troops alive, there was fertile ground for the development of the use of transfusion in civilian medical emergencies. The first organisation of blood donations for transfusion in the UK began in 1921 when Percy Lane Oliver, as honorary secretary of the Camberwell Division of the British Red Cross, organised a panel of donors who were willing to donate their blood voluntarily at hospitals around London. This became the London Blood Transfusion Service. It served only a handful of central London hospitals – blood was taken directly, donors had to live near to the transfusion centre, and the experience for the donor in giving blood, lying alongside or close to a recipient who was often in pain could be unpleasant. Nonetheless, Percy Lane Oliver’s enthusiasm was such that after he lectured at St Thomas’ Hospital on 11 November 1924 his system was adopted by the Red Cross for use across the country. In 1926 the British Red Cross transfusion service formally began, limited to urban areas at first because it depended on “walking donors” giving their blood directly.[77] In 1929 in Edinburgh, Jack Copland inspired a group of walking donors to give transfusions of their blood to the Royal Infirmary in Edinburgh.[78]
It took another war, after another ten years, for the next significant development to occur in the UK. During the Spanish Civil War, Frederic Durán-Jordà established one of the first blood banks in Barcelona. Blood was transfused indirectly, having first been donated into glass bottles containing anticoagulant, and stored in a “bank” from which the bottles might be drawn to treat casualties.[79] In 1939 Frederic Durán-Jordà fled to London, where he published about the Barcelona Blood Service in The Lancet and shared his knowledge with Dr Janet Vaughan who was influential in creating four transfusion depots around London, administered by the Medical Research Council (“MRC”), in readiness for the expected war.[80] These were followed by regional depots in 1940.[81] The Scottish National Blood Transfusion Association was established in January 1940 with five regional blood transfusion centres.[82] The Army Blood Supply Depot was also set up, with a donor pool of some 5,000 at the start of the war and over half a million donors by the end of the war.[83] Indirect transfusion, and short-term storage in a blood bank, had become established.
By the start of the Second World War plasma had long been separated from whole blood. Indeed, frozen plasma was first developed in 1925[84] and plasma itself was first used in the treatment of haemophilia a year earlier.[85] However, the volume of plasma (or thawed fresh frozen plasma) was likely to be unsuitably large for many purposes. Its volume often hindered easy transport in bulk. This was especially the case where it was the albumin it contained which was essentially what was needed initially to keep troops with serious wounds alive. By the Second World War, however, it could be freeze dried, which made it more transportable, easier to store without deterioration, and more easily usable.[86]
In 1941 the Treasury War Emergency Committee decided to finance two facilities in the UK to prepare freeze-dried human plasma, to take advantage of these benefits. One of these was to be situated “in the north”.[87] Thus a unit for drying plasma was constructed in an underground site at the Royal Infirmary Edinburgh; and production near London centred on Cambridge (later relocated to Elstree).[88]
1941 saw a further major advance, which together with freeze drying improved the ease of supply of blood derivatives to theatres of war. In the US, Dr Edwin Cohn and his team at Harvard discovered how the constituent parts of plasma could be separated for use. His process, known as “Cohn fractionation” was developed then, and its essential principles remain in use to this day.[89] He knew that what uniquely distinguished one protein from another was its solubility under different conditions – almost to the extent of this being a fingerprint. Using ethanol allowed the process to be conducted at a low temperature, and minimised the risk of bacterial growth. In a five stage process, some of the proteins would become insoluble at each stage. They would drop to the bottom of the fractionating vessel (or in a centrifuge be spun to the sides), leaving a fluid containing the remaining proteins in solution – the supernatant – to pass to the next stage of fractionation. “Cold ethanol fractionation” deposited fibrinogen at its first stage, together with two proteins present in such small quantities as to be described as “trace proteins” – which became known as Factor 8, and von Willebrand factor. The next stage saw the deposit of Factor 9 and after further stages the last stage would leave albumin.[90] Dr Cohn’s discovery of his fractionation process was timely: the albumin which was extracted, in concentrated form, saved many lives in the immediate aftermath of the attack on Pearl Harbour.[91]

Fractionation by the Cohn process was enthusiastically adopted in both the Edinburgh and Cambridge centres before the end of the Second World War. The principal aim of it was to produce the two fractions of (then) greatest therapeutic interest – immunoglobulins and albumin. Clotting factor proteins came to prominence later.
The intense demands of warfare, and escalating use of transfusion during it, alerted administrators, scientists, researchers and clinicians to the fact that a transfusion could do harm as well as good. By the end of the Second World War, if not earlier, this had become well established by experience. More is said about this in the chapter Knowledge of Risk Before 1970: it is sufficient here to note that by 1944 The British Medical Journal was drawing attention to the risk that transfusion could transmit hepatitis;[92] and on 19 August 1946 Dr William d’A Maycock, who had become the consultant advisor in blood transfusion to the Ministry of Health, recorded in a letter that he agreed that “users must be told that [plasma] is a potentially lethal fluid which should be used with discretion.”[93] In October 1947, the Journal of the American Medical Association, the prestigious US medical journal, contained an article which ended by observing that: “Plasma, as well as other forms of transfusion therapy, should be administered only when the clinical indications are absolute.”[94]
In December 1964 a circular from the Scottish Home and Health Department echoed the same theme: “All blood for transfusion must be regarded as potentially contaminated … The most important transmissible disease in this country is homologous serum jaundice or serum hepatitis … No transfusion should be undertaken unless the benefits outweigh the risk of hepatitis.”[95] Dr Jean Grant, the director of the regional transfusion centre in Oxford wrote the following year: “The practitioner should satisfy himself that it is really necessary to give blood and that no other treatment would be equally efficacious even though it might take a little longer to achieve results.”[96]
Just over 30 years later, similar words were used by Sir Colin Walker, when as chairman of the National Blood Transfusion Service he wrote in a foreword to a booklet celebrating 50 years of the blood transfusion service in the UK that “Our blood supply is amongst the safest in the world but, even so, medical advice is always likely to be that the best transfusion is no transfusion.”[97]
Hepatitis is an inflammation of the liver.[98] It may be caused in a number of ways: by infection (most commonly viruses, but also bacteria and parasites), by medication, or by a high alcohol intake. It may be the result of a fatty liver (steatosis),[99] of autoimmune disease or some metabolic disorders.
Inflammation of the liver is diagnosed by a blood test which measures the levels of certain enzymes in the blood: ALT [100] and AST. [101] These are released when cells in the liver are damaged or start to die. Though a low normal level is always present, hepatitis is suspected when one or more of these enzymes is elevated above the normal range. However, a reading above the normal does not identify on its own what the likely cause is: a wide range of factors may cause a temporary elevation of ALT or AST levels; “an evening’s sustained drinking” may do so, for instance. For that reason, where there is an elevated reading, much will depend upon the extent to which the level is higher than the normal range, and after a short period a further test still shows an elevated reading. Further testing to help discover the cause of the hepatitis usually involves a panel of blood tests, ultrasound imaging of the liver, and (in some cases) may involve a liver biopsy.
There are five hepatitis viruses – lettered A–E. Of these, the two most important viral causes of hepatitis are Hepatitis B virus and Hepatitis C virus; Hepatitis D only occurs if Hepatitis B is present.[102]
Both Hepatitis B and C can range in severity from being very mild, where an individual has no significant symptoms in the six months after infection and clears it naturally to being so severe that the liver can no longer carry out its essential functions and fails. If it fails there is a high risk of death. A liver transplant may be the only solution where there is liver failure.
Both Hepatitis B and Hepatitis C are transmissible by blood. Hepatitis A is sometimes transmitted by blood, but its normal route of transmission is oro-faecally. It comes via environmental factors, such as contaminated food or water.
The letters “A”, “B” and “C” were not used until around 1970 (for A and B) and 1988 (for C). Before 1970 no distinction was made between Hepatitis B and Hepatitis C. Together they were termed “serum hepatitis” (which indicated that they were carried by the serum (or plasma) component of blood). By contrast, what is now known as Hepatitis A was termed “infectious hepatitis”, which indicated it was not usually transmitted in that way.
By 1944 it had become well known that serum hepatitis could be transmitted by blood (this might be either by sharing a needle which had been used to vaccinate a number of people in turn, or by transfusion from one person to another).
There was no laboratory test for either part of serum hepatitis (indeed, it was not recognised that there was more than one constituent virus) until the discovery of an antigen associated with serum hepatitis in 1965.[103] When this was followed in 1970 by the identification of a virus-like particle by Dr David Dane of the Middlesex Hospital (known, therefore, as “the Dane particle”) it became known as Hepatitis B to distinguish it from infectious hepatitis, which then became known as Hepatitis A.[104]
After Hepatitis B was isolated, and a test for it developed in the early 1970s it was progressively realised that it had not been the sole cause of serum hepatitis. A larger component was a virus which had not yet been precisely identified. Since this was neither A, nor B, it became known as non-A, non-B Hepatitis (virus) (“NANBH”). Since compromised liver function can be tested for by measuring ALT and AST levels, and the presence of Hepatitis B infection in the past could be shown by the presence of anti-HBc,[105] NANBH was established as a diagnosis of exclusion. Where liver enzyme counts taken on at least two occasions close in time were elevated, tests for Hepatitis A or B were negative, and there was no other more obvious explanation for the elevation, then it was present.
The Hepatitis C virus was cloned in the US; the Chiron Corporation announced on 10 May 1988 that it had achieved this. The scientific details of its achievement were not fully released until 21 April 1989. Tests for the virus were then developed, NANBH stopped being used as a label, and screening blood for the virus became possible. The history of Hepatitis C screening is the subject of a later chapter.
Together, Hepatitis B and Hepatitis C viruses are amongst the leading causes of mortality globally, responsible for more deaths each year than malaria or HIV.[106]
The first six months of infection by either Hepatitis B or Hepatitis C is known as the “acute phase”; those infections which last for over six months are known as “chronic”. In this context, the words “acute” and “chronic” are no indication of the severity of symptoms. They are simply a measure of the length of time for which infection has persisted, whether the symptoms are significant or not. However, long-term (chronic) hepatitis infection is likely to lead to progressive scarring of the liver (fibrosis) which can lead to cirrhosis (a nodular form of scarring) and then an increased risk of liver cancer (hepatocellular carcinoma).
About 180 million people are infected worldwide: it is likely that the disease has been around for over 3,000 years. The onset of Hepatitis C can be insidious. The body can clear the disease naturally. When it does so, this usually occurs within the first six months after infection. Where chronic, its effects may take a long time to show. The symptoms are unspecific, presenting at first like many other illnesses. They may simply be understood by a patient as the ravages of time on the human body, and in particular cases (where a woman is infected around the time that she gives birth) have been ascribed to the tiredness that comes with childbirth, and the strains of bringing up children; and later attributed to the menopause and then to increasing age. However, in a significant number of cases, cirrhosis develops. Whereas less than 20% of Hepatitis C patients experience the typical symptoms of acute hepatitis, such as malaise, fatigue and jaundice, the virus can persist in the liver and silently begin to cause liver inflammation and scarring. After 20 years, approximately 20 to 30% develop cirrhosis. After 30 years it is 40% and after 40 to 50 years 60%. (Roughly, therefore 1 to 2% per year). Between 2 and 8% a year of those who have cirrhosis will develop liver cancer: successful treatment for Hepatitis C will reduce, but not eliminate the risk of cancer to around one third of these figures.[107]
There are eight genotypes of Hepatitis C, of which genotype 1 is the most common globally. In the UK, genotypes 1 and 3 each account for approximately 40% of the infections. Patients with genotype 3 tend to progress more rapidly to fibrosis and cirrhosis, and have a higher prevalence of severe steatosis (fatty liver) and a higher incidence of liver cancer. Early treatments for Hepatitis C were based on interferon: these genotypes responded differently, so the choice of treatment and its duration depended upon them. Genotypes remain of some, though diminishing, importance now that modern treatments are active across all genotypes.[108]
Where there is cross-infection between HIV and Hepatitis C, the disease progresses more quickly to fibrosis. The likelihood of spontaneous clearance is reduced. Sustained virological response (or cure) after ribavirin combination therapy was significantly lower in HIV co-infected individuals, particularly those with genotype 1 Hepatitis C.[109]
Treatment was initially, in the early 1990s, by interferon, then interferon coupled with ribavarin, an antiviral. In the restrained language sometimes used in medical reports, it is said that this treatment was often “poorly tolerated”. The experiences described in the chapter on People’s Experiences give more colour to this, and set out just how brutal and destructive earlier treatments often were. As explained by the Hepatitis Expert Panel adverse events associated with interferon and its toxicity include a range of infections (such as bronchitis, respiratory infections, herpes, viral and bacterial infections, skin infections, endocarditis, otitis externa), serious complications (such as thrombocytopenia, immune system disorders and sarcoidosis, thryoiditis, rheumatoid arthritis, endocrine disorders, metabolism and nutrition disorders) and psychiatric symptoms and disorders (including depression, anxiety, insomnia, aggression, mood alteration, emotional disorders, decreased libido, suicidal ideation and suicide, hallucinations, psychotic disorder, mania and bipolar disorders).[110] Ribavirin could also cause significant side-effects.[111]
Between 2014-15, direct-acting antivirals (without either interferon or ribavirin) were developed. These are more effective, cheaper, can be taken orally in tablet form, and have far less by way of side-effects, and require a shorter period of treatment.
There is now a worldwide push to eliminate Hepatitis C altogether. The current aim in the UK is to eliminate Hepatitis C infections by 2025.
In contrast to Hepatitis B,[112] Hepatitis C is only rarely transmitted by sex: there are some, but few, cases which have been reported to the Inquiry where this has happened. It is usually transmitted by blood – shared needles, razors, toothbrushes or in childbirth; and may be transmitted vertically by mother to child during pregnancy.
Hepatitis C is more easily transmissible than HIV. A small amount can contaminate a whole pool of blood, and it is more difficult to eliminate. Dry heating of blood products at 80°C for 72 hours eventually proved effective in the UK to destroy Hepatitis C infections, whereas lesser heat for a lesser time was sufficient to eliminate HIV.[113] Hepatitis C is also highly resistant to chemical and physical methods of elimination, can survive for months in the frozen state, and withstands repeated thawing and refreezing.
In very young children (under the age of five) only about 10% would have symptoms or signs of the disease in the first phase of infection. In older children and adults between one fifth and one third have symptoms or signs. Symptoms could include nausea, loss of appetite, in particular fatigue, and vague abdominal pain. It could involve a skin rash, muscle aches and joint pains. There might be a dull pain in the right upper quadrant over the abdomen. Symptomatic patients usually had jaundice (yellowing of the skin), yellowing of the eyes and dark urine. Signs of the infection during the acute phase might include jaundice, tenderness over the liver, and a patchy red rash over the trunk or whole body.[114]
Where the infection becomes chronic many patients suffer from neurocognitive symptoms including fatigue, anxiety, depression, “brain fog”, attention deficit and impairment of memory. These symptoms are associated with a low level inflammation in the brain, and with functional changes which are identifiable. They may last even beyond successful treatment. There can be a skin rash and peripheral nerve damage, and a loss of sensation in the fingers. Again, any nerve damage may not improve after treatment. Hepatitis C can also lead to a wide variety of other health conditions and complications.[115] If the hepatitis leads to advanced liver disease, the loss of liver function and increasing pressure in the abdominal veins causes a variety of symptoms. They include abdominal swelling due to the collection of fluid (“ascites”),[116] jaundice, confusion and coma (known as encephalopathy), oesophageal varices, which are essentially varicose veins in the gastrointestinal system which may rupture and bleed, fatigue, breathlessness, and a susceptibility to bruising due to a loss of clotting factors. These symptoms and signs are associated with a limited life expectancy unless there is a transplant.[117] Many of the symptoms to which Hepatitis C infection led in individuals are described in the chapter on People’s Experiences. There are also rare, but serious, complications associated with Hepatitis C such as kidney damage (which can lead to kidney failure and require dialysis) and lymphoma.[118] Further information about the range of other health conditions or complications that can be caused or contributed to by hepatitis can be found in the Expert Report to the Infected Blood Inquiry: Hepatitis.[119]
An estimated 257 million people are living with chronic Hepatitis B infection worldwide and it has been found in human remains up to 4,500 years old. The symptoms of Hepatitis B are similar to those described for Hepatitis C. It is more likely than Hepatitis C to produce jaundice, and symptoms, in its acute phase. There are eight recognised Hepatitis B genotypes but, unlike Hepatitis C, their clinical relevance is relatively limited. Where Hepatitis B infection occurs in infancy, it is estimated that between 15 to 40% of people infected will develop cirrhosis during their lifetime. If infected in early adulthood, the virus is usually present at a high level, but in its chronic phase does not cause liver inflammation or damage. However, this phase (known as the immune tolerant phase) is of variable duration, and though it can last decades, over time patients develop liver injury as the immune system interacts with the virus (the immune active phase).Liver injury may thus persist and cirrhosis develop. It is not yet possible to cure Hepatitis B. There was no treatment until interferon started to be used experimentally in the 1980s and was approved for use in 1992. Direct acting antivirals are now used but with very few exceptions have to be taken for the rest of the person’s life: once chronic, hepatitis B is almost always life-long. Most people with chronic Hepatitis B are recommended to have six monthly testing (usually involving an ultrasound of the liver and an alpha-fetoprotein blood test) due to the risk of advanced liver disease and cancer.[120]
39 million people are estimated to have died worldwide as a result of HIV infection; at least 16 million have become orphans as a result; and nearly 80 million people worldwide have been infected. At least 36.9 million people worldwide are currently living with HIV infection. HIV exists in two types – HIV-1 and HIV-2 – with HIV-1 being responsible for the majority of infections worldwide and it is HIV-1 with which this Inquiry is concerned.
HIV (Human Immunodeficiency Virus) is not AIDS. HIV attacks the cells that control the body’s immune system and by damaging it compromise the body’s ability to fight infection. This renders the body vulnerable to life-threatening infections. AIDS is a failure of the immune system, manifested by a collection (syndrome) of infections which are a consequence of infection by HIV. HIV infection passes typically through three phases: an acute phase (in which the viral load is particularly high). Then a chronic phase which may well be asymptomatic, but during which the CD4 T-cell count declines.[121] Third comes the AIDS stage. Because the immune system is less effective, some infections which would normally be suppressed can take hold. Characteristic opportunistic infections which occur in the presence of HIV infection are pneumocystis pneumonia and Kaposi’s Sarcoma, a form of skin cancer. There may often be candidiasis (thrush/fungal infection), herpes diseases, histoplasmosis, cytomegalovirus, HIV-related encephalopathy, Burkitt’s lymphoma, wasting syndrome and tuberculosis. 23 clinical conditions, including opportunistic infections, were recognised in 1986 by the CDC as “AIDS defining”.[122]
HIV is a blood-borne infection, and may be transmissible by sex, though not by kissing or social contact. It is less readily transmissible than is Hepatitis C, and more easily inactivated by heat treatment.[123]
AIDS first came to attention in the western world after 5 June 1981 when the CDC reported in the Morbidity and Mortality Weekly Report that there was a strange disease of the immune system in five young gay men in San Francisco. It was not then labelled AIDS, but plainly serious symptoms had been caused by a failure of the immune system for some reason. Later it was discovered that HIV infection had most probably begun before 1981 – in the US in 1978, in the UK in 1979: though the first AIDS patient in the UK was identified as such in December 1981.[124] There is a long period between infection and AIDS becoming manifest.[125] Without treatment, the life expectancy after the occurrence of the first AIDS defining event (or the reduction of the CD4 cell count to below 200/uL) is very poor, usually around two years.[126]
Treatments began experimentally with AZT in 1986. There were very serious side-effects, with the dose used in the early trials twice that now licensed. Some of the side-effects were long-lasting, including lipodystrophy (fat redistribution disorder), lipohypertrophy (fat accumulation), lipoatrophy (subcutaneous fat loss), peripheral neuropathy, chronic liver disease, exocrine pancreatic deficiency, low bone mineral density and chronic kidney disease.[127] There was no other known means of treating the HIV infection itself, although some of the symptomatic opportunistic infections which occurred could be individually treated – for instance, pentamidine could be used to mitigate the effects of pneumocystis pneumonia. Treatments focussed on the way in which, through the activities of enzymes, the HIV virus attacks a CD4 T lymphocyte. Some therapies aim to prevent entry of the virus into the host cell in the first place (entry inhibitors). Some aim to prevent the enzyme replicating a strand of its RNA to form a double strand of DNA (nucleoside reverse transcriptase inhibitors “NRTIs”). Some aim to prevent the viral double strand becoming part of the host cell DNA (integrase inhibitors), some aim to prevent the DNA of the host cell assembling building blocks of protein to form new proto-virus particles, which might go on to infect further cells (protease inhibitors) and some aim to stop the viral replication cycle (non-nucleoside reverse transcriptase inhibitors). Ever since the mid to late 1990s a combination of three drugs (usually two NRTIs plus one other) have been used in antiretroviral therapy (“ART”) – this is known as HAART treatment, the “HA” standing for “highly active”.[128]
Although efforts continue, HIV infection cannot currently be “cured”. But, with treatment, then assuming resistance to that treatment does not build up, and that the effect of highly active treatment is to diminish the possibility of the virus mutating, viral load can be reduced to undetectable levels. If undetectable, it is untransmissible. The government has pledged to end new HIV infections by 2030.[129]
Acute HIV infection is frequently undiagnosed or misdiagnosed because the non-specific nature of many of the symptoms and signs mean that it may be confused with other viral infections such as glandular fever (Epstein Barr virus). Accordingly, a diagnosis of HIV infection is rarely made without specific testing. A proportion of people will develop symptoms during early HIV infection, most frequently, a raised temperature, sore throat, mouth ulceration, enlarged lymph nodes, aching muscles and joints, and tiredness. A short-lived faint pale pink rash is sometimes seen. Nausea, diarrhoea and weight loss can occur. Neurological symptoms are common and may include headache and aversion to light. In rare cases there may be signs of meningitis or of encephalopathy. In most people these illnesses last up to three weeks and resolve on their own. Without treatment, most people with HIV infection experience a gradual decline in CD4 count over a period of approximately eight to ten years before the development of symptomatic disease. People who begin treatment late in the course of their HIV infection may suffer severe inflammatory symptoms in addition. Even with effective antiretroviral treatment, people with HIV have higher levels of multimorbidity occurring at a younger age than those who are HIV negative. Frailty and its associated disabilities appear to occur at a younger age in people with HIV. Leading causes of hospital admission of people with HIV in Europe in 2017 included respiratory illness, psychiatric conditions, and cardiovascular, renal and neurological disorders. Data from the UK show 75% of those living with HIV have at least one other long-term condition including mental health conditions, hypertension, lipid disorders and diabetes.[130]
For people coinfected with HIV and one or more hepatitis viruses, the likelihood of spontaneous clearance of Hepatitis B and Hepatitis C decreases and Hepatitis B and Hepatitis C progress more quickly. Interferon-based treatment for Hepatitis C was less effective with HIV, leading to longer treatment and a higher risk for cumulative interferon and ribavirin toxicity. Treatment for Hepatitis B that can be taken with HIV treatment was not available until relatively recently. Treatment options are still poor for people infected with Hepatitis D as well as Hepatitis B and HIV. For people coinfected with more than one hepatitis virus, there is an interaction between them and if one is successfully treated another may flare. For people coinfected with more than one genotype of Hepatitis C, a genotype present at low levels may re-emerge after treatment of other coinfecting strains, particularly with the older treatments.[131]
Haemophilia is usually inherited. Inheritance is gender-linked: it is much more common for men to suffer than women. It is a clotting disorder. Some proteins are central to the process by which blood clots. Most are known as clotting factors. People vary in the amounts of these factors in their blood. The average level in humans is 100%. [133] There are thus many who have a level in excess of 100%. However, if someone has less than 1%[134] of Factor 8[135] he[136] is usually classed as having severe Haemophilia A. If he has less than 1% of Factor 9 he is usually classed as having severe Haemophilia B. For moderate Haemophilia A or B the level is between 1% and 5%; for mild, between 5% and 30%.[137] Rather than have an absence of Factor 8, a person may lack the desired level of a protein (von Willebrand factor) which is necessary to help Factor 8 function: this is von Willebrand disorder. Its absence is not a gender-linked characteristic. Accordingly, women will experience its absence as often as men.[138] The consequence of lacking von Willebrand factor is very similar to that of lacking Factor 8.[139]
Though the response to a lack of clotting factor inevitably varies from person to person, in the absence of treatment, people with severe haemophilia will bleed spontaneously, sometimes up to two or three times per week. By contrast, spontaneous bleeding is rare in those who have mild haemophilia: rather, they will bleed excessively only after accidents, injuries, surgery and dental extractions.
Though a common image of haemophilia is of a person bleeding uncontrollably and externally from a small, minor wound, this is far from the usual case. Bleeding is internal: usually into joints and muscles, but more seriously still into the gut or the brain.[140] Where blood collects in a joint it begins to destroy parts of the lining of the joint, the synovium, which causes it to swell and then tear, in turn causing more swelling until it “resembles a sponge laden with blood”[141] making it yet more liable to further bleeding, and causing the joint to become a “target joint”. This leads to arthritis – painful, stiff joints.[142] That in turn causes serious immobility as well as pain. Being immobile compromises life. The consequence is that without treatment, a person with severe haemophilia had a life expectancy in the twenties before the 1950s,[143] and only a little more than that by the late 1960s.
A person with severe haemophilia would typically be diagnosed in early infancy, as mobility developed and joints were banged. From then on (until treatments improved) life was far from easy. Schooling was fractured by the need to go to hospital to treat bleeds – as many as one or two a week, losing one or two days’ education.[144] It was thus more difficult for those with severe haemophilia to get good qualifications. Earning a living was affected by the need for frequent spontaneous absences from employment. Many jobs were manual, which were best avoided by someone whose joints and muscles might suffer all the more if he were to do them.
Post-war treatment focused on restocking the bloodstream with enough Factor 8 or 9 to meet the immediate need to stop a bleed, because the underlying problem is a deficiency of clotting factor. Transfusion of whole blood was an option. The adult human body has eight or nine pints of circulating blood. To raise the level of, say, Factor 8 in the whole bloodstream from 1% or 2% to a level of 25% (which usually would be just sufficient to resolve most immediate bleeding problems)[145] would obviously require a large additional volume. That could not easily be provided without imposing a huge strain on the heart. Further, the donation used might not itself have as much as the average 100% of relevant factor: it was difficult, therefore, to titrate a dose appropriate to the recipient. The process took time, and could only be done in hospital. It would never be done in advance, but rather in response to a major bleed. The patient would have to get, or be brought, to hospital whilst bleeding internally.
Blood consists of three main parts: red blood cells (approximately 45%), plasma (approximately 55%), with the remainder being composed of platelets and white blood cells.[146] If an appropriate anticoagulant is applied to a phial of blood and it is allowed to settle, the platelets and white blood cells form a “buffy coat” between the red cells below and the straw-coloured plasma above.
Whereas donated blood had historically a useful life of 21 days after donation,[147] plasma, if frozen at the point of donation, could last for several months or even longer. Fresh frozen plasma (“FFP”) was therefore often used to provide the necessary clotting factors. The volume needed was less than the volume of whole blood. It was easier to handle. But the process still took time.
Preparations of clotting factors derived from cows or pigs were often used;[148] and sometimes the venom of a Russell’s viper (also known as Stypven), but so far as this was concerned, because of its toxicity it could not be transfused and could only be injected topically to stop a bleed into a joint.[149] Gradually greater and greater use was made of clotting factors derived from human plasma.
Plasma contains proteins. Early in the Second World War, Dr Edwin Cohn had developed ways of separating plasma into separate protein fractions, by treating whole blood with anticoagulant, separating off the plasma, and “fractionating” the plasma under varying conditions of acidity and proportions of ethanol so as to separate one fraction of it from another.[150] It proved possible to freeze-dry fractions which contained Factors 8 or 9. In 1957 The Lancet was able to describe some of the development,[151] which led to the preparation of a concentrated form of Factor 8, then known as antihaemophilic factor (“AHF”).[152] Freeze-dried granules of this could be mixed with sterile water to reconstitute what has been described as “dreadful soups and thick creamy stuff”.[153] The volume needed was still regarded as challenging.[154]
From around 1968, Factor 8 concentrate was produced under the aegis of the Lister Institute at Elstree and Oxford and by the Blood Products Unit in Edinburgh (renamed the Protein Fractionation Centre in 1970);[155] Factor 9 was produced in Oxford. Until about 1974, Factor 8 concentrate contained large amounts of protein (in particular fibrinogen) other than the protein of interest. Fibrinogen is not readily soluble, and the dose needed for injection was usually greater than 100 ml, making the early Factor 8 product far more suitable for administration in hospitals than at home.[156]
When FFP was slowly thawed under certain conditions of acidity and concentrations of alcohol, a sludge dropped out of the solution. In 1959 Dr Judith Pool at Stanford University discovered that this “cold-insoluble precipitate contains considerable quantities of the plasma antihemophilic globulin”.[157] It became known as cryoprecipitate. The “supernatant” (the solution which remained) contained many of the other proteins which were in the plasma. When this was further fractionated, Factor 9 dropped out of the solution too.[158] The great advance for which Dr Pool was then responsible came in 1965 when she realised that plastic bags (now increasingly used for transfusions in place of bottles[159]) could be used in a closed, sterile system to hold separated out cryoprecipitate, which could then be stored and used by blood banks.[160]
Cryoprecipitate provided a greater quantity of clotting factor in a smaller volume. Where derived from a pool of different donors, the concentrations of this factor in the pool would tend towards 100%, because of the natural averaging out that comes with numbers of individual donations of differing percentages. Cryoprecipitate could be given as the product of a single donation, rather than pooled. Where there were pools they were small: they did not need to be large. Cryoprecipitate became the mainstay of treatment for Haemophilia A before the mid 1970s. It had drawbacks: it was usually kept in a hospital deep freeze, had to be raised very carefully to around 4°C, and transfused into a vein slowly. It thus typically[161] involved attendance at hospital to administer it, and the process could take a number of hours to complete. Where it came from a single donor, there had to be a presumption that there might not be enough clotting factor, because it was not known how great a concentration of it was contained in that particular donation. It tended to be used to treat bleeds which had led to hospitalisation, after the event, rather than administered in advance to provide a sufficient level of the necessary factor in the bloodstream to deal with potential bleeds as and when they might arise. Because the precipitate or sludge from which the Factor 8 or 9 was drawn contained a number of other proteins, it could in a number of cases provoke an adverse reaction from the immune system of the recipient, which might produce “inhibitors”. These inhibitors limited the effectiveness of the “foreign” Factor 8 or 9 protein.
Cryoprecipitate was enthusiastically (and rightly) hailed as a breakthrough in treatment. For instance, Dr Peter Jones wrote in 1967 in a letter to The Lancet that “Cryoprecipitate is now the method of choice in treating bleeding episodes in patients with haemophilia, but, when not available, adequate therapy with fresh frozen plasma is possible and can be made relatively safe”,[162] and returned to the same theme of praising cryoprecipitate in July 1972 when he wrote that: “Thirty years ago most haemophilics died of exsanguination in childhood. Today they can expect to live a normal life-span.”[163] He attributed this increased life expectancy to the identification of Factor 8, the organisation of the blood transfusion services post war – and to cryoprecipitate.[164] Commercial concentrate was to be used in the management of severe bleeds not as first choice, but as second best to cryoprecipitate: to be used “when insufficient cryoprecipitate is available”.[165] By 1977, with by now over ten years’ experience of its use, he remained of the view that cryoprecipitate had made a significant difference to the advantage of patients – talking of both cryoprecipitate and freeze-dried concentrates in the same breath as having made a difference, but then pointing out that Factor 8 concentrate was not without its problems, principal among which was that it was a significant cause of hepatitis.[166]
This enthusiastic embrace given to cryoprecipitate was echoed both contemporaneously and in retrospect by other clinicians. Thus Dr Elizabeth Mayne described its advantages amongst which were “efficacy, low donor exposure, simplicity of manufacture” set against some disadvantages; its discovery “transformed Haemophilia treatment”.[167] Even by 1990, after concentrates had become very widely used, she summarised her opinion as being “the selection of mode of treatment depends upon the category or type of patient concerned. In respect that cryoprecipitate and Factor VIII concentrates are both efficacious treatments, preference of the one over the other depends on the age, the severity of the haemophilia and whether the patient is on a self-treatment programme, or requires major or minor surgery.”[168] Two years earlier she had expressed herself more enthusiastically still: in a profile of haemophilia management in Northern Ireland she described how “In 1967 a milestone occurred; a revolutionary concentrate was produced called ‘cryoprecipitate’. It was prepared from single plasma donation according to the methodology discovered by Poole, 1965 … the patients were ecstatic about the new treatment. A simple dental extraction was normalised and no longer constituted a major ordeal necessitating many weeks in hospital.”[169]
Some haemophilia clinicians have, in their written and oral evidence to the Inquiry, identified a number of disadvantages to cryoprecipitate: including that it was less effective clinically than concentrate, it was laborious to reconstitute, it had to be stored in deep freeze and was therefore not suitable for home treatment; and it caused side effects.[170] However, whilst it is undoubtedly correct that cryoprecipitate was more laborious to use, it could be used, and had been used, to raise Factor 8 levels. Side effects were for the most part transient.[171] As to the lack of suitability for home treatment, whilst there can be no doubt that cryoprecipitate was less convenient than concentrates, the evidence available to the Inquiry confirms that home treatment with cryoprecipitate could and did occur.
Cryoprecipitate was not used for the treatment of Haemophilia B. Prior to the availability of Factor 9 concentrates, treatment for Haemophilia B was with fresh frozen plasma (FFP).[172]
The 1970s saw a gradual shift from the use of cryoprecipitate, largely in hospitals,[174] to the use of factor concentrates, particularly at home.[175] Improvements were steadily made in producing freeze-dried AHF, so that it became far more user-friendly than its early precursor in 1957.
Until 1973, when the first commercially manufactured concentrates were licensed for importation,[176] factor concentrate was produced at three sites in the UK. The principal English site was run by the Lister Institute (a privately funded research and production enterprise) at premises in Elstree. It operated as the Blood Products Laboratory (“BPL”) until 1978, though funded for the production of factor concentrates there by the Department of Health and Social Security (“DHSS”). Thereafter Lister was no longer able to continue its operations because of a lack of resources, and the operation continued as the BPL in that name.[177] A secondary site in England was that at Oxford, which was known as the Plasma Fractionation Laboratory (“PFL”), and the second major site was the Protein Fractionation Centre at Liberton in Edinburgh (“PFC”). At the start of the decade they tended to use small pools: a paper by Dr Rosemary Biggs in 1974[178] showed that the mean pool size in 1971 for Factor 8 was 192 donations.[179]
Competitive mass production led to commercial products being manufactured in the US and in Europe from pools which consisted of several thousand individual donations (“large pool concentrates”). The products, whether large pool concentrates from the US, or products manufactured by the three UK production facilities from smaller pools (“NHS concentrates”) revolutionised the treatment of haemophilia. The product, being concentrated and freeze-dried, could be stored in a small volume. It was relatively easy to transport. A deep freeze was not required. It was relatively easy to reconstitute the concentrate by adding sterile water: the earlier difficulties caused by “impurities”[180] (proteins other than Factors 8 and 9 contained in the final product, such as fibrinogen) had been reduced.[181] The quantity to be infused was no longer so great as to make injection difficult. A clinician could more accurately know the units of Factor 8 or 9 activity contained in a given volume in any injection, because of the averaging effect of the pools.[182] The preparation and administration of an injection was quick. It was convenient.
Though in the early 1970s injections of factor concentrates (Factors 8 and 9) were largely administered in response to a bleed, and in hospital, these characteristics meant that the phial of concentrate could easily be kept in a domestic fridge. Home treatment became easier. Initially, that too would have been responsive to a bleed.[183] But since the underlying constitutional problem was a relative lack of clotting factor in the patient’s bloodstream, it eventually began to be given to some patients in advance of any bleed, designed to stave one off by maintaining the level of clotting factor in the bloodstream sufficiently to cope with most bleeds.
Prophylactic treatment as a policy was not well developed until later in the 1980s or early 1990s,[184] but an element of prophylaxis occurred in some of the uses to which home treatment was put. Thus if a patient on home therapy knew that they were about to engage in an activity which had an elevated risk of causing a bleed, they might well choose to take some concentrate in advance. It seemed to some clinicians that patients chose to overprescribe to some extent, just to be sure they would achieve the desired effect. It soon became clear that home therapy, and occasional prophylaxis, together with the success of the factor replacement therapy adopted since 1967[185] in extending the lifespan of people with severe haemophilia (who needed the greatest number of units of product),[186] greatly increased the overall consumption of factor concentrates. The graph in Figure 1 shows that until 1973 almost all of the requirements for factor concentrate were met by NHS manufactured product. After that, the demand for factor concentrate was increasingly met by imported commercial concentrate: from 1977 until 1983 more than half of the Factor 8 concentrate supplied in the UK was commercially produced. The use of cryoprecipitate diminished until 1978, after which it comprised only a small portion of the total consumption of products supplying Factor 8.[187] Factor 9, though, was mostly domestically produced:[188] for that reason, there is no corresponding graph for Factor 9.
.svg)
Cryoprecipitate nonetheless remained in constant use for treating von Willebrand disorder.[190] And it had the considerable advantage that it required little by way of equipment to manufacture it – a centrifuge was perhaps the critical technology – compared with the much more sophisticated processes used for making freeze-dried concentrate. An implication of these two facts (that expertise in making it was retained, and the equipment needed was relatively simple and commonplace) is that it would need little additional resource to scale up production of cryoprecipitate if it proved desirable to do so.
Consumption of factor replacement therapy[191] before 1971 is difficult to measure – after that there was an internationally agreed standard of Factor 8 activity by which quantities could reliably be assessed. From about 1973 (when the first commercial Factor 8 concentrate was imported for general use, rather than for use by specific patients on particular request[192]) there was a steady increase in the UK from under 20 million international units to just under 80 million international units. This was a fourfold increase. It was fuelled by a combination of (a) the availability of a product which in its concentrated form had become more available, more readily, and both easier to use and easier to store (in a domestic fridge); leading first to its use as a home treatment (which resulted in a greater quantity of concentrates being used than would be in hospital) and then to a sporadically increasing prophylactic use (which as it developed, led to some[193] people with severe haemophilia infusing Factor 8 at home three or more times per week to maintain their baseline levels[194]); and (b) an increasing number of people with haemophilia requiring treatment, since a consequence of the success of treatment both with cryoprecipitate and factor concentrate was an increase in life expectancy. Factor concentrate formed an increasing proportion of coagulation therapy, with cryoprecipitate supplying the balance.[195] By 1982, almost all the consumption of Factor 8 was supplied by factor concentrates, as the graph shows.
A common side effect of treatment for Haemophilia A was the development of Factor 8 inhibitors. These are antibodies produced by the immune system and can occur in people with (usually severe) Haemophilia A: the reason why some people develop inhibitors and some do not “is complicated and only partially understood”.[196]Treatment options in the 1970s included Factor 9 concentrate, FEIBA[197] and Autoplex.[198] People with Haemophilia B and Type 3 von Willebrand disorder could also develop inhibitors though less frequently.[199]
In the late 1970s a synthetic product – desmopressin (known as DDAVP) – became available as a treatment for Haemophilia A (in particular, but not solely, people with mild Haemophilia A) and for von Willebrand disorder. In 1977 it was reported, following a trial, that DDAVP infusion caused a marked increase in Factor-8-related properties in patients with moderate and mild haemophilia and von Willebrand disorder. The administration of DDAVP before dental surgery and in the early postoperative period was followed by a two- to threefold rise in Factor 8 coagulant activity. It led Professor Pier Manucci to write in The Lancet that DDAVP could be “a promising pharmacological alternative to plasma concentrates in the management of some patients with haemophilia and vWd.”[200] Von Willebrand disorder would otherwise be treated with cryoprecipitate or with Factor 8 concentrates.[201]
There is little doubt that concentrates were seen at first as a wonder drug which might revolutionise the lives of people with haemophilia. They might not need to take as much time out of school. They could play sports. Concentrates could ensure substantially less time off work.[202] They would not have to wait for their treatment to be thawed and prepared for use. People with severe haemophilia attended the clinics so frequently the doctors became well known to them, and they became well known to the doctors. It was to be expected that doctors saw and welcomed the significant improvements factor concentrates brought to the patients for whom they were caring. Sadly, this almost certainly fuelled a desire to reject any suggestion that the product might actually be doing more harm than good to those who received it, and an inclination to reject any critical appraisal of the value of administering factor concentrates as they then were.[203]
The principal developments in the 1980s involved two matters: first, the birth and development of effective techniques of viral inactivation in factor concentrates (for which, see the chapter on Viral Inactivation), which when established (after 1984 for HIV in NHS concentrate produced at PFC, 1985 for both hepatitis and HIV in NHS concentrate produced at BPL though in insufficient quantities for all English and Welsh patients, and mid 1987 for hepatitis in NHS concentrate produced at PFC, and at some later stage for commercial concentrates) ensured that cryoprecipitate was much less used in haemophilia therapy except for von Willebrand disorder, and second the development of “higher purity” concentrates. “Purity” referred not to freedom from external contaminants or microbes, but to the relative absence of proteins other than Factor 8 or Factor 9. These would be proteins such as fibrinogen or fibronectin, which were present in very much greater quantities in plasma than were clotting factors, which were trace proteins only. Throughout most of the period with which the Inquiry is centrally concerned factor concentrates were described as of “intermediate purity”; towards and moving into the 1990s “higher purity” products became more prevalent. The advantage of higher purity was that patients would receive a lesser amount of unnecessary protein from a human source foreign to the recipient than would be the case if being given intermediate purity products. This meant that they were theoretically less likely to suffer an adverse reaction to the factor product.
This chapter assesses the state of knowledge up to 1970 of the risk of hepatitis and its transmission through blood.
1923 report in Sweden suggests jaundice as an adverse effect of vaccination with a viral cause.
1942 recognition that human serum in yellow fever vaccine transmits hepatitis.
1942 Ministry of Health acknowledges connection between transfusion and jaundice and concludes that this association “may have been overlooked”.
1942 Emergency Blood Transfusion Service recognises that blood transfusion may result in delayed jaundice.
1944 MRC Jaundice Committee is told that hepatitis caused by serum transfusion after long intervals is “beyond doubt”.
1952 WHO Expert Committee on Hepatitis recognises serum hepatitis as a serious problem and suggests five preventative measures.
1954 The Lancet reports that larger pools cause higher incidence of hepatitis.
1964 Scottish Home and Health Department circular states that “All blood for transfusion must be regarded as potentially contaminated … No transfusion should be undertaken unless the benefits outweigh the risk of hepatitis.”
1965onwards blood donations in Germany are tested for raised ALT.
1970 onwards blood donations in Italy are tested for raised ALT.
ALT alanine transaminase
MRC Medical Research Council
WHO World Health Organization
Just as a first principle of medical practice is often summarised as “First, do no harm”, [204] a primary duty of government is to protect the safety of its citizens. That involves keeping them free of unreasonable risks to their health and safety wherever possible.
Blood transfusions are intended to benefit the recipient. But they are not like most medications, which are derived from chemicals. They are of human origin, and as a result vary just as humans do. So, just as the recipient may be given blood or a blood product which restores their circulation or provides them with a protein they are lacking, so too will they receive whatever may be harmful in the blood of the donor. This may be such as a virus, a parasite (such as in malaria), a microorganism (as the spirochete in syphilis), a prion (as in variant Creutzfeldt-Jakob disease), or a protein which may cause a dangerous reaction. The risk that the benefit may be outweighed by the harm of a transfusion is ever present.
Any decision to administer a transfusion thus involves risks to the patient, which go well beyond the risks of infection from breaking the skin to insert a transfusion needle. There is no general principle that all risk must be avoided: some risks simply cannot be. It may be desirable to run inevitable risks because of the importance of the object which is to be achieved by doing so. A balance has to be struck between, on the one hand, the magnitude of the risk – itself a combination of the likelihood of the risk materialising and its probable severity if it does – and, on the other hand, the importance of the purpose to be achieved by incurring it, and the availability and expense of protective measures against it. Thus the risk of catching the common cold is almost certainly increased by working closely together in offices and travelling on public transport to get to those offices. It is however a risk of low magnitude, since the probability is that any cold will be short-lived and have no serious long-term consequences. Compared with that, the magnitude of even a small chance of incurring a terminal cancer is clearly very much greater, especially if suitable protective measures cannot be taken and if it is likely that any attempted cure will be ineffective. Avoiding the risk may then be appropriate.[205]
To assess where the balance lies between risk and benefit when transfusing blood or a blood product to an individual, one must first know that there is a risk, second how serious a risk that is, third what steps can be taken to avoid or minimise that risk, and fourth whether it is unreasonable, or unreasonably difficult, to take those steps. The question is not whether taking the steps is reasonable – the fact that a step could be, but is not, taken to prevent or minimise the risk of harm means it should be taken unless it would be unreasonable not to do so. That is a more demanding standard than simply doing what is reasonable in the circumstances.
The risks may not simply be to the individual patient. Patients have families. They live in communities. A risk of infection to a patient may also be a risk to the health and wellbeing of others. Though it is for the clinician to identify the clinical need for treatment of some kind, what the available treatments are, and to advise the patient about their risks and benefits, and those of any reasonable alternative, it is a fundamental ethical principle that the ultimate decision whether to take or reject that treatment is for the patient to make.[206] Where risk may also be caused to others in the patient’s family or community, the patient will almost always be best placed to know how significant that risk is to them.
The answers to the first two of these questions (“is there a risk, and how serious is it?”) slowly began to become clear a hundred years ago in relation to suffering hepatitis as a consequence of transfusion.
In 1885 it was reported that 191 of 1,289 shipyard workers in Bremen who had been vaccinated against smallpox by a particular form of lymph[207] developed jaundice; two other groups of workers vaccinated by a different lymph did not. It seemed that some infectious agent in the lymph had caused this.[208]
From at least as early as 1923 it had not only been reported that jaundice[209] might be caused by and after vaccination, but also that a virus was the probable cause.[210] Human serum was used to carry an inoculation into the bloodstream of the recipient: it appeared to be infective.
Well before the inception of the NHS in 1948, scientists, state authorities and medical practitioners in the field knew that after any transfusion of blood or plasma (of which human serum is part) there was a risk that hepatitis would develop. Knowledge of this “post-transfusion hepatitis” became well established during the Second World War at the latest, in particular after an epidemic of hepatitis amongst US and Allied troops inoculated against yellow fever. In April 1942 the US Surgeon General, upon determining that human serum could transmit hepatitis from donors to recipients of the vaccine, ordered the omission of human serum from yellow fever vaccine production. The epidemic stopped.[211] Later the same year, in June, the UK Ministry of Health reported an outbreak of jaundice amongst children given measles convalescent serum from a particular batch (K60).[212] There was “no conclusive proof”[213] that the serum transmitted hepatitis, but enough concern that it might have done so as to justify investigation, and recall of the implicated batch. These events were reviewed by a senior medical officer in the Ministry of Health, who summarised the K60 incident, and noted that jaundice had more recently followed receipt of mumps convalescent serum, yellow fever vaccine, and whole blood or plasma transfusion. He noted an “almost complete absence of reported cases” after transfusion of blood or plasma and concluded that the association between transfusion and jaundice “may have been overlooked”.[214]
Confirmation of the association followed swiftly. By 1 December 1942, the Emergency Blood Transfusion Service discussed the fact that blood transfusion might result in delayed jaundice, caused by human serum.[215] On 2 December, a review of previous reports of post-transfusion hepatitis began with the words: “It must now be recognised that under certain circumstances at present undefined hepatic necrosis may follow the parenteral administration[216] of human blood products.”[217]
“Serum hepatitis” as it was called,[218] was well recognised by 1944.[219] That label distinguished it from “infectious hepatitis” which was caused by environmental conditions and spread principally through the oral-faecal route.
It was known at least by the time that the NHS began in 1948, that:
Jaundice was the label by which hepatitis was then more commonly known, because of the yellowing of the skin which was a frequent and obvious diagnostic sign of it.
Thus, by 1951, large pool plasma filtration was abandoned in favour of small pools because the prevalence of homologous serum jaundice was 10% in the former compared with 1% in the latter.[223] The Lancet reported in 1954 that “large pool” plasma (by which it meant a pool derived from 300 or more donations of blood) caused the highest incidence of hepatitis, but that those receiving small pool plasma had only a slight risk, similar to that carried by single donations of blood, and that it had already been decided to reduce the size of plasma pools to small pools to “restrict the dissemination of the infective agent.”[224]
Although serum hepatitis was known to be caused by viral infection, the viruses which were causative were not identified for many years. The precise microbiological configuration of the viruses did not however need to be known in order to understand that post-transfusion hepatitis could have serious consequences. This became very well understood, whether the transfusion was of whole blood or plasma. As early as 1946, Dr William d’A Maycock recorded an agreement that users of plasma “must be told that it is a potentially lethal fluid which should be used with discretion.”[225]
In 1966, the British Medical Journal had reported that when relatively large plasma pools were used the incidence of serum hepatitis could reach the alarming figure of 11.9%, though if the pool was of ten bottles or fewer the figure fell to 1.3%.[226]
By 1970 it was authoritatively reported that serum hepatitis caused death at a rate of approximately 1 in every 150 transfusions in the US in people over the age of 40. An infection rate of 3.6% of all transfused hospital patients was reported. US studies showed that the mortality rate in late middle age of those infected could be as high as 40%, and in patients over 60 about 50%.[227]
Deaths were known to be the consequence of liver failure, caused by chronic infection leading first to fibrosis, chronic active hepatitis, then to cirrhosis of the liver, and then in a significant number of cases to liver cancer. Though in many cases of serum hepatitis the effects might appear short-lived (a noticeable but quickly fading jaundice) or barely apparent at all, it was known that in many cases chronic infection would follow. Liver failure and liver cancer were then almost inevitably fatal. The risks of these consequences of chronic hepatitis were sufficiently appreciated not only by scientists but by the Government, such that the Scottish Home and Health Department said in a circular in December 1964 that: “All blood for transfusion must be regarded as potentially contaminated … The most important transmissible disease in this country is homologous[228] serum jaundice or serum hepatitis … No transfusion should be undertaken unless the benefits outweigh the risk of hepatitis.”[229]
Because the viruses had not been identified, it was impossible (a) to develop a test to show if they were present in any donation of blood or plasma; or (b) to treat infection effectively, since it could not be shown except by passage of a considerable time that the virus had been inactivated in the person infected. The lack of any known serological marker[230] was often echoed by an absence of any specific symptom – many of the consequences of infection, such as tiredness, itchy skin, depression, a muzzy head or “brain fog”, could so easily be ascribed to the general activities of life, to ageing, to the demands of childcare or to hormonal changes. This, coupled with the challenges of relating current infection to an event possibly ten or twenty years earlier that might have caused it, undoubtedly meant that it often went unrecognised by the person who was infected, was under-reported, and was often diagnosed on clinical grounds far too late.
However, the risks of post-transfusion hepatitis were appreciated not only in the US and the UK, but also internationally. In 1952, an Expert Committee on Hepatitis of the World Health Organization (“WHO”) reported serum hepatitis as a serious problem, which in many cases came on insidiously and in some cases persisted beyond five years.[231] It suggested five measures to reduce the risks of the disease: (1) the selection of donors; (2) the control of pool size; (3) the treatment of plasma; (4) the maintenance of records; and (5) reporting.[232] If these measures had been taken appropriately during the next 30 years, in relation to the supply of blood and blood products in the UK, it is reasonable to think that a significant part of the suffering on which this Inquiry is focussed would not have occurred.
Elsewhere precautions were taken to lessen the chance that those risks might materialise. Thus in Germany, from 1965 onwards, all blood donated for possible transfusion was tested to see if it contained abnormally high levels of a liver enzyme, alanine transaminase (“ALT”). Raised ALT levels are not specific for hepatitis – they may be caused by a number of other circumstances too, for instance the consumption of alcohol, or obesity – but they can indicate liver dysfunction.[233] In this country, some comfort was taken from the fact that donors had no motive in giving blood other than to benefit another human being: they donated as a gift. By contrast, in the US, many, if not most, of those who gave blood and plasma did so to benefit themselves directly or indirectly, and inevitably had far less interest in the quality of what they were providing. The incentive was instead for them to be dishonest about their state of health.[234] The first of the five measures recommended by the Expert Committee on Hepatitis of the WHO in 1952 was thus addressed (at least in part) by reliance on the voluntary nature of blood donation in the UK.[235] It might also be addressed by asking some questions of a would-be blood donor, to help assess whether taking and using their donation might be more risky than usual.
“Infectious hepatitis”, which became known as Hepatitis A, was not identifiable as such until 1973.[236] However, in 1965, researchers identified an antigen which was associated with serum hepatitis.[237] This led to a virus being isolated in 1967, termed Hepatitis B,[238] though it took until 1970 when the “Dane particle” was discovered for the complete virus to be demonstrated by electron microscopy. By around 1970, there was finally a test to screen blood for the presence of Hepatitis B, though it was not sensitive enough to identify every case of infection in the blood.[239]
The Department of Health and Social Security (“DHSS”) appointed an advisory group which advised in July 1971 that the regional transfusion centres should begin testing “at the earliest possible date” and the DHSS accepted the recommendation.[240] The regional transfusion directors met that month and noted that the transfusion centres at Sheffield and Edgware were testing all donations, some centres were testing some donations and some would not be able to start until late in 1972.[241] From November 1971 the Blood Products Laboratory tested the plasma used to make blood products and from December 1972 all blood donations in England and Wales were screened, then mostly by immunoelectrophoresis.[242] The Scottish National Blood Transfusion Association annual report for the year ending 31 March 1972 recorded that routine screening had been in place in Scotland for at least a year in all centres and longer in some.[243] By 1975, two years after Hepatitis A was identified, there was a test for both Hepatitis A and Hepatitis B.[244]
Despite the increasing ability in developed economies to be able to screen out Hepatitis B from the blood supply, Italy also introduced ALT testing of donations with effect from 1970. This increased the protection against infections which might cause hepatitis but which Hepatitis B testing, particularly in its early forms, failed to spot.[245] The UK never adopted ALT screening.[246]
Four themes are explored in this chapter: a developing awareness of non-A non-B Hepatitis transmission through blood and blood products and of the potential seriousness, the repercussions of introducing a screening test for Hepatitis B, the risks associated with paid donations, and the risks of pooled donations.
February 1970 The Gift Relationship discusses the increased risks of hepatitis with paid donations.
1972 Professor Garrott Allen emphasises the increased risk of serum hepatitis “from transfusions derived from prison and Skid Row populations”.
November 1972 publication by Dr Alter and others recognises that Hepatitis B does not account for all post-transfusion hepatitis.
August 1974 Dr Prince and others report in The Lancet that an agent other than Hepatitis B is the cause of 71% of cases of post-transfusion hepatitis and may be implicated in chronic liver disease.
January 1975 Professor Garrott Allen attempts to persuade Dr Maycock of the dangers of importation of factor concentrates.
January 1975 Dr Owen pledges to fund self-sufficiency in blood products.
May 1975 WHO urges self-sufficiency and supports voluntary non-remunerated blood donation.
August 1975 The Lancet reports on a hepatitis outbreak at Bournemouth haemophilia centre following treatment with Hemofil.
December 1975 broadcast of Blood Money highlights hepatitis risks of commercial concentrates.
February 1976 article by Dr Alter and others suggests the long-term prognosis of NANBH may be similar to Hepatitis B.
July 1976 article by Dr Hoofnagle and others suggests that until the nature of NANBH is “elucidated”, blood and blood products should be considered as potentially infectious.
1977 articles by Dr Alter, Dr Hoofnagle and others emphasise that NANBH can progress to chronic hepatitis and cause liver disease.
September 1978 publication in The Lancet of study by Dr Preston and others showing chronic liver disease in patients with haemophilia treated with factor concentrates.
April 1979 Dr Kernoff describes NANBH as “a serious disease with long-term consequences”.
September 1980 international symposium in Glasgow considers risks of NANBH.
September 1980 memo from Dr Walford describes NANBH as a form of hepatitis that “can be rapidly fatal ” or “can lead to progressive liver damage”.
July 1981 The British Medical Journal reports hepatitis as “the major complication of the modern treatment of haemophilia.”
ALT alanine transaminase
NANBH non-A non-B Hepatitis (Hepatitis C)
Four themes predominate during the 1970s: a developing awareness that viruses other than Hepatitis A and Hepatitis B – in other words, non-A non-B Hepatitis (“NANBH”) (which would later come to be known as Hepatitis C) – were being transmitted through blood and blood products; the repercussions of introducing a screening test for Hepatitis B; the knowledge of the risks associated with the paid donation of blood for imported factor products; and the risks that pooled donations presented.
In February 1970, Professor Richard Titmuss published a book which was recognised in The New York Times as one of the seven most important non-fiction books to be read that year. [247] In his evidence to the Inquiry, Lord David Owen said he thought every doctor would have been aware of it.[248] The Gift Relationship compared the system of voluntary non-remunerated blood donation in those countries such as the UK, which saw the giving of blood for the treatment of others in need as an important social obligation, with systems such as those in the US, which relied substantially upon “donors” being paid to give their blood. One saw donating blood as giving the gift of life; the other saw it as buying and selling a commodity. There was a market in blood, and in particular in plasma. Pharmaceutical companies in the US and elsewhere[249] used plasma in particular to produce products which could be marketed worldwide. Unless precautions could be taken, a virus prevalent in the blood and plasma of even one member of the donor cohort could find its way into a blood product, and hence to a recipient in a country where the virus was less prevalent, if present at all. Where no test is available to identify and exclude a virus, any single donation might carry that virus. It is more likely to do so where the donation is sold for private benefit, rather than given altruistically. Moreover, there is a commercial incentive to buy necessary raw materials as cheaply as practicable. The raw material for blood products was human in origin. In stark contrast to sourcing blood from unpaid donors, who will come from any part of society, rich or poor alike, US pharmaceutical companies bought plasma from cheap sources, including “down-and-outs” in particular in New York and San Francisco, prisoners, and those living in poorer countries such as Mexico, Belize and Lesotho.[250]
President Richard Nixon directed his officials to recommend an improved blood collection and distribution system to reduce reliance on commercial blood banks, which were described as often accepting “blood from such donors as derelicts and drug addicts who may be the transmitters of such diseases as hepatitis, syphilis and malaria. A study made two years ago indicated that 30,000 Americans contract hepatitis each year through transfusions of contaminated blood with 1,500 of them dying from the effects of the disease.”[251]
In his book, Professor Titmuss drew attention to a series of studies demonstrating the risk of hepatitis incurred by those who received transfusions of whole blood or blood products, to support his case that a system relying on voluntary non-remunerated donations was very much safer not only in theory but in reality.[252] Very shortly after he published his book, Professor Joseph Garrott Allen of Stanford University confirmed exactly that same message: the hepatitis risk posed by blood commercially sourced was markedly higher than the risk from blood and plasma sourced from truly voluntary donors.[253] Nor was this a new warning: he had drawn attention to it as long before as September 1959,[254] and had returned to the theme in several following publications.[255] Professor Garrott Allen emphasised also the seriousness of transfusion hepatitis: “The numbers of patients with transfusion hepatitis … who will be able to show disability or who will die of this disease, will be approximately 0.9% of the total transfused.”[256]
When Professor Titmuss wrote, he did not distinguish between the different viruses which together caused serum hepatitis. It is reasonable to think that until the early 1970s scientists, doctors, politicians, administrators, and manufacturers of blood products assumed that the inflammation of the liver which gave the disease its name was caused by just one virus.[257] It may be that they thought that with the discovery of the Australia antigen in 1965 and identification of the Hepatitis B virus by 1967 that the virus had been found. In 1970 it was shown to be possible to screen blood donations for the presence of Hepatitis B. The Report of the Advisory Group on Testing for the Presence of Australia (Hepatitis-Associated) Antigen and its Antibody noted that: “Knowledge of all aspects of Australia (hepatitis-associated) antigen is accumulating very rapidly” and that “Although the hepatitis agent may be less widely dispersed in the UK than in some other countries, the institution of testing donations for Australia antigen should reduce the incidence of serum hepatitis, which is the most serious complication of transfusion and so avoid suffering and disablement and even death.”[258]
By October 1971, the Blood Products Laboratory was screening plasma for Hepatitis B.[259] Though the tests were imprecise,[260] it was not unreasonable to think that the cause of post-transfusion hepatitis had been identified and the risk of infection had been reduced in consequence. It was hoped that once the tests were improved the blood supply (and products made from tested plasma) would be relatively free of any significant risk of post-transfusion hepatitis. This was not to be. Any such optimism soon began to evaporate, starting from 1972,[261] and growing throughout the mid 1970s, when it was increasingly reported that hepatitis was occurring after transfusion, yet when tested the patient was suffering neither from Hepatitis A nor Hepatitis B.[262]
Of particular note was the report by Dr Alfred Prince and others in The Lancet in August 1974 that an agent other than Hepatitis B was the cause of 71% of cases of post-transfusion hepatitis: “The data suggest that a large proportion of long-incubation post-transfusion hepatitis is unrelated to hepatitis B and that control of post-transfusion hepatitis will require identification of a hepatitis virus(es) type C.” As to the potential significance of this virus:
“The fact that non-B hepatitis cases are less frequently associated with serious acute illness does not imply that such cases are of lesser importance. Long-term complications of acute hepatitis-B infection, such as chronic hepatitis, cirrhosis, and hepatoma, have been reported to follow mild anicteric infections more frequently than severe icteric cases; consideration must thus also be given to the possibility that non-B hepatitis may play a role in the aetiology of some forms of chronic liver disease.”[263]
This publication was one of the most widely-read journals by clinicians in the UK: no clinician dealing with transfusions had any reason to be unaware of this conclusion.
Though outbreaks of Hepatitis B continued in the 1970s,[264] the majority of infections post transfusion were of this third type. Not knowing whether it was one virus (which might have justified the label “Hepatitis C”) or more than one, science opted for the label “non-A non-B Hepatitis”. Though cases of serum hepatitis which were undoubtedly Hepatitis B continued, since the tests used to screen donations were imprecise and viruses “slipped through the net”, they formed a smaller part of serum hepatitis. But serum hepatitis continued, now principally in the form of NANBH.[265]
On 6 January 1975, Professor Garrott Allen wrote to Dr William d’A Maycock (the consultant advisor to the CMO[266] in respect of the Blood Transfusion Service) to attempt to persuade him to advise against the continued importation of some factor concentrates from the US to the UK. He said that one commercial product which “as you know” was sourced “100 percent from Skid-row derelicts” was extraordinarily hazardous – a 50-90% rate of hepatitis developed from its use. He added that “The other imponderable which has troubled most of us is the ineffectiveness in screening for the HB antigen … This failure, of course, dates back to at least 1971, and suggests that half, if not more, of the cases of posttransfusion hepatitis are caused by an agent other than Hepatitis A or B.”[267]
Two other significant warnings were given in the course of 1975: in May the World Health Organization urged the development of national blood services based on advised self-sufficiency for all nations, and supported voluntary non-remunerated blood donations (ie self sufficiency for all nations),[268] and in December Granada’s World in Action highlighted on TV in two documentaries called Blood Money that there was a high risk of hepatitis in blood sourced commercially from prisons and “skid row” paid donors, and used to make coagulation products.[269] It was obvious that there was a continuing risk of serious hepatitis from the use of commercial products which on two bases were more dangerous than domestic products: (a) the source material came from donor populations where the underlying rate of hepatitis infection was between five to twenty times greater than that in the UK; and (b) the risk was amplified by the much larger pool sizes used in commercial manufacture.
A way of avoiding the need to rely upon the purchase of commercial products, and the risks they brought with them was to achieve self-sufficiency (producing enough of the necessary product domestically to avoid any need for importation). Since Self-Sufficiency has a chapter of its own, only a short sketch needs to be made of it at this stage.
The desirability of self-sufficiency had been recognised for over seven years by this stage. One of the most authoritative medical voices of the late 1960s in the field of haemophilia, Dr Rosemary Biggs, made a prediction in August 1967 that within the “next year or two” very large amounts of commercial product would become available in the US. “When this material comes on to the market we shall be obliged to buy it at a very high cost”.[270] Self-sufficiency in blood supply had always been a policy objective since the Second World War. Blood products were forming an increasingly important part of this supply by 1970. The goal of self-sufficiency remained, given impetus by Professor Titmuss’ book, national pride, and the belief, which it is clear Dr Biggs shared, that purchasing supplies from abroad would be more expensive than producing blood products domestically. This was in addition to the knowledge that if self-sufficiency were achieved the risk to any recipient of blood or a blood product would be derived from the domestic population, and not from a country where there might be different viruses, or different diseases, transmissible through blood.
Dr Owen was himself convinced of the need for self-sufficiency. He made a pledge to Parliament on a number of occasions in 1975 that the Government would fund self-sufficiency in blood and blood products.[271] He intended that it should be achieved by mid 1977 if not earlier, such that the importation of the riskier commercial products into the UK need continue no longer. However, self-sufficiency did not occur for well over a decade.[272] In that period,[273] risks from blood products eventuated which had in the main been imported. Suffering and deaths resulted in the population of the UK, as could have been (and was) both foreseeable and foreseen.
Hepatitis B often revealed itself clinically by a yellowing of the skin: it was “icteric”. NANBH was less likely to be icteric. Liver function tests showed consistently elevated enzyme levels (in particular of alanine transaminase (“ALT”)) in Hepatitis B infection, but generally levels which fluctuated and were less elevated in NANBH. Hepatitis B was often symptomatic in its acute phase (“acute” means occurring within six months of infection: it does not refer to the severity of the symptoms caused by the infection), whereas NANBH was more rarely so – though more likely to result in a persistent chronic infection (“chronic”[274] means lasting for more than the first six months of infection).
For some time a number of doctors held the view that NANBH was a mild or benign disease. The view that the disease was mild rested centrally on assertion and/or wishful thinking[275] rather than evidence, and was reached by a comparison with Hepatitis B in the acute phase rather than on epidemiological studies. Such evidence as there was for it amounted to noticing that the skin often did not yellow, as it usually did with Hepatitis B; that the extent to which liver function tests showed high levels of ALT or aspartate aminotransferase (“AST”)[276] was usually less than in the case of Hepatitis B, and that the symptoms arising in the first six months after a transfusion thought to be causative were usually less significant. This represented a serious and collective failure of judgement amongst the many who asserted it. At its heart was making an unjustified assumption, and asking the wrong questions.
The unjustified assumption was that most or all of the serious effects of what had previously been known as serum hepatitis were attributable to the recently identified Hepatitis B.
In the 30 years since the ending of the Second World War post-transfusion hepatitis was noted sometimes to have a short-lived, acute, flu-like phase, and then remain apparently asymptomatic for several years. Though the damage it caused, and its presence, were potentially detectable by liver biopsy, there might be little obvious reason to conduct such a test. Indeed, to do so in a person with a bleeding disorder might be risky, for some bleeding would be bound to occur and steps to control this might not work well.[277] Eventually, however, it was known that in many cases increasing liver dysfunction might appear, leading to cirrhosis and sometimes to cancer. That is why “serum hepatitis” was regarded as a serious disease. It was sufficiently so that it was thought that the costs in time and resources involved in screening all blood donations for the presence of Hepatitis B were justified, even though the tests initially used were able to identify only around one third of the infections.
By the mid 1970s, it was understood that serum hepatitis had at least two contributory viral causes. Unless there was good evidence to show that Hepatitis B on its own had caused almost all the serious effects previously attributed globally to “serum hepatitis”,[278] NANBH viruses simply could not be assumed to be any less harmful. The observed effects of serum hepatitis might just as well have been caused by the major[279] viral component[280] of serum hepatitis (NANBH) as by what now seemed the lesser (Hepatitis B). There could have been no proper confidence that NANBH would not have serious long-term consequences which would emerge only after an extended period of chronicity. After all, hepatitis by definition involves some damage to the liver. Damage to the liver is potentially serious.
It is not the judgement of enlightened hindsight, but a realistic appraisal to say that clinicians and researchers should have been alert at that time to what was at least a risk of chronicity, and receptive to reports that the long-term consequence of hepatitis was serious, earlier than was the case.[281] Some were. But by no means all.
The question that should have been asked, particularly given what was now at least a 25-year history of familiarity with serum hepatitis, was whether NANBH might have long-term consequences: put another way, whether the risk that it might do so could be excluded. Dr Pier Mannucci, a highly respected haematologist, noted in 1975, after considering liver disease in people with haemophilia which had produced no overt symptoms, the possibility “that repeated and prolonged contact with the infective agent(s) may cause chronic liver damage not associated with overt illness”.[282] Just a few months later Dr Robert Purcell, Dr Harvey Alter (later to be awarded the Nobel Prize for his work in this area) and Dr Jules Dienstag commented further that “Although type non-A, non-B hepatitis is associated with less severe acute illness than type B disease, as judged by frequency of jaundice and magnitude of SGPT [serum glutamic-pyruvic transaminase] elevations, the long-term prognosis for the two diseases may be similar”and “chronic non-A, non-B hepatitis is not necessarily a benign infection and may be the cause of a significant proportion of chronic hepatitis not identifiable as type B disease”;[283] and in their turn Dr Jay Hoofnagle and others, just a short while later again, added: “Until the nature of this [NANBH] virus and its disease is elucidated, it is important to consider human blood and pooled plasma products as potentially infectious. At the present time, fibrinogen, AHF [antihemophilic factor] and Factor IX concentrates remain ‘high-risk’ plasma products”.[284]
The alert might have been sounded yet more clearly by the report of an outbreak of hepatitis at the haemophilia centre in Bournemouth after the administration of Hemofil, a commercial factor concentrate, which was the subject of a report in The Lancet in August 1975.[285] Subsequently, Dr John Craske (of the Public Health Laboratory Service) and Dr Peter Kirk (at Lord Mayor Treloar’s College, Hampshire) produced a retrospective survey of Hemofil-associated hepatitis. They concluded that the incidence of chronic consequences due to NANBH “is at present unknown”, and that “Further follow up will be required to assess the incidence of chronic liver disease after non-B hepatitis”.[286]
By 1978 there were a number of reports showing that NANBH was linked to persistent liver damage.[287] Dr Hoofnagle and others wrote in 1977 that:
“Several clinical and epidemiological features of non-A, non-B hepatitis have become clear from studies such as the present one. First, non-A, non-B hepatitis closely resembles type B hepatitis. The incubation period, the clinical symptoms and signs, and the potential for chronicity appear to be similar to type B hepatitis … Undoubtedly, what was once referred to as ‘serum hepatitis’ included both type B and non-A, non-B hepatitis. Second, [most cases of] non-A, non-B hepatitis … have been described in association with transfusion, intravenous drug use, or serum inoculation … Third, non-A, non-B hepatitis appears to be associated with a chronic carrier state and chronic liver disease … Finally, non-A, non-B hepatitis appears to be common. Three of the five infectious donors studied here transmitted this non-A, non-B hepatitis.”[288]
To like effect, Dr Alter, also in 1977, emphasised that “Although non-A, non-B hepatitis is, on the average, less acutely severe than type B hepatitis, it can cause severe acute disease and, more disturbing, it appears to have considerable propensity to progress to chronic hepatitis.” He urged that the major thrust of post-transfusion hepatitis research be directed at developing methods for detecting the virus or developing a method of viral inactivation.[289]
In September 1978 The Lancet published a paper by Dr Eric Preston and colleagues in Sheffield, reporting on the “systematic screening of forty-seven haemophiliacs in Sheffield” which revealed abnormal liver function tests in 77% of the patients, “with a tendency for these abnormalities to persist.” Liver biopsies on eight symptom-free patients demonstrated a “wide spectrum of chronic liver disease … including chronic aggressive hepatitis and cirrhosis”, which the authors attributed to treatment with factor concentrates. NANBH rather than Hepatitis B was thought to be an “important factor” in four of the eight patients.[290]
In his oral evidence, Dr Mark Winter said that this paper “blew out of the water instantly the idea that this [NANBH] was nothing to worry about because their study showed, as did other studies, that most of these patients had very significant chronic liver disease”. It was something haemophilia doctors could not simply ignore.[291] He ascribed doctors as having been unwilling to think that NANBH might be a problem because factor concentrate had brought “such spectacular benefits”: it was this reluctance to face the facts as portrayed in scientific journals that had therefore prevented earlier acceptance of the seriousness of the problem.[292] There had, in his view, been a “golden interval” after screening for Hepatitis B first began, during which the dangers of NANBH had not yet fully been understood, and it seemed as if Hepatitis B was going to be a diminishing threat as screening tests improved. It ended, as he saw it, in the publication by Dr Preston and others.[293]
In January 1979 Dr David Dane, of the Middlesex Hospital, after whom the “Dane particle” which had enabled successful screening tests for Hepatitis B was named, wrote to Dr Sheila Waiter at the Department of Health and Social Security (“DHSS”) about NANBH, with the observation that “If one or more of these viruses is responsible for the abnormal livers which are evidently common among haemophiliacs then chronic liver disease due to these viruses might also be found among other transfused individuals.”[294]
By February 1979 the Medical Research Council had been told by the chief scientist of the DHSS that non-A non-B Hepatitis was “being given high priority by the Department”.[295] An ad hoc meeting was convened (on 12 March 1979) at which Dr Craske noted that studies in people with haemophilia showed that NANBH might severely damage the liver. He reported that US and German workers said that up to 40% of NANBH infections progressed to chronic liver disease.[296] Professor Arie Zuckerman told the meeting that “much non-A non-B associated PTH [post-transfusion hepatitis] might be anicteric, and that the risk of progression to chronic liver disease remained, however mild the initial infection.”
Concern about the dangers of hepatitis was not consigned to the text of scientific journals. At least one commercial supplier thought them sufficiently serious to justify a price premium for a product which had less risk of transmitting hepatitis. Source plasma was thought far more likely to be infected if it came from the US than plasma sourced elsewhere: and it was reported in April 1979 to the UK Haemophilia Centre Directors’ Organisation reference centre directors that Immuno Ltd (based in Vienna) now sold their Kryobulin Factor 8 concentrate at two prices. The cheaper was that which had been manufactured from US plasma.[297]
At the end of April 1979 Dr Peter Kernoff wrote to Dr Brian Colvin, in the latter’s capacity as secretary of the North East Thames Region Association of Haematologists, observing that NHS concentrates were to be preferred to commercial concentrates because of:
“the growing awareness of the probability that commercial concentrates have a higher risk of transmitting non-A non-B hepatitis than NHS material. This is a serious disease with long-term consequences which, as far as is known, is at present much less common in the U.K. than in those parts of the world – particularly the U.S.A. – where donor blood for commercial concentrates is collected … The only medium to long-term solution to these problems is for the NHS to markedly increase production of factor VIII.”[298]
The Lancet added to the concerns being expressed about the long-term consequences of NANBH in a report in May 1979. It spoke of NANBH being related to a “high frequency of persistent hepatic dysfunction”.[299] In a report to the DHSS for 1978-79, Professor Zuckerman recorded the conclusion of research at the University of London that “until blood donors can be specifically screened for the virus(es) of non-A, non-B hepatitis, it would seem wise to restrict the use of blood concentrates to life-threatening situations.”[300]
The wisdom of this course was echoed on 16 May 1979 by the North East Thames Regional Association of Haematologists Haemophilia Working Party when it issued guidelines on the screening and investigation of hepatic disease in patients with congenital coagulation disorders. They said: “Despite the generally mild nature of acute non-A non-B hepatitis it seems very possible that there may be serious long-term sequelae and the acute disease may sometimes be fatal.”[301] This drew an important distinction between acute NANBH and chronicNANBH: there is a suspicion that those clinicians who at the time described NANBH as “generally mild” were thinking of the acute phase – there could be little doubt that the chronic phase (which would follow in all bar some 20% of infections)[302] was potentially anything but mild.
In July 1980 the findings of liver biopsies undertaken at Sheffield Children’s Hospital were published. Five boys with haemophilia whose liver function was persistently abnormal underwent biopsies: in each case the biopsy “confirmed underlying chronic liver damage, ranging from chronic persistent hepatitis to chronic aggressive hepatitis with early cirrhosis.” Only one had serological evidence of previous Hepatitis B infection.[303]
An international symposium into “Unresolved problems in Haemophilia” was held in Glasgow in September 1980. During it, Professor Peter Scheuer from the Royal Free Hospital said that the American literature suggested that when compared with hepatitis B, “the non-A, non-B tends to be more symptomless. Secondly, the incidence of serious sequelae is likely to be higher than the B.” When speaking of “symptomless” he was plainly talking of the acute phase: his “serious sequelae” shows that. Dr (later Professor) Howard Thomas and Dr (later Professor) David Triger (hepatologists) agreed, for their part, that “we are just building up trouble” and “it is in 10 years time that we shall see the problems. Bearing in mind the proportion of the patients that are infected, or have persistent abnormal liver function tests, anything from 60 to 80 per cent, it will be an enormous problem when it happens.”[304] Professor Thomas told the Inquiry that the messages from the symposium, the 1978 Sheffield study and other publications from 1981 and 1982 “were all in accord really.”[305]
Because the symposium was attended by leading lights in the treatment of haemophilia and hepatitis in the UK,[306] and followed on from the annual meeting of haemophilia centre directors, there is strong reason to suppose that haemophilia centre directors were either aware, or would rapidly be made aware, of the views of the experts at the symposium. There is no good reason after that why they should have thought that NANBH was benign.
By 1980 Dr Diana Walford at the DHSS was confident enough of the position to write a memo during the course of which she said: “I must emphasise that 90% of all post-transfusion (and blood-product infusion) hepatitis in the USA and elsewhere is caused by non-A, non-B hepatitis viruses which (unlike hepatitis B) cannot, at present, be detected by testing donor blood. This form of hepatitis can be rapidly fatal … or can lead to progressive liver damage. It can also result in a chronic carrier state, thus increasing the ‘pool’ of these viruses in the community.”[307]Notwithstanding the contents of the memo from Dr Walford, Lord Cullen, speaking in the House of Lords on behalf of the Government in February 1981, said that “There is a danger that Factor VIII, which has to be injected into haemophiliacs, can have in it a strain of hepatitis, and at the moment there is no way of testing for these strains. That is the one product as to whose freedom from infection we cannot be absolutely certain. However, every effort is made to see that it is not infected, and although occasionally something may happen, it is not of a serious nature.”[308]
Only a matter of days after Dr Walford’s memo, Dr Craske told a meeting of UK Haemophilia Centre Directors that: “Large pool concentrates appeared to give a higher risk of hepatitis than small pooled concentrates and Dr Craske felt that increased usage of small pooled concentrates would help to reduce the incidence of hepatitis in the haemophilic population.”[309]
At the very start of the 1980s, therefore, it was clear that hepatitis in consequence of a blood transfusion, or receipt of a blood product to treat haemophilia, carried with it a serious risk of long-term consequences.[310] It was known that this could not be ascribed simply to Hepatitis B infection, for that had been progressively screened out from the start of the 1970s (though it still remained as a risk and researchers were alert to the need to exclude it).[311]
It was clear that after transfusions (or blood products) liver damage or cirrhosis sometimes developed. It was clear that the cause in a number of cases was certainly not Hepatitis B. It was thus clear that there was some other cause – probably non-A non-B hepatitis. Thus when, after screening, it was apparent that hepatitis was still being transmitted and that it was not Hepatitis B, no assumption ought to have been made that it was less serious unless there was convincing proof that was the case.[312] It should have been assumed there was such a risk, rather than the opposite, unless it had become clear that the assumption was unjustified. It never was. It never could be. Those suggesting it was the case were not taking the careful, methodological approach of fitting the theory to the observed facts, but rather of wishing the world to be other than it truly was. They asked the wrong question. Instead of asking whether there was sufficient evidence that NANBH was a serious disease and/or as serious a disease as Hepatitis B they should have asked whether they could reasonably exclude the risk that it may cause the long-term consequences that serum hepatitis had been shown to cause. They might have added whether they could reasonably ignore the risks to which a number of well-regarded researchers had referred to in various prestigious publications.
The view that NANBH was relatively benign and non-progressive nonetheless remained difficult to shift in the early 1980s. Professor Charles Hay, whose personal view by 1984/5 if not earlier was that NANBH was neither benign nor non-progressive, nonetheless thought that was a generally held opinion.[313] He described it in evidence as “the consensus view”.[314] This has been frequently said, but it does not fit very closely with the contemporaneous evidence. That was to the effect that acute NANBH was less severe than acute Hepatitis B: but that in the longer term there was significant evidence accumulating that a large proportion would develop active hepatitis leading potentially to cirrhosis. It was not just the view of a handful of researchers or clinicians. Thus Armour Pharmaceutical published Plasma Perspectives in July 1981 to inform readers of the current state of knowledge, saying: “Studies of the histopathological sequelae of acute non-A, non-B infections indicate that chronic liver damage, which may be severe, may occur in as many as 40-50% of the patients whose infection is associated with blood transfusion or with treatment by haemodialysis.”[315] In that same month The British Medical Journal editorial was devoted to post-transfusion hepatitis, referring to it as remaining “the major complication of the modern treatment of haemophilia.” Some reference was made in evidence to a paper by Dr Richard Stevens and others, headed Liver disease in haemophiliacs: an overstated problem? What the article did not suggest was that NANBH was a mild disease, since it concluded that the results found were similar to reports in larger studies where 16% (ie roughly one in every six people) had suffered chronic active hepatitis and cirrhosis.[316] The very fact that the article was termed “an overstated problem?” (when recording results consistent with between one sixth and one fifth of infected persons going on to develop active liver disease) suggests that the authors understood the general view at the time to be that, indeed, it was to be taken seriously.
There were some reasons for wondering if NANBH did cause serious deterioration – in 1981 Stirling et al in Liver function in Edinburgh haemophiliacs: a five-year follow-up compared results before introduction of NHS concentrates in 1974 with those in 1979. Liver function in those treated with Factor 8 concentrate had deteriorated; those treated with cryoprecipitate had not. The article commented: “there does not [at present] appear to be sufficient evidence of any serious deterioration in liver function from NHS concentrate to limit its current use for patients on home treatment, for whom the convenience of the product is all important. It would seem reasonable, however, that patients in hospital should whenever possible receive non-pooled cryoprecipitate instead.”[317]
However an editorial in the British Medical Journal in July 1981 chillingly observed: “in some cases early death from liver disease might prove to be the price paid by haemophiliacs for the improved quality of life afforded by the easy availability of clotting-factor concentrates.” It spoke of three practices which might reduce the risks, focussing on “the risks of collecting plasma from paid as opposed to volunteer donors; the optimum size of the plasma pool; and attempts at removing the several viruses of hepatitis from blood products.” As to the first of these, the British Medical Journal said the rate of infection from paid donor blood was six to seven times that from volunteers; the rate of infection dropped by 75% in a hospital which changed from paid to volunteer blood.[318] As to the second, Dr Stirling’s report on Scottish patients showed that use of cryoprecipitate did not affect liver function by contrast with commercial concentrate.[319] As to the third, “three recent reports [suggested] that viral contamination may be removed by specific processing by chemicals, ultraviolet light, or heating.”[320]
It could have added that the “optimal use of blood and its components” would reduce the risk of NANBH.[321]
Since 1980 it has often been said, almost by way of apology or excuse for the failure of many to realise soon enough the risks posed by NANBH, that what was labelled either NANBH or Hepatitis C was a “new” or “newly discovered” virus, as if it had emerged for the first time in the mid 1970s, or later when the label Hepatitis C was first adopted. That is simply wrong. It was in truth almost as old as the hills.[322] Its genetic code was first established in 1988, and a test for its presence developed in 1989, and it was first labelled Hepatitis C shortly afterwards: so it became recognisable, and could be screened for, only then. It was thus “new” only in the sense of being newly coded and freshly labelled, but it was not new in the same sense that HIV, or more recently COVID-19, have been. Its consequences, wrapped up with those of Hepatitis B to similar effect and known as serum hepatitis, had been known of for a long time, before either Hepatitis B or C was identifiable (or labelled) as such.
This chapter examines the progression of the knowledge of AIDS between 1981 and 1984.
5 June 1981 CDC reports a cluster of people suffering from immune system failure, with a further 36 cases in July and 70 more in August.
December 1981 CDC reports cases in intravenous drug users.
March 1982 infectious agent as the cause of AIDS is the leading hypothesis for CDC.
June 1982 AIDS discussed at Second International Symposium on Infections in the Immunocompromised Host, Stirling.
9 July 1982 CDC director alerts all US haemophilia centres to a new disease and requests notification of all new cases.
16 July 1982 CDC reports three confirmed cases of people with haemophilia who had developed AIDS; Dr Gunson alerts DHSS.
August 1982 CDSC introduces surveillance for AIDS.
3 October 1982 US National Hemophilia Foundation urges pharmaceutical companies not to use plasma from gay men, intravenous drug users or people from Haiti.
November 1982 report from Dr Craske indicates likeliest cause of AIDS is infectious agent.
November 1982 Observer reports “major speculation” that AIDS virus is “carried in the blood”.
December 1982 MMWR reports the “San Francisco baby” case, the death of the three patients from the July 1982 MMWR and more cases of AIDS in haemophilia patients.
13 January 1983 New England Journal of Medicine: “If the use of cryoprecipitate will minimize this risk, the current home-infusion program needs to be revised”.
19 January 1983 discussion of AIDS at UKHCDO Hepatitis Working Party meeting.
24 January 1983 meeting at Heathrow between haemophilia doctors and Immuno.
29 January 1983 Lancet reports that bloodborne agent seems likely cause of AIDS.
3 February 1983 New Scientist suggests “prime suspect” is blood borne virus.
7 March 1983 letter from Dr Evatt (CDC) to Professor Bloom says epidemic is evolving with a frightening pace.
26 April 1983 Professor Bloom reports probable case of AIDS to CDSC.
1 May 1983 Articles in Observer and Mail on Sunday describe risk of AIDS.
4 May 1983 Professor Bloom’s letter published by the Haemophilia Society.
9 May 1983 paper from Dr Galbraith (director, CDSC) recommends suspending importation of US blood products.
20 May 1983 isolation of a viral particle (then called “LAV”) in Paris by Dr Luc Montagnier. It turns out to be the same as HTLV-3 and HIV.
August 1983 first death from AIDS in the UK of a person with haemophilia.
December 1983 The British Medical Journal: no evidence any factor product is AIDS-free.
23 April 1984 Dr Robert Gallo announces he has found the virus which causes AIDS.
CDC Centers for Disease Control, US
CDSC Communicable Disease Surveillance Centre
AIDS was unrecognised in the Western world until 5 June 1981, when the Centers for Disease Control and Prevention (“CDC”) in the US reported a cluster of five cases of people suffering from a failure of their immune systems, allowing a form of pneumonia (pneumocystis carinii pneumonia (“PCP”)) to develop. The cluster was in the gay community. Its discovery has elements of a detective story. The CDC had control over the supply of pentamidine. This was a drug used specifically to treat PCP. There was not much call for it across the US – until reports arrived of a spike in demand for it in Los Angeles. So the CDC investigated: Why there? Why all at once? What they found was that those who needed pentamidine were all men in early middle age. They had been previously healthy. They had no clinically apparent, underlying immunodeficiency. Yet their immune systems had failed to prevent PCP taking hold. The alarm bells sounded. There was initially a widespread view that what caused this must be something associated with “a gay lifestyle”, for apart from age and living in Los Angeles this was the one factor which they shared in common. [323]
The CDC inquired further. Four weeks later the CDC reported in the Morbidity and Mortality Weekly Report (“MMWR”) that it had found approximately 10 more such cases, again amongst gay men, and in addition 26 cases of gay men who had developed Kaposi’s sarcoma (“KS”), a skin lesion, which had been diagnosed within the previous two and a half years.[324]
By August 1981, an additional 70 cases of PCP and KS amongst gay men were reported; and by December 1981 the same failure of the immune system which gave rise to these characteristic opportunistic infections was seen in intravenous drug users.[325]
By March 1982, the possibility that the cause of AIDS was an infectious agent had developed as a leading hypothesis: the CDC investigators then reported as much to the Food and Drug Administration (“FDA”).[326] The CDC had experience of the way in which Hepatitis B was transmitted by blood, and by sex. The CDC saw the same epidemic pattern emerging when in the MMWR of 16 July 1982 it reported three cases which had been confirmed in people with haemophilia who had developed AIDS.[327]
This report had not come completely out of the blue. William Srigley of Cutter Pharmaceutical was aware before then (“very early”) that a homosexual donor who was hepatitis positive risked transmitting AIDS.[328] Dr Henry Kingdon, vice president and general manager at Hyland Division, recorded in January 1983 that they had been closely monitoring AIDS since December 1981.[329] Thus, in early 1982 at least two pharmaceutical companies could see that if the cause of AIDS was an infectious agent then blood – and therefore blood products – might transmit it. Their actions show they were not certain that an infectious agent could be ruled out. Moreover, the finding of three people with haemophilia who had developed AIDS was what the CDC expected having itself thought that an infectious agent was likely: for they saw the disease spreading in the same way as an earlier epidemic of Hepatitis B had done. Dr Bruce Evatt’s first-hand account shows the first report of signs of AIDS in a person with haemophilia came in early 1982 and then the question was what characteristic did people with haemophilia, Haitian immigrants to the US, intravenous drug users and male homosexuals share, for it seemed there would have to be a circumstance common to all.[330]
News of the spread of AIDS to people with haemophilia, and no other apparent risk factor, predated 16 July by some days. The CDC director and Assistant Surgeon General of the US wrote to all haemophilia centres to alert them to this on 9 July 1982, and to ask that they report any case of PCP amongst their patients.[331] On 14 July the National Hemophilia Foundation in the US alerted its members that there was a risk to people with haemophilia.[332] Dr Harold Gunson in the UK was alerted to this development, shortly before 16 July 1982, in his capacity as consultant adviser on blood transfusion to the Chief Medical Officer. The Department of Health and Social Security (“DHSS”) thus had knowledge of it even before those who read the MMWR in the world as a whole were told by the publication.[333]
Although the similarities with the way Hepatitis B had spread suggested a viral aetiology, the precise cause of AIDS remained elusive. Although the exponential growth from month to month was suggestive of an epidemic, no infectious agent had yet been discovered. A number of possibilities were advanced to explain why the immune systems of those who later developed AIDS had begun to fail. The first five victims identified were all linked by the fact that they were gay.[334] Some suggested that the use of amyl nitrite poppers, which were regularly used in the gay community to heighten sexual experience, might have had a role to play.[335]
The “S” in “AIDS” stands for “syndrome”. A syndrome is a combination of a number of characteristic illnesses: none is sufficient on its own for a clinician to diagnose with any confidence a failure of the immune system from any particular cause. It was noted that those people with haemophilia who appeared to have developed the syndrome did not, usually, show signs of KS as part of their mix of illnesses. It was suggested that the failure of their immune system might have been because it had slowly been worn down by having to cope with an excess of foreign protein.[336] This was because the rapid expansion of home therapy with factor concentrates, and the sporadic giving of it prophylactically to protect an individual from future bleeds rather than simply to respond to a current bleed, meant that their bodies had been exposed to a much greater range of proteins than others had experienced previously when the treatment regime involved mainly cryoprecipitate. The factor concentrates supplied were not “pure” (in the sense of being free of any protein other than the factor of interest). They contained “foreign” fibrinogen and fibronectin in particular. So, the exponential growth in demand implied that individual immune systems had a far greater load of “foreign” protein to cope with, and some could not manage it. Other suggestions too were advanced, such as a link with cytomegalovirus, though with less general support.
By June 1982 what was known about AIDS was already a principal subject of international scientific concern. In that month, the Second International Symposium on Infections in the Immunocompromised Host was held in Stirling, Scotland. Few haematologists attended, though Dr Ian Hann, and (he thought) at least one representative of the Scottish National Blood Service, did.[337] The meeting was shocked by developing information about AIDS.[338] Dr Hann left the conference realising that it might be relevant to haemophilia patients, and later was to comment that what he heard was “a bombshell” in terms of the nature and severity of the new disease. Though the central focus of the conference was not haematology, his evidence was that it filtered through – he called it “part of the burgeoning knowledge that began to explode at that time.”[339]
By the end of July 1982 the US Public Health Service had set up a Committee on Opportunistic Infections in People with Hemophilia, to consider whether the use of certain blood products placed them at risk of developing AIDS. Three of the leading pharmaceutical producers attended an open meeting of the Committee together with representatives of the CDC.[340] The Committee concluded that AIDS was probably caused by an infectious agent, but it was unclear whether people with haemophilia were at risk. It recommended conducting studies, and that techniques be developed urgently to reduce the risk of infection from Factor 8.[341] Though it was not yet certain that AIDS was caused by an infectious agent, this was a clear recognition that at least a risk existed that this was the case.
It was certainly the view taken by the journal Science, which in August 1982 carried an article headed “New Disease Baffles Medical Community”. It described how more than 470 people in the US had AIDS, that almost half had died, and that an infectious agent appeared likeliest to be the cause. Ominously, it noted that the signpost “opportunistic” infections were first noticed in mid 1979[342] – ominous, because it suggested that if the cause was an infectious agent it had a long incubation period.
By September 1982, the US Committee had concluded that there was not enough data to suggest that immediate action should be taken in respect of licensed blood products.[343] However, on 3 October 1982 the US National Hemophilia Foundation urged pharmaceutical companies to stop using plasma collected from gay men, intravenous drug users and people who had recently been in Haiti for the manufacture of coagulation products as a “precautionary measure”.[344]
Pausing there, it is clear that in late 1982 steps were being suggested in response to the threat of AIDS to reduce the risk that factor concentrates might have been transmitting it.[345]
The debate in the US did not go unnoticed in the UK.[346] There had been the Stirling conference, mentioned above, in June 1982. As early as 16 July, Stanley Godfrey of the DHSS wrote an internal memo alerting the Medicines Division that he had been warned there might be adverse publicity about the risks of using US Factor 8 concentrates: it was being said that “400 haemophiliacs in the USA have exhibited signs of the virus” and that the licences of certain manufacturers of imported blood products might have to be revoked.[347] The Communicable Disease Surveillance Centre (“CDSC”) took steps to introduce national surveillance for AIDS in August 1982.[348]
On 5 November 1982 Dr John Craske of the Public Health Laboratory Service wrote a short report about the AIDS outbreak. He put forward three possible causes only to discount the first two (the use of amyl nitrite and the immunosuppressive effects of cytomegalovirus (“CMV”)). The third was an infectious agent. Of note, he concluded that there was a delay between symptoms emerging and diagnosis, and that as symptoms began to develop they might not be specific. He also concluded that mortality after the first development of symptoms was high (around 50%).[349]
Given this history, there can be little doubt that possibly by March 1982, and certainly from July 1982 onward, it was known in the UK to both some clinicians and some within government that there was a real risk that blood, and blood products in particular, might transmit the cause of AIDS. A wider audience was informed through The Observer, which in November 1982 reported that people with haemophilia in the US were suffering from AIDS and that there was a “major speculation” that the AIDS virus was “carried in the blood”.[350] Though there was no certainty as yet, the risk that this was the case was clear.[351]
In December 1982, a report was received of a baby who had received multiple transfusions shortly after birth, who had contracted the symptoms of AIDS and died aged two. One of the donors whose blood was transfused into the baby had been identified since the transfusion as having contracted AIDS.[352] Since plainly a baby could have neither a homosexual lifestyle, nor have been regularly exposed to an overload of foreign protein, nor used amyl nitrite, and was not born with a primary immune deficiency,[353] this – “the San Francisco baby case” – was powerful evidence in support of the infectious agent theory. The same MMWR disclosed that the three individuals whose cases had been reported in the 16 July 1982 MMWR had since died, and that four additional cases of AIDS in haemophilia patients had been identified, together with a further “highly suspect” case of a seven year old child with severe haemophilia. All had received Factor 8 concentrates and two of the five had died.[354]
The reality of the risk as it was there to be seen is underscored by the fact that on 29 December 1982, Edward Cutter, of Cutter Pharmaceutical, advised in an internal memo that his firm should thereafter include an AIDS warning in the product leaflets which accompanied its factor concentrate product.[355]
By the end of 1982, Dr Joseph Smith, the director of the National Institute for Biological Standards and Control had formed the view that the cause of AIDS was almost certainly a virus;[356] and according to Dr Charles Rizza, all UK Haemophilia Centre Directors’ Organisation (“UKHCDO”) directors knew there was a real risk that AIDS could be transmitted by an infectious agent carried by blood products.[357]
In the Netherlands, the Central Laboratory of the Blood Transfusion Services was convinced by the end of 1982 that people with bleeding disorders were at risk and started to coordinate a response with the Netherlands Haemophilia Society, haemophilia clinicians and the Netherlands National Institute for Public Health and Environmental Protection.[358] The medical director of the Central Laboratory, Professor Willem van Aken, was asked about this decision by the Lindsay Tribunal and said: “We struggled at that time … and in the end, we thought that it would be absolutely utterly irresponsible not to do it if there was a serious risk. So of course we agreed that at that time the evidence was still limited but on the other hand, there was strong indications that there was indeed a significant risk.”[359] He also said that at the end of 1982 the Central Laboratory recognised that they needed to take steps to exclude high-risk blood donors.[360]
A viral cause was further implicated on 7 January 1983, when the MMWR reported that two female sexual partners of males with AIDS and four female sexual partners of intravenous drug users had developed either AIDS, or PCP, or opportunistic infections typical of AIDS: in short, the cause was highly likely to be viral, transmissible by sex as well as blood, and similar to Hepatitis B.[361]
On the same day Alpha Pharmaceutical issued a press release, which said: “The evidence suggests, although it does not absolutely prove, that a virus or other disease agent was transmitted to them in the Factor VIII concentrate, derived from pooled human plasma”.[362]
The New England Journal of Medicine, a prestigious, widely read US medical journal, carried an editorial in its 13 January 1983 edition which stated: “The fact that haemophiliacs are at risk for AIDS is becoming clear. If the use of cryoprecipitate will minimize this risk, the current home-infusion program needs to be revised.”[363]
A Hepatitis Working Party which had been set up some time earlier by the UKHCDO met within a week of The New England Journal of Medicine editorial. This and another article in the same edition of The New England Journal of Medicine were discussed.[364] Dr Craske reported on what he had found out from the CDC: in the US there were now ten cases of AIDS in people with haemophilia of whom five had died. All had been treated with Factor 8 concentrate. The youngest was seven. “It seemed possible that factor VIII or other blood products administered to these patients might be implicated.” The CDC was working on the hypothesis that AIDS was caused by an infective agent, possibly a virus which attacked T-cells. This gained further support from the fact that there had been three cases of AIDS following transfusion of whole blood or platelets (one of which was that of the “San Francisco baby”). The incubation period ranged from six months to three years.[365]
On 24 January 1983, 21 haemophilia doctors, together with Professor Arie Zuckerman and Dr Craske, met a team from Immuno Ltd of Vienna, led by Dr Hans Eibl. The meeting, at Heathrow, lasted most of the day. It was chaired by Professor Arthur Bloom. Though the focus of the meeting was centrally on whether Immuno had found a chemical method which might inactivate non-A non-B Hepatitis and Hepatitis B in blood products, the afternoon session was given up to a discussion about AIDS.[366] No one appears to have questioned that it was likely to result from the transmission of a transmissible agent (though there was some question whether there might be more than one).[367] Importantly for understanding the risks if factor concentrates were responsible, Dr Craske informed the group that:
The meeting was also told that studies reported in The New England Journal of Medicine showed that it was more likely that those people with haemophilia who were currently without symptoms but who had received factor concentrates had abnormalities of the T-cells of their immune system, whereas those who had received cryoprecipitate did not.[369]
An article in The Lancet of 29 January 1983 concluded that a blood-borne agent seemed likely to be the cause of AIDS.[370] The New Scientist of 3 February 1983 reported that the “prime suspect” was a blood-borne virus.[371] On 4 February 1983 The Journal of the American Medical Association reported under medical news both that: “During the past year, evidence has accumulated to suggest that the lethal and mysterious acquired immunodeficiency syndrome (AIDS) can be spread by infusion of blood and blood products”, and that “all major suppliers currently have licenses pending with the FDA to market new preparation methods that may result in lowered infectivity, such as heat-treated Factor VIII concentrate products.”[372] The Deutsches Ärzteblatt (German Medical Gazette), distributed to all physicians in Germany, carried a report on 18 February 1983 from the Robert Koch Institute in Berlin that AIDS appeared to be caused by an unknown infectious agent transmitted through blood and blood products.[373]
By this time, Dutch patients had been advised that “AIDS is a very serious condition with a long incubation time. It is not yet possible to detect carriers or persons in which the disease is in the early stage. This makes it necessary to develop a policy so that the risk for haemophilia patients to be contaminated by this disease is as small as possible.”[374] Dutch physicians treating haemophilia patients agreed to use only cryoprecipitate in children under four and newly diagnosed patients, desmopressin (“DDAVP”) for patients with mild or moderate Haemophilia A or if necessary cryoprecipitate, but for all other patients to consider cryoprecipitate as the treatment of choice followed by locally produced (small pool) Factor 8 and Factor 9 concentrates.[375]
On 4 March 1983 the CDC reported that blood products or blood appeared responsible for AIDS among haemophilia patients who required clotting factor replacement. It noted that the first signs of AIDS might take two to three years to emerge after exposure to a possible transmissible agent, and that 60% of those who had a diagnosis of AIDS for more than one year died. It also observed that it looked as if the agent was transmitted only by sex or blood, and that person-to-person contact did not transmit the causative agent.[376]
The Canadian Hemophilia Society Medical and Scientific Advisory Committee advised in late March 1983 that people with haemophilia switch from Factor 8 concentrate to cryoprecipitate whenever feasible.[377]
By April in the Netherlands, the Dutch Red Cross had secured agreement that high-risk donors from the homosexual community would not donate blood.[378]
The risk that Factor 8 concentrates might transmit the cause of AIDS was recognised by the FDA: it recommended that all blood and plasmapheresis centres should inform donors about AIDS and ask donors in high-risk groups (Haitians, male homosexuals, intravenous drug users, men who have sex with men, those with signs of AIDS, sexual partners of each of these) not to donate. Products from donations made before this had to be labelled to indicate this.[379]
Some haemophilia doctors in the UK began to check patients for signs of AIDS as a routine measure: doing this conveys that they must already have recognised that receiving factor concentrate therapy carried a real risk of leading to AIDS.[380] The evidence is that those directly engaged in the process by which concentrates were derived from blood (fractionators) thought it likely that AIDS was caused by a blood-borne virus.[381]
Professor Bloom wrote to Dr Evatt of the CDC to seek information about AIDS in the US and on 7 March 1983 Dr Evatt replied. He told Professor Bloom that the AIDS epidemic was evolving “with a frightening pace”: there were now 13 confirmed AIDS cases in the US among people with haemophilia (one with Haemophilia B), and a further five highly suspect cases under investigation; the clinical course was rapid after the appearance of an opportunistic infection; all had had Factor 8 concentrates and AIDS had developed in people both with mild and severe haemophilia. The ages ranged from 7 to 62 years. Preliminary data suggested that half the population of people with haemophilia in the US had T-cell abnormalities, and 13% were markedly abnormal, as in AIDS patients. So far as transfusion in the absence of haemophilia was concerned, approximately 12 patients had developed AIDS. Half were male, half female.[382] There is no evidence that Professor Bloom circulated the letter at the time. Given what he was to go on to say, it is to be inferred that he did not.
Dr Evatt’s letter probably informed Professor Bloom’s remarks when he raised AIDS at the end of a meeting of the Central Blood Laboratories Authority (“CBLA”) on 23 March 1983, though his words appear to have been an inaccurate summary of what he had been told. Dr Richard Lane, director of the Blood Products Laboratory (“BPL”) recorded:
“Professor Bloom drew to the attention of the CBLA … the problems that are becoming associated with blood transfusion and blood product administration with the increasing incidence of reported AIDS cases which continues to gain momentum in the United States on a monthly basis. The high mortality in reported cases is a cause for concern and is a primary factor behind what is described as the American over-reaction to the problem. The aetiological factor or factors remain unknown.”[383]
Dr Lane told his colleagues at BPL: “patients … are evidently concerned and resistance against the use of imported American coagulation factor concentrates is becoming apparent. Equally, there is a likelihood that a return to cryoprecipitate as a desirable form of treatment may become irresistible, whether logical or not”. He noted that many regional transfusion centres had not made cryoprecipitate for some time and so wanted to discuss “strategic alternatives at BPL for manufacturing small pool freeze dried cryoprecipitate to offset the requirement for manufacturing at [local] level.”[384] However, production of small pool freeze-dried cryoprecipitate by BPL was ruled out “on logistic production considerations” and BPL adopted a “wait and see” policy with continued manufacture and also research into viral inactivation.[385]
Since the previous autumn, it had been known that the number of people known to be suffering from AIDS in the US doubled roughly every six months.[386] The disease was recognised as being epidemic in form. Because of the limited chances of survival if it developed, public concern was heightened. Though this chapter, and this Report, focus centrally on transmissibility by blood and blood products, it is important to see actions (or failures to act) in the context that a much larger number of people than those infected through blood and blood products suffered from AIDS in the UK. The Terry Higgins Trust was already set up, and on its way to becoming “reborn as a formal organisation”, known as the Terrence Higgins Trust, in August 1983 and the Scottish AIDS Monitor was also set up that summer.[387] UK citizens had already died of AIDS.[388]
It was at the end of April and the beginning of May 1983 that concern about AIDS and its causes intensified in the UK. On 25 April 1983 the BBC screened an hour-long Horizon programme, Killer in the Village, which identified “the 4 Hs” in the major risk groups – “Homosexual males, IV Drug (Heroin) users, Haitians and Haemophiliacs”.[389]
The press had also taken note. There was a flurry of reports in mainstream publications at the start of May 1983. The Observer said that the AIDS disease, “characterised by a collapse in the body’s ability to fight infection, is a medical time-bomb for Britain. Although only 15 cases have been reported since it first crossed the Atlantic in December 1981, many more people could be harbouring it, for the incubation period is up to three years.” It drew attention to a suspected case in a patient with haemophilia in Cardiff.[390] The Mail on Sunday “revealed exclusively” that two cases of AIDS in people with haemophilia treated in the UK with plasma imported from the US were already suspected.[391] The following day The Guardian again said that there were two cases of AIDS amongst people with haemophilia in the UK,[392] the Daily Mail referred to the possibility that Britain was importing blood products from the US “contaminated with the killer homosexual disease AIDS”, and the Daily Express called AIDS “The new killer-disease”.[393]
Despite all this, on 4 May 1983 a statement from Professor Bloom, who was in charge of the Cardiff Haemophilia Centre, and chair of the UKHCDO, and who had been asked by the Haemophilia Society for his view on the media furore, was sent to Haemophilia Society members. He said that the “cause of AIDS is quite unknown and it has not been proven to result from transmission of a specific infective agent in blood products”, that the number of AIDS cases was small, that “in spite of inaccurate statements in the press” he was unaware of any proven case in “our own haemophilic population”, and that none had been reported from Germany despite the fact that it consumed more commercial factor concentrate than any other European country. He appeared to suggest that the licensing system for blood products was such that any significant risk would have been picked up, and permission for those products to be distributed any further would be refused.[394] He advised no change to therapy with factor concentrates.
Saying that the number of AIDS cases was small was a surprising thing to write without any qualification: it may have been true that the number of people with haemophilia known (so far) to have developed AIDS was small, but the popular press were already reflecting a considerable concern that a deadly unidentified disease was growing amongst the general population in epidemic form.[395] If this was the case in the US, it was likely also to be the case in the UK; if it was the case in relation to the general population, it was likely to be the case in respect of people with bleeding disorders.[396]
This was a surprising letter for Professor Bloom to write for other reasons too. The press had reported that there were two probable cases of AIDS, one of whom was in Cardiff. As far as the Cardiff case was concerned, the report was true, and Professor Bloom had reported the case a week earlier as a probable one of AIDS to the CDSC.[397] Further, the first German person with haemophilia and AIDS died in 1982.[398] Reports of two German patients with AIDS became known during 1983, by late April.[399] Third, Professor Bloom ought to have realised that the number of cases in which the infection had become sufficiently developed to show themselves as cases of AIDS were potentially only the tip of a very much larger iceberg: The Observer had made this very point in terms clearly understandable by a layman let alone a scientist.[400] He ought to have realised this not just because of the clear terms in which the Sunday newspaper spoke, but also because of the particular knowledge he personally had been given. He had written to Dr Evatt at the CDC earlier in 1983, to ask about the spread of AIDS in people with haemophilia. In his reply Dr Evatt gave him the grim details set out above.[401] What Dr Evatt was saying should not have come as any great surprise: it repeated the essential messages which Professor Bloom and his colleagues had been given on 24 January in their meeting with Immuno at Heathrow.[402] It was wholly in line with the report Dr Craske had given to the UKHCDO Hepatitis Working Party on 19 January – a meeting to which Professor Bloom had specifically been invited.[403]
Further, it is to be inferred from the evidence given to the Inquiry that Professor Bloom may have been saying one thing for public consumption, whilst taking a different tack within his own haemophilia centre. This inference arises from four facts. First, in January 1983 a medical registrar in Professor Bloom’s team in Cardiff responded to a patient with haemophilia who, prompted by his knowledge of what the New Scientist was publishing, had raised with the registrar whether taking commercial factor product risked AIDS. Rather than disagree with his patient, say there was no good evidence that that was the case, and tell him that he should continue to take commercial factor concentrates, the registrar recorded that he was “well-read”.[404] The inference is that whatever may have been said for general public consumption by the leader of the unit, the risk that AIDS might be transmitted by commercial factor product was regarded within that unit as a real and serious risk. Second, on 18 May 1983 – only two weeks after his letter to the Haemophilia Society – Haemophilia Treatment Policy Guidelines for use in Cardiff were issued. They advised using DDAVP, cryoprecipitate and only NHS factor concentrates for children and those with mild haemophilia, and even when it came to those with severe haemophilia advised using only NHS concentrate for those who had never received commercial concentrate “where possible” and cryoprecipitate for in-patient treatment “where feasible”.[405] This can only have been on the basis that imported factor concentrates created such a risk of AIDS that they should not be used unless there was no alternative.[406] Third, he had already written a letter on 18 February 1983 to his patients saying in respect of AIDS that “the occurrence of these illnesses has been extremely uncommon and has been confined to the United States” which not only was wrong, but then suggested action which can only have been on the basis that he did consider there was a real risk rather than there being nothing to worry about.[407] Fourth, and possibly most compelling of all in revealing Professor Bloom’s two-faced approach, is that he had informed the Public Health Laboratory Service that one of his patients probably had AIDS whilst suggesting to the Haemophilia Society (and in a number of meetings) that there was no proven case of AIDS in the UK population.[408]
If what Professor Bloom had said had been faithful to the facts, and he had advised the Haemophilia Society that although it had not finally been established that there was a real risk that taking factor concentrates risked contracting AIDS, the likelihood of the risk becoming a certainty appeared to be growing stronger by the month, it is not difficult to see that the events that followed might have taken a different turn.
Dr Joseph Smith had been alerted, probably by the FDA’s request in March 1983 to the American fractionators not to accept plasma from high-risk donors, to a need to discuss AIDS in order to advise the licensing authority. Whether it was this, or press reporting that was the cause, word appears to have got round that there was a possibility that the UK might move to suspend the importation of commercial concentrates, at least in the short term. On 4 May, the day of Professor Bloom’s letter, the Association of Scientific, Technical and Managerial Staffs whose members staffed the NHS blood product facilities in Elstree, Oxford and Edinburgh called for a ban on the importation of blood products because they derived from sources likely to be rife with AIDS.[409]
Five days after Professor Bloom’s letter, Dr Spence Galbraith, who was the director of the CDSC for England and Wales, wrote a paper entitled Action on AIDS. He sent it to the DHSS. He said: “I have reviewed the literature and come to the conclusion that all blood products made from blood donated in the USA after 1978[410] should be withdrawn from use until the risk of AIDS transmission by these products has been clarified.”[411]
This view – that the risk from importation of commercial factor product was so serious that it should be suspended – proved controversial. On the very same day as Dr Galbraith wrote to the DHSS, the co-ordinator of the Haemophilia Society[412] wrote to the Medical Advisory Panel of the Society to say that “a group of us will be meeting with Geoffrey Finsberg … [to seek, inter alia, an] assurance that there will be no immediate ban on the importation of US blood products.”[413]
A special meeting of UKHCDO reference centre directors was convened on 13 May 1983. Though it considered it was “circumspect” to use only NHS materials to treat young children and people with mild haemophilia, it minuted that there was “as yet, insufficient evidence to warrant restriction of the use of imported concentrates in other patients in view of the immense benefits of therapy. The situation shall be kept under constant review.”[414] Dr Diana Walford from the DHSS attended the meeting. In a memo of the same day she recorded that she regarded Dr Galbraith’s recommendation as “premature in relation to the evidence and unbalanced in that it does not take into account the risks to haemophiliacs of withdrawing a major source of their FVIII supplies”, and plainly preferred the conclusion of the UKHCDO directors.[415]
The background was this. Measures were being taken in the US to reduce the risk posed by the concentrates made there. The FDA had asked pharmaceutical companies in March 1983 to take steps to ensure that donors in risk groups (sometimes referred to as “the 4 Hs” – homosexual males, people from Haiti, intravenous drug users (the “H” stands for heroin addicts) and people with haemophilia)[416] avoid donation. It had asked those commercial companies to label their products to indicate whether they had been produced from plasma collected before these recommendations were implemented by the industry.[417] Secondly, also in March, the FDA had licensed Hyland Laboratories to market dry-heated concentrate.[418] Though the risk which the heating process had been intended to address was that of hepatitis, it was widely thought that if the cause of AIDS was indeed a virus, it too might be inactivated by the heat treatment. These two measures indicated that in the US there was not only known to be a risk, but it was a risk of such magnitude as to merit a regulatory response. By way of comment the principle in play should have been to ask – was there a real risk of cause and effect? If yes, then can we be certain that that risk has been reduced to a level at which no further precautions are needed. The principle was not – can we be certain there is cause and effect, and is there a chance these precautions might lessen the chances of the effect?
The voices urging the avoidance of the risk from imported concentrates increased in volume and authority. The Council of Europe Committee of Experts on Blood Transfusion and Immunohaematology was due to advise the Council of Ministers who were meeting in June. Prior to its meeting in May, it sought details from each member state as to the number of AIDS cases there had been. The answer as at 28 April was that Spain reported three cases in people with haemophilia, Germany two, Austria one suspected case, and Finland one suspected retrospectively after the person’s death.[419] In May the Committee concluded that although “Absolute proof that AIDS is caused by a transmissible infectious agent is not yet available” nonetheless “the consensus in the Committee was that it should be regarded as such and that a recommendation should be made to the Council of Ministers at the meeting in June to take necessary steps to minimise the transmission of AIDS by the transfusion of blood products.” It advised avoiding the use of coagulation factors prepared from large plasma pools except when such a product was specifically indicated for medical reasons, and it advised informing physicians and “selected recipients, such as haemophiliacs” of the “potential health hazards of haemotherapy and the possibilities of minimising these risks”together with pursuingthe“rapid and full implementation” of recommendations made earlier urging a need to attain self-sufficiency in blood product production from voluntary non-remunerated donors.[420]
The directors of the Scottish National Blood Transfusion Service prepared a leaflet regarding the risk of AIDS, identifying people with haemophilia amongst the classes of those who could get AIDS:[421] in other words, accepting that there was a risk of transmission by blood products.
On 23 June 1983 the Council of Europe followed the recommendations of the Committee of Experts.[422]
By July, Transfusion International, a journal directed to transfusionists, observed in an editorial by an eminent physician that:
“There is relatively strong evidence indicating that [AIDS] may be transmitted by blood. In the United States, it is reported that eleven haemophiliacs have contracted AIDS, and additional haemophiliacs with AIDS have been observed in Europe. There is a suspicion that commercial Factor VIII concentrate, prepared from large pools of US plasma, has been the source of infection. Although there is no absolute proof that blood really does transmit AIDS infection, there is one case where the causal relationship is highly suggestive.” [The editorial went on to describe the case of the San Francisco baby.][423]
It was on 13 July that the question whether the UK should suspend the importation of foreign concentrates was to come for formal consideration before the Biological Sub-Committee of the Committee on the Safety of Medicines met. In advance, Dr Leslie Keith Fowler of the Medicines Division prepared a paper for the Committee to consider. He dated interest in KS and PCP infections as having started “three or four years ago” (thus 1979-80), described AIDS as “clearly a transmissible condition”, but thought that “repeated exposure to allogeneic sperm together with cytomegalovirus (CMV) over a prolonged period impairs T cell mediated immunity, allowing reactivation of Epstein Barr virus” was the likeliest cause. He concluded that AIDS might be a “function of the concentrate itself rather than a specific agent”. This contribution shows that there was as yet no unanimity as to the cause of AIDS, though it has to be said that his particular theory was very much his own. It was undoubtedly heterodox. However, he also said, on firmer ground, that “The media concept of a ticking time bomb is a very real one for haemophiliacs and no effort should be spared to protect them by all practical means.”[424]
The Sub-Committee decided not to recommend that imports be suspended. The correctness of this decision is considered in the chapter on Regulation of Commercial Factor Concentrates: for the purposes of this chapter, however, the first conclusion it reached was: “The cause of AIDS is unknown, but an infectious aetiology seems likely. A previously unrecognised or new agent may be responsible, but repeated exposure to, or reactivation of, known agents, (eg CMV, EBV) may be involved.”[425]
Also in July 1983 Dr Michael Rodell, who was the vice president (regulatory and technical affairs) of Armour Pharmaceuticals and representing the Pharmaceutical Manufacturers Association, told a standing committee advising the US Secretary of State of Health and the Commissioner of the FDA that on average persons who were paid for their plasma had it collected between 40 and 60 times per year.[426] At that rate, and given the pool sizes used for the manufacture of concentrates in the US, his presentation suggested that four infected persons could contaminate the entire world supply of Factor 8 concentrate.[427] It is clear that pharmaceutical companies regarded the risk that factor concentrates might transmit AIDS as real and substantial.[428]
Well before the autumn of 1983 the frontrunner among the postulated causes of AIDS had been an infectious agent. The strength of evidence and opinion supporting this hypothesis kept on increasing thereafter. The isolation of a viral particle (then called “LAV”) by Dr Luc Montagnier and his team in Paris on 20 May 1983[429] did not attract significant attention at the time, but was later said to have made it clear scientifically that the cause of AIDS was indeed a virus,[430] though there remained some suggestions until early 1984 that injection of foreign proteins could be a causal or contributory factor. Though there were many who were alert to the publication on 20 May 1983 of his findings, there were few wider references to its importance.
In mid August 1983, the Medical Research Council produced a Brief on AIDS in which it said: “Over the last six months the possibility of transmission by blood transfusion has become increasingly apparent … An infectious agent has therefore been implicated which is sexually, parenterally and even perinatally transmitted with a long asymptomatic infectious incubation period … Transmission of AIDS by transfusion and blood products may become a serious problem.”[431]
Underscoring these last few words was the first known death in the UK of a person with haemophilia with AIDS. He died in August 1983, having been unwell since he received commercial concentrate some months earlier.[432] Nonetheless, when UKHCDO held its annual general meeting on 17 October, and despite the death which was widely reported in the national press,[433] Professor Bloom felt able to treat a suggestion that patients should revert to having cryoprecipitate by saying that “he felt that there was no need for patients to stop using the commercial concentrates because at present there was no proof that the commercial concentrates were the cause of AIDS.”[434]
By December 1983, an article in The British Medical Journal commented that there was no evidence that any factor product, whether made from purchased or voluntarily donated plasma, was free from the risk of transmitting AIDS.[435] By way of comment, if the question had been put in this form at the start of 1983 – “is there any evidence that any product is free of the risk of transmitting AIDS?” – the answer would have been the same. None. The question should have been asked in that form once it became clear that there was a real risk that concentrates might transmit the cause: it should have been asked before the end of 1982.
On 12 January 1984 The New England Journal of Medicine published a report of a study of 18 suspected cases of AIDS associated with transfusion. None of the recipients possessed any risk factor other than being the receipt of blood components. The conclusion of The New England Journal of Medicine was that blood components could transmit AIDS, that exposure to one infected unit might result in transmission, and that symptomless donors could be infectious.[436] Dr Thomas Zuck, who was later to be the director of the blood and blood products division of the FDA, told the Krever Commission that the effect of the study was to “put the whole medical community and perhaps the world on notice that AIDS is transmitted by blood transfusions.”[437]
By March 1984 all blood products manufacturers in the US warned of the risk of contracting AIDS from using their products.[438]
One of the seminal dates was that of the identification of the virus which led to AIDS. Though Dr Montagnier had reported in May 1983 that he had isolated a viral particle in association with AIDS,[439] when Dr Robert Gallo in the US held a press conference on 23 April, and published on 4 May, and claimed he had found the virus which caused AIDS, terming it “HTLVIII”,[440] the scientific and medical community now took notice. Indeed, there was an element of theatre about the announcement – the US Secretary of State for Health came to a press conference at which Dr Gallo’s discovery was announced, and predicted that the test would be widely available within six months to screen blood to exclude the virus.[441] In fact, Dr Gallo had identified exactly that which Dr Montagnier had called LAV. However, from now on the overwhelming consensus was that the cause of AIDS was infection with HTLV-3 (LAV) which was later renamed HIV.
In summary, the risk that blood transfusion or use of factor concentrates could cause AIDS (and hepatitis, mainly non-A non-B Hepatitis) was apparent in mid 1982. All those involved in treating patients with blood or blood products either knew, or should have known, of the risk by the end of 1982. It became increasingly apparent as a serious risk until it came to be regarded as a near certainty in April 1984. This risk (that transfusion or factor concentrates could transmit the cause of AIDS) had to be addressed when it first became recognised as a real risk, by the end of 1982 or January 1983 at the latest; all the more so when it became a near certainty, and all the quicker since the context was known to be a developing epidemic.
This chapter provides an account of how knowledge of AIDS arose and developed. Subsequent chapters in this Report demonstrate the reluctance of clinicians, and because of that, of the Haemophilia Society, to accept that a particular style of preparation of a product which they had strongly favoured might after all be more deeply harmful than alternatives which they had largely discounted. Later chapters demonstrate, too, elementary failures of analysis – conflating risk with incidence, failing to recognise the significance of long incubation periods, and somehow being reassured with the idea that the disease was confined to the US, rather than seeing the fact it was epidemic in the US as a red flag giving advance warning of what might happen here. There was a failure to ask the right questions: given sufficient material to show there was a real risk, was there any evidence that the products concerned were free of it? There was a lack of any sense of urgency. There was insufficient regard to developing experience, knowledge and wisdom elsewhere in the world supplied by US concentrates. And there was, over and above all, a search for certainty of cause-and-effect as if that were necessary before action should be taken.
On 3 May 1984, Professor Robin Weiss of University College London wrote in Nature that: “There no longer seems to be any doubt that AIDS is caused by an infectious agent”: the overload of foreign protein theory did not explain why single transfusions could transmit AIDS, nor how infants acquired infections from affected mothers. He commented that: “ELISA [enzyme-linked immunosorbent assay] screening tests for blood banks are urgently needed”. The word he used was “urgently”.[442]
This chapter, then, ends with an overdue call for urgency. How far that call for a screening test to be developed in the UK was answered is for a later chapter.[443]
This chapter reviews the structure and functions of the blood services as they developed throughout the UK and considers the impact of the way in which the blood services were organised.
1940 SNBTS is set up.
September 1946 Ministry of Health creates National Blood Transfusion Service for England and Wales.
July 1948 with the establishment of the NHS, RTCs are managed by regional hospital boards instead of nationally; SNBTS becomes the responsibility of the Secretary of State for Scotland.
1970, 1973 RTDs advocate a national and centrally financed and administered blood service.
1974 NHS reorganisation results in RTCs coming under the control of regional health authorities; the Common Services Agency takes over responsibility for SNBTS.
1975 Central Committee for NBTS created.
1980 Dr Tovey proposes a plan for the reorganisation of the NBTS under a central coordinating committee. DHSS establishes Advisory Committee on the NBTS.
1987 a report on the organisation of blood services recommends reform.
1988 National Directorate is set up to coordinate blood services in England and Wales. Despite name, has no executive control.
1991 Welsh Health Common Services Authority manages services in Wales.
1993 National Blood Authority is established.
1994 NIBTS is established.
1999 WBS is established.
Dr John Cash national medical director, Scotland (1979 - 1997)
Dr Harold Gunson director, NBTS (1988 - 1993)
Dr William d’A Maycock consultant transfusion adviser to the CMO ( until 1978)
Dr Morris McClelland director, Northern Ireland Blood Transfusion Service (1980 - 1994)
Dr Tony Napier medical director, Welsh Regional Blood Transfusion Service (1977 - 1998)
Dr Angela Robinson medical director, National Blood Authority (1994 - 2007 )
Dr Geoffrey Tovey consultant adviser to the CMO (1978 - 1981)
NBA National Blood Authority
NBTS National Blood Transfusion Service
NIBTS Northern Ireland Blood Transfusion Service
RTC Regional Transfusion Centre
SNBTS Scottish National Blood Transfusion Service
WBS Welsh Blood Service
As explained in the chapter on Blood and Transfusion and repeated here simply for easy readability, the Army Blood Supply Depot was established by the War Office at the start of World War Two. It operated from Southmead in Bristol. As well as meeting the requirements of the armed forces it supplied civilian hospitals in South West England. Treating London civilians in the war was to be the work of four blood depots established in 1939. By 1940, regional blood depots had also been established close to large district hospitals in the major cities and these later became known as regional transfusion centres (“RTC”). [444] The Scottish National Blood Service began on 11 January 1940, funded independently of its later English counterparts.[445]
As for blood products, the Treasury War Emergency Committee decided in 1941 to finance two facilities in the UK for the preparation of freeze-dried human plasma. One of these was established in an underground site at the Royal Infirmary of Edinburgh. The other was set up at Cambridge, under the auspices of the Medical Research Council.
By 1943, in England and Wales, it was recognised that the blood supply system had reached such a scale that national management was required.[446] The National Blood Transfusion Service (“NBTS”) for England and Wales was thus created by the Ministry of Health on 26 September 1946. There were 11 regional transfusion centres within the Service, including what were by then 2 London centres.[447] This later became 14 regional transfusion centres. It was managed directly by the Ministry of Health for a year and three quarters, advised by Dr William d’A Maycock, and a committee (which had no executive power). However, following the establishment of the National Health Service (“NHS”) under legislation which provided for regionalised medical services, the Ministry of Health no longer exercised unitary national control. Instead, regional hospital boards exercised functions with respect to the administration of hospital and specialist services in their respective regions.[448] These included blood services. Twelve such regional hospital boards were established, and the management of regional transfusion centres was transferred from the Ministry of Health to these regional hospital boards. Each regional transfusion centre was managed by a regional transfusion director who was medically qualified and was appointed by and accountable to the regional hospital board.[449]
Having been run under central executive control for a brief period until 5 July 1948 as a unitary National Blood Service it then became an amalgamation of autonomous regional services. The history of the next 46 years was one in which many concerned in collecting voluntary altruistic donations to supply blood and produce blood products sought to avoid the consequences that regional control brought in its wake. In particular, those who sought to facilitate a supply of blood products from the fractionation centres[450] argued, in increasingly strenuous terms, for a truly national system rather than one which was regionally funded, regionally directed, regionally controlled, and responsive in particular to the needs of the individual regions rather than to the nation as a whole.
Disquiet at the problems this fractured control created for a national service was recorded as early as 1954, with a sense that the service was being starved of the cash it needed to equip itself properly.[451] Nothing materially changed. By June 1961, the future of the transfusion service was the subject of discussion at a meeting of regional transfusion directors. Dr Neville Goodman, the Deputy Chief Medical Officer, chaired this discussion, and began by saying that he thought the NBTS “tended to be rather isolated from the rest of the N.H.S.”[452] The views expressed at the meeting were not unanimous, save in one respect in which several attendees raised a concern. That was that a national effort needed to be made to improve research and development. They thought that as a consequence of the regionalised arrangements this was being sadly neglected. No dissenting voice was recorded on this point.[453]
Divergences in practice remained between regional transfusion centres. Efforts to standardise the medical selection of donors and other functions were only ever partially successful (according to Dr Harold Gunson, later to be director of the NBTS, and there is no reason to doubt his conclusion in this regard) as there was no obligation on regional transfusion directors to adopt national policy, particularly where it came into conflict with regional priorities.[454]
In the early 1970s restructuring of the NHS was under active discussion. At a special meeting between regional transfusion directors and Department of Health and Social Security (“DHSS”) representatives, held in 1970 to consider a green paper on the future structure of the NHS, the directors advanced a case for the reintroduction of a national service. They complained that the existing structure of independent regional transfusion centres was leading to fragmented administration. The meeting included:
This was followed up by the directors in January 1973, when they presented a document to the Standing Medical Advisory Committee.[456] It began with the words:
“In the light of the proposed reorganisation of the National Health Service, Directors of the Regional Transfusion Centres and the two associated laboratories (Blood Group Reference Laboratory and Blood Products Laboratory) have considered the present and future structure of the National Blood Transfusion Service. They are unanimously against administration of the Centres by Regional Authorities. They strongly recommend that the National Blood Transfusion Service be reorganised round a unified system of central administration.”
In its detail the document complained that the proposal for regional control, contained in the draft statute about to be enacted, was not based on any expert opinion, but “purely in pursuit of the principle of devolution.”[457]
The National Health Service Reorganisation Act 1973[458] replaced regional hospital boards with regional health authorities. Regional transfusion centres remained under local management despite the views the regional transfusion directors had expressed. No national executive was established to control blood services policy or management.
Regional transfusion directors remained sceptical about the effectiveness of this structure. An ad hoc committee was set up to consider their concerns, and whether any change should be made in the organisation of the blood transfusion services in England and Wales. This committee, though recognising the force of many reasons for centralising administration of the national blood services, was unconvinced that responsibility for administration and providing services should be taken away from regional health authorities. Nonetheless, a degree of central coordination was thought desirable: and a Central Committee for the National Blood Transfusion Service was proposed.[459] This was created in 1975. It was to keep under review the operation of the blood service in England and Wales, including Blood Products Laboratory (“BPL”) and the Blood Group Reference Laboratory, and to advise the DHSS on the development of the blood service. This committee first met in June 1975.[460]
In April 1974, guidance was sought by the regional transfusion directors from the DHSS on the relationship between the regional transfusion centres and regional health authorities: such guidance was generally lacking.[461] By October 1974 they were still waiting. While they waited, the position was of such concern that it merited an editorial in The British Medical Journal in July 1974.[462]
The background to this editorial was that some had recently begun to argue that a voluntary system of donations did not, and could not, produce enough plasma to produce sufficient blood products domestically to satisfy the needs of patients. Hence, they argued, the gap needed to be filled by imports of blood products manufactured elsewhere. The imports were from the US, though the editorial claimed that paid donors in the US were not the only sources, and that the professional donors came “not from Leeds, Liverpool, or London, but from people in such countries as Puerto Rico, Chile, and Columbia.”[463]
In the eyes of The British Medical Journal, the reason for insufficiency of plasma was not that the public were to blame for not being sufficiently forthcoming in donating, as this argument appeared to suggest. Rather, the editorial suggested that the “shortage” of blood (allowing entry to the UK of the products made by commercial pharmaceutical companies to remedy that shortage) was not a real one but was to be ascribed to:
“the quality of management (or lack of it) which has led to a steady decline in the British Blood Transfusion Service since the late 1950s. There has been no effective national planning; the regional and protein fractionation centres now lack sufficient staff, accommodation, equipment and the basic organisational units to do the job. Moreover, the medical staff in the centres are often geographically and administratively isolated from the care of patients. The remedy, then, is … an urgent appraisal (for the first time) of a national policy for the procurement and eventual distribution of a natural resource which, unlike oil, will be still readily available in 100 years’ time.”[464]
The view of the author of the editorial appears to have been shared by Dr Maycock, whose view for many years had been that “An efficient modern blood transfusion service does not really fit at all into the pattern of the NHS.”[465] It was also and importantly shared by the then Minister of State for Health, Dr David Owen. In a parliamentary written answer within a week of the publication of the editorial he recorded that the production of Factor 8 in the NHS had increased significantly in the last few years, but that “Further increases will depend on the extent to which regional health authorities are able to expand facilities in transfusion centres for the production of plasma, from which factor VIII is derived.”[466] In short, he did not blame the public for being unwilling to come forward to donate: rather, he saw the solution in regions providing the necessary finance to expand the capabilities of regional transfusion centres in England and Wales to process their donations. It lay in the hands of the regional health authorities to enable BPL and Plasma Fractionation Laboratory (“PFL”) to work effectively in the national interest, by supplying them with greater amounts of plasma.[467]
Dr Owen was right, the author of the editorial was right, and the majority[468] of regional transfusion directors were right, in thinking that it would not have been difficult to persuade people to come forward to donate in greater numbers. Some 4-5% of the general population donated repeatedly. Subsequent evidence shows that if a real need was perceived, as during the Gulf War, this proportion would rise markedly; and almost every transfusion director who was asked about this in oral evidence confirmed that they would have expected little difficulty in increasing the number of donations if they had been required to do so.[469] Insofar as there was a brake on this, it came from the availability of finance in some regions, and a need for capital investment in premises, plant and equipment and for higher staffing levels which were often unsatisfied. These are points expressed as conclusions here: they are considered more fully below.
Proposals for reorganisation to improve the national service by the provision of central finance, and management through a committee with executive powers, remained an active concern. In 1977 the NBTS submitted to the Royal Commission on the NHS that the NBTS had assumed an increasingly national role which had suffered from constraints arising from regional development, inadequate central coordination and financing, and a poor integration of the activities of regional transfusion centres.[470] The current structure of the transfusion service was described as a “loose confederation of 14 Regional Transfusion Centres, independently financed, each providing services which vary considerably from Region to Region, and three central laboratories financed by the DHSS.”[471] The Royal Commission noted that blood transfusion was one of the services provided by regional health authorities but “common services like these do not require a regional tier.”[472]
The structure of the blood services across the UK was linked to the supply to BPL in England (and Protein Fractionation Centre (“PFC”) in Scotland, though Scottish National Blood Transfusion Service (“SNBTS”) was and is distinct from NBTS) of sufficient plasma to enable them to utilise production facilities to the full. At the same time as these oft-repeated concerns were being expressed about the difficulties caused by the fact that transfusion centres in England and Wales were administered and funded locally (regional health authorities had little incentive to provide plasma for fractionation if those health authorities were not themselves going to see a benefit for patients within their own region) BPL itself was suffering from an extended period of underinvestment. There was an accompanying lack of funds and incentive for research to be conducted into producing safer products.[473]
Until 1978 the same person was in a position of central influence in respect of both the NBTS, and the BPL (then operated by the Lister Institute) at Elstree: Dr Maycock. He was both consultant advisor on blood transfusion to the Chief Medical Officer (“CMO”), and in that capacity had some oversight[474] of the NBTS, and the director of BPL.[475] His influence was wider still: he was an honorary consultant in blood transfusion and resuscitation to the War Office, later the Ministry of Defence; had been president of the British Society for Haematology; and was a recognised teacher of pathology in the University of London.[476] He was the dominant figure in the field of blood transfusion. His standing astride both the sourcing and supply and manufacturing bodies ensured a degree of coordination between BPL and NBTS, both of which could in addition potentially benefit from the influence he could bring to bear.
Dr Maycock retired in 1978. When that happened, his roles passed into different hands. Dr Geoffrey Tovey succeeded him as consultant advisor to the CMO; Dr Richard Lane replaced him as the director of BPL. This coincided with the Lister Institute running out of the funds necessary to continue operations at Elstree (known as “BPL”, “Lister” or “Elstree”) under its own auspices. The facilities at Elstree, sadly in need of upgrading given a lack of recent investment, and which had never been designed to provide accommodation for large-scale fractionation of blood products,[477] were now to be funded jointly by the DHSS and North West Thames Regional Health Authority.[478] Though production facilities in England had never formally been part of the same service as the NBTS, and the making of blood products had always been funded separately since 1948, they might have been seen as two aspects working together under one NHS to obtain and supply blood and blood products to those in need of them. They were now not only funded differently, but very clearly managed separately, though still both within the NHS. Though there is little evidence of direct conflict between BPL (producing blood products) and the NBTS (obtaining fresh blood and plasma from donations, supplying hospitals with blood, plasma and blood derivatives, and supplying BPL with plasma),[479] this separation cannot have helped the formulation of a unitary response to these challenges.
Separation had a wider impact, too, in respect of the UK as a whole. Even whilst he was only director designate of BPL and not yet in post, Dr Lane began expressing his view that England (together with Wales) should look after itself, and BPL should be upgraded and expanded to achieve this. He opposed what had been Dr Maycock’s and the government’s previously favoured approach, with which Dr (later Professor) John Cash (Dr Maycock’s equivalent in Scotland) had enthusiastically agreed, which was to develop two production units of roughly equal capacities, one in England and the other in Scotland, to meet the needs of the UK as a whole. Though PFC in Scotland had been provided with new buildings on a new site in Edinburgh, and was designed to operate there on a 24-hour continuous process on weekdays, with a view to processing plasma harvested from the four most northerly regions in England as well as the Scottish regions,[480] Dr Lane’s voice was persuasive in ensuring the processing of northern plasma to make factor concentrates in Scotland never happened.[481] Further detail of this is given in the chapter on Self-Sufficiency.
In February 1980 Dr Tovey took up the cudgels which regional transfusion directors had previously wielded when he proposed a plan for the reorganisation of the NBTS. He complained that increased national demand had only highlighted the “constraints arising from regional development, inadequate central co-ordination and financing and poor integration of activities of Regional Transfusion Centres.”[482]
He was clear that the major defects were unlikely to be overcome without an Act of Parliament creating a committee or board with executive powers. As an “interim” measure “and as a matter of urgency”[483] he suggested that there should be a central coordinating committee for the NBTS including the chairman of the joint management committee for the central laboratories of the NBTS (which had been established shortly beforehand), the consultant advisor in blood transfusion, three regional transfusion directors, directors of the central laboratories, a regional medical officer, a regional treasurer, a representative of the joint committee, and representation from the DHSS. He suggested the committee formulate and coordinate national policy, and through its membership achieve implementation of that policy at central and regional levels. The three regional transfusion director members were expected to be the chairs of the northern, eastern, and western divisions which Dr Tovey had established within the service.
It was also apparent from what he wrote that he saw a need for closer liaison between the NBTS and the SNBTS, extending beyond effective coordination between BPL and PFC at Liberton. He commented: “My colleagues and I have agreed full national co-ordination will not be accomplished and a maximally cost-effective Service obtained until the NBTS and the Scottish NBTS are welded into a truly national Blood Transfusion Service, embracing all four corners of the United Kingdom.”[484]
The DHSS adopted his proposal (though a truly national, in the sense of “UK-wide”, service was not for it to establish since the Advisory Committee spoke for England and Wales alone) and established a new Advisory Committee on the NBTS.[485] It was, however, to be chaired by a DHSS representative. Its terms of reference were “To advise the DHSS and the Welsh Office on the co-ordination of (i) the development and work of Regional Transfusion Centres, and the Central Blood Laboratories in England and Wales; (ii) as necessary – the English and Welsh Blood Transfusion Service with that of Scotland.”[486]
A number of national[487] policies were pursued by the Advisory Committee. However, difficulties in achieving national standardisation persisted, and Dr Gunson (who succeeded Dr Tovey as consultant adviser in 1981) was later to highlight that the inconsistent and inadequate supply of plasma to BPL, and the difficulties in implementing HIV testing were examples of problems caused by a lack of an effective national policy for decision-making.[488]
In 1982, a special health authority (the Central Blood Laboratories Authority: “CBLA”)[489] was established to manage the central laboratories. Its remit included BPL at Elstree, the Blood Group Reference Laboratory, and PFL in Oxford. It did not include PFC in Scotland. In the same year the blood transfusion research committee of the Medical Research Council, which had met since 1939, was disbanded. This severed the last formal link between the national blood service and the Medical Research Council, which had once been responsible, in large part, for much of the transfusion service.[490]
By the start of 1983, therefore, the UK service was still one in which there were a number of autonomous parts: regional transfusion centres, organised in England and Wales into three districts but still consisting of individual regional transfusion centres, each under the financial and administrative control of their respective regions, and the services in Scotland[491] and Northern Ireland. The Advisory Committee on the NBTS was advisory only, and remained unable to exercise executive control over the service as a whole.
The directors of all the regional transfusion centres in England and Wales repeatedly noted that if plasma supply to BPL were to be sufficient to support the goal of self-sufficiency this required national management. The DHSS was aware too that research and development were duplicated unnecessarily across regional transfusion centres, BPL, and PFC due to a lack of central coordination; and that successful introduction of heat treatment to inactivate viruses in blood products would benefit from such central coordination.[492] By 1986 it was agreed that the organisation of the NBTS should be investigated by DHSS Central Management Services. A report followed in October 1987, which reported “wide variations in policy, procedures and functions between the regional transfusion centres with no real evaluation of performance and little effective co-ordination either between the regional centres or between the centres and CBLA.”[493] There were four major problems: the absence of useful and reliable management information; the inability of London regions to meet the needs of their hospitals; the lack of coordination between RTCs and between RTCs and the CBLA; and “Inefficiency”.[494] It identified three alternatives: (a) maintain the present system with the introduction of reliable management information; (b) create a new special health authority to manage the system centrally; or (c) retain the regional health authorities’ management of RTCs, but with formal national coordination of their work.[495] The DHSS favoured the third option. Accordingly, a National Directorate, intended formally to co-ordinate the blood transfusion services[496] in England and Wales, was set up as from 28 July 1988, funded by the Department of Health.
The National Directorate (despite its title) still lacked executive authority, which remained with the regional transfusion centres and their regional health authorities. Dr Gunson, the first national director, described it as operating by “persuasion”rather than executive power. Any policy proposal which involved the use of additional resources by regional transfusion centres was liable to create difficulty, since their budgets remained controlled by regional health authorities. He reported that the National Directorate did achieve some things: the interregional transfer of blood; the establishment of a management information system; quality assurance at RTCs, supported by audit; and “Improved blood donor recruitment and retention”. Nonetheless, he said the National Directorate was “overtaken by national events.”[497]
The NHS and Community Care Act 1990 had the effect that RTCs had to handle their operating costs through reimbursement for products and services. This inevitably led to RTCs working closely with the hospitals receiving their products and services. The National Directorate was marginalised: “the lack of executive authority became crucial.”[498] In June 1990 this led Dr Gunson to propose a fully national service with central executive management.[499] He argued that this would increase efficiency, supply and quality of blood products. At the same time, Professor Cash, who headed up SNBTS, maintained a call for more effective integration of the blood transfusion services on both sides of the border, as well as further finance for research and development in blood products from voluntary British donors. Though the Government had indicated that it respected clinical freedom, Professor Cash thought that such an approach frustrated efforts towards self-sufficiency.[500]
Individual directors at regional transfusion centres, including Drs Marcela Contreras, Fereydoun Ala and Ian Fraser wrote in support of Professor Cash, recording their concerns about the limited authority of the National Directorate, which did not have the power to formulate national policy in the light of the independent management of the RTCs.[501]
In 1991 Ernst and Young conducted a structural review of the NBTS. Their report favoured a central contracting authority (unifying the National Directorate and the CBLA) rather than a centrally managed service with direct line management. The latter was more costly.[502]
A special health authority as a “contracting authority” was therefore proposed. It was to be a central NBTS body which would agree operating contracts with regional transfusion centres as a means of managing the national service (a “contract rather than persuasion” model), which left regional transfusion centres with local autonomy. As discussions proceeded over the next 18 months it became apparent that it was impractical for the new National Blood Authority (“NBA”) to contract directly with hospitals. Instead, the conclusion was that it should become a central strategic management authority, which should directly manage both BPL and the regional transfusion centres along with the Blood Group Reference Laboratory.[503] From 1 April 1993 the Department of Health finally established a single body with executive authority along these lines, the National Blood Authority.[504] It was established as a special authority.
Thus 46 years after the last date when there had been central control of the blood transfusion system, and the production of blood products had been under unitary national control in England, during which there had been repeated calls for its reintroduction, it was finally restored.[505] In those 46 years it is probable that the way in which the service had been diversely organised, and regionally funded, with an inbuilt reluctance to fund and direct centrally, created unnecessary shortfalls in the supply of plasma to, and in the productive capacity of, BPL and rendered the achievement of self-sufficiency in the supply of coagulation concentrates much more difficult than it needed to have been. It also failed to concentrate funds spent on research, so that it might be better equipped and resourced, because funding made available for research was provided regionally, and thus both spread more thinly, and capable of duplicating efforts in another region rather than supplementing them.
As the history set out above shows, warnings to this effect were not heeded until too late.
Coordination between England and Wales, on the one hand, and Scotland on the other hand, so that there could be one unitary service was never achieved, though on an individual level there was often significant cooperation. A consequence of Dr Lane’s looking at England and Wales as a single unit, influential in an abandonment of the idea of providing for the UK as a whole, meant that PFC was not developed as it might have been to ensure sufficient supplies of product to the North of the UK and Northern Ireland while BPL concentrated on Wales, the South and the Midlands of England.
In May 1994 Dr Angela Robinson replaced Dr Gunson as national director of the NBA. Following consultation, the NBA created three administrative zones (London and the South East; Midlands and the South West; and Northern, administered respectively from North London, Bristol and Leeds).
In 2005 the NBA was replaced by NHS Blood and Transplant (“NHSBT”), a special health authority. The functions of both the NBA and the NHSBT were collecting, screening and processing and supplying blood, blood products and plasma for the purposes of the health services. NHSBT also was to supply stem cells and other tissues, and to facilitate and secure the provision of services to assist tissue and organ transplantation.
On 1 January 2011, BPL was transferred from NHSBT to become a Department of Health owned limited company: Bioproducts Laboratory Ltd (“BPLL”). This was technically a wholly owned subsidiary of Plasma Resources UK Ltd (“PRUK”), 100% owned and managed by the Department of Health.
In 2013 private sector investment in PRUK was permitted and on 18 July that year Bain purchased an 80% stake. BPLL was thus no longer under full public control. BPLL is now a privately owned company. Full privatisation was achieved when BPL’s current owners, Creat Group Corporation, acquired Bio Products Laboratory Holdings Ltd (of which BPL Ltd is a wholly owned subsidiary) from Bain and the Department of Health in 2017.[506]
The origins of the Scottish blood transfusion service echoed the way in which it began in England. A single man – in this case Mr Copland, a dentist – inspired a “group of walking donors” to give transfusions of their blood to the Royal Infirmary in Edinburgh. In 1936, the Lord Provost of Edinburgh formed a committee to take over responsibility for the service. By the outbreak of War on 3 September 1939, small blood banks had been set up in Edinburgh and Glasgow.[507] These individual initiatives led to the setting up of the SNBTS on 11 January 1940. The SNBTS consisted of five regional blood transfusion centres: Edinburgh and South East Scotland; Glasgow and West of Scotland; Dundee and East Scotland; Aberdeen and North East Scotland; Inverness and North Scotland. It was managed by a charity, the Scottish National Blood Transfusion Association (“SNBTA”). There was a national organiser, initially Mr Copland.[508]
Following the creation of the NHS in 1948 the blood service became the responsibility of the Secretary of State for Scotland. The Secretary of State took over the premises and equipment of the SNBTA, which remained an independent charitable body with an agreement with the Secretary of State underpinning its work to provide the service.[509]
By 1953, the unit set up in 1943 to produce dried plasma in support of the war effort was expanded to handle plasma fractionation.[510] It operated in premises which were on the site of the Royal Infirmary in central Edinburgh. In the early 1970s it moved to a new site in Liberton (no longer in the same building as the Royal Infirmary, though close by a new building constructed to house it which was also established on the south side of the city) and was named the Protein Fractionation Centre (“PFC”). As the name suggests, it was specifically designed for the fractionation of plasma, by contrast with its English equivalent.[511]
The agreement between the SNBTA and the Secretary of State formally ceased on 31 March 1974. In 1974, too, PFC was completed.[512] The Common Services Agency (“CSA”)[513] took over responsibility for the service, which thereafter was formally known as the known as the SNBTS.[514] The CSA was overseen by the Scottish Home and Health Department (“SHHD”) and later its successors: until devolution in 1999 the CSA was administered by the Scottish Office; since then it has been answerable to the Scottish Parliament.
Administration by the CSA, which had responsibility for a range of services other than blood supplies, led to complaints that its management committee no longer had, or had available to it, independent specialist advice about blood transfusion. Directors of the five RTCs continued to press their point, and in April 1978 this led to the establishment of a sub-committee of the CSA to be known as the Blood Transfusion Service Sub-Committee. This included specialists in clinical medicine, laboratory medicine, a medical officer from SHHD, a representative of donor interests, and the national medical director of the service who had the right to attend or be represented at each meeting.[515] Following this, in 1978, Professor Cash was appointed as the national medical director. A national headquarters research laboratory, national reagents unit, and national quality unit were also created around this time.
Although there was no formal liaison committee between SNBTS and NBTS until January 1989, SNBTS and the Belfast regional transfusion directors participated in national meetings of the regional transfusion directors in England and Wales and, reciprocally, a regional transfusion director from south of the border, or representative of the NBTS National Directorate, after that was formed, attended some meetings of SNBTS directors.[516] The Advisory Committee on the NBTS dealt with matters concerning England and Wales but the SHHD, Welsh Office and DHSS Northern Ireland were represented by observers (as well as, in the case of Scotland, by Professor Cash) who would participate fully in its discussions.[517]
In 1990 the position of general manager was created – renamed national director in 1996 – and the national medical director (Professor Cash) became the national medical scientific director. The SNBTS management board included both the general manager/national director and the national medical scientific director, and the five regional transfusion directors amongst others. It was restructured at the start of the millennium, to move away from the previous regional structure toward a national functional structure. Since then, all blood donor services have been managed nationally, whereas before they were managed regionally. Regional transfusion directors thereafter became known as clinical directors; a national quality directorate was formed, a director of operations was created to manage donor services, manufacturing and logistics, and the number of blood processing and testing units was reduced to two.[518]
The governance arrangements through the CSA were strengthened in 2003, when the SNBTS director became an executive director of the CSA board. It remained and remains responsible for the provision of supplies of human blood for transfusion and related services, but in 2008 the production of blood fractions was removed from the functions of the CSA.[519] Wider organisational change occurred in 2012/13, in which divisions of the CSA[520] were consolidated into strategic business units, and support services were centralised. SNBTS was considered of sufficient size and specialty to retain its own identity; in 2013 its “board” was renamed the Senior Management Group, chaired by the SNBTS national director, and the Medical and Scientific Committee was renamed the Clinical Governance and Safety Group, and was chaired by the SNBTS medical director. SNBTS was thereafter organised in a number of directorates: donor and transplant services; blood manufacturing, tissues cells and advanced therapeutics; patient services, quality assurance and advanced regulatory compliance; strategy, planning and performance.[521]
There have been no further significant changes to structure since then.[522]
Throughout the relevant period all funds have been provided centrally, rather than from regional budgets as was the case in England and Wales.[523]
With the start of the National Health Service, the Northern Ireland Blood Transfusion Service (“NIBTS”) became the responsibility of the Northern Ireland Hospitals’ Authority. In 1953 a new headquarters was established in Belfast.[524] In many ways, it was ahead of its time: in 1953 it started to use a mobile donation unit.
The blood transfusion laboratories were at Royal Victoria Hospital. In 1961 they moved to the Belfast City Hospital.
In 1973, when the NHS was reorganised, it merged in Northern Ireland with the broader social care system. It became called the Health and Personal Social Service and later the Health and Social Care (“HSC”) System. At that time, and indeed from 1972 until 1999, the system was managed by the UK government through the Northern Ireland Office. Public and social policy decisions were taken at Westminster, and communicated through the Secretary of State within the Northern Ireland Office. They answered directly to the UK government. In general, policy and strategy in health and social services developed in Northern Ireland to mirror English policy decisions.[525]
On 1 June 1994 the Northern Ireland Blood Transfusion Service (Special Agency) was established as a special health and social care agency.[526] Its functions were to ensure that all hospitals and other clinical units in Northern Ireland were provided with adequate supplies of blood and blood products and that those “comply with all current national standards of safety and efficacy”.[527] It was to assess and anticipate the needs for blood and blood products in Northern Ireland, recruit and maintain adequate numbers of healthy, voluntary, non-remunerated donors, ensure the health and safety of donors during contact with the NIBTS, and to provide counselling to those found to have abnormalities during routine screening. It was also to provide “an education and advisory service on the utilisation of blood and blood products by clinicians.”[528] A purpose-built facility opened at the Belfast City Hospital site in 1995. The NIBTS moved there, and it remains their headquarters.[529]
The director of the service between 1969 and 1980 was Colonel Field, followed from June 1980 to May 1994 by Dr Morris McClelland.[530] From June 1994, when NIBTS was created, he became known as the chief executive and medical director. He stepped down in 2009.[531]
Until the early 1980s no plasma was sent from Northern Ireland to the mainland of the UK for fractionation. However, Northern Ireland did receive some blood products manufactured by BPL, as well as purchasing commercial blood products. In the early 1980s it began sending plasma to Scotland for fractionation at PFC.[532]
In 1946, NBTS was formally established in England and Wales. The first blood banking service opened in Wales in 1946 located in Newport Road, Cardiff. During this time, it was under the supervision of the Emergency Medical Service.[533]
In 1948 the Welsh Hospital Board was formed as one of the regional hospital boards established under the National Health Service Act 1946. The board, known up to 1961 as the Welsh [Regional] Hospital Board, was responsible to the Welsh Board of Health. It had oversight of the South Wales RTC, and the Liverpool Regional Hospital Board managed the supplies for North Wales through the Mersey RTC. The Cardiff regional transfusion director initially reported to the Welsh Hospital Board and then, from 1974 when regional health authorities were established in England, to the Welsh Office.[534]
Essentially this arrangement continued until 1991 when the management passed to the Welsh Health Common Services Authority (“WHCSA”).[535] When the National Blood Authority was set up in England, NBTS (Wales) did not become part of it but remained under the control of the Welsh Office; management remained with WHCSA. A new purpose-built building for the South Wales RTC was completed in 1996, and the service moved from Rhydlafar to the new site at Talbot Green, Pontyclun, in 1997 where it remains.[536]
With devolution and the establishment of the Welsh Government, the Welsh Blood Service (“WBS”) was created in 1999, with the director reporting to the Velindre NHS Trust.[537] It was not until 2016 that management responsibility for the blood service in North Wales moved to the WBS. Until then, blood service policies for South and Mid Wales were agreed and funded by the Velindre Trust and the Welsh Government and for North Wales by the NBA and then from 2005 NHSBT.[538]
For most of the time with which the Inquiry is centrally concerned, Dr Tony Napier was director of the RTC in Cardiff. He commented on the disadvantages of the system of regional autonomy (which in practical terms affected South Wales):
“They [the South Glamorgan Health Authority] had their own problems in funding services, but it was always a struggle … If the big issues that we’re concerned with are … to be self-sufficient in terms of England and Wales … then the accountability discussions and the funding discussions should have been taking place centrally with whatever authority was set up to do that … if you were to have a sort of analogy, in World War II times, you would never expect enough Spitfires to be made if the responsibility for doing that was … handed out to different parts of the United Kingdom. It has to be an efficient, centrally managed operation. And the arrangements of accountability being held locally, the sort of accountability discussions didn’t … greatly concentrate on the issues that were important for the service itself: safety, self-sufficiency and suchlike.”[539]
His perspective on BPL, and the ability of the service to deliver self-sufficiency, is also worth recounting:
“Q. … in terms of the obstacles to achieving self-sufficiency, do you have any perspective on the relative significance of, on the one hand, the ability to supply enough plasma and, on the other, the ability of BPL to fractionate? …
A. … I think it could have been run better. I was never completely certain how much the limitations in capacity at BPL played a factor in this. I think we got different signals at different times. Sometimes it appeared that they were our target to support self-sufficiency and at other times we seemed to get messages that there were operational problems which might constrain that.”[540]
The way in which the transfusion services and fractionation plants[541] were organised played a part in the failure of the UK as a whole to achieve the level of safety in blood and blood products it could have done.
Thus the problems of a lack of coordination, highlighted by Dr Napier’s “Spitfire” analogy, and the lack of any one person or body exercising executive authority contributed to the failure of the UK as a whole to achieve the goal of self-sufficiency in blood products to which many had aspired even before Dr Owen made it official government policy. A lack of coordination between England (and Wales and Northern Ireland) and Scotland from the early to mid 1970s onwards added to this.[542] Part of the reasoning which led Dr Lane to persuade others that English plasma should not be sent to Scotland for fractionation, even if it came back to the supplying regions as manufactured blood products, was that the regions had to pay out of their own funding for this. If the services had been operated as initially envisaged in wartime[543] they would have been run and financed to serve the interests of the UK as a whole.
As for NBTS in England and Wales, supplies of plasma for fractionation could not be mandated centrally, and the willingness of regions to use their resources to provide it to BPL was dependent not only on the good will but also the resources available to the region at the time, balanced against other pressing health needs arising locally. The Royal Commission on the National Health Service reported in 1979 that common services such as blood transfusion did not require a regional tier, and pointed to the Common Services Agency in Scotland (with similar arrangements for Wales and Northern Ireland) which provided services to the health boards “without exercising the monitoring role of RHAs in England”.[544]
The separation of a controlling influence over both the transfusion and production parts of the service which occurred when Dr Maycock retired, to be replaced by Drs Lane and Tovey, exacerbated the problems caused by regional autonomy in provision.
The lack of centralised funding led to research being a poor orphan of the service so far as funding and resources were concerned.
As the following chapters will explain, it also contributed to a failure to achieve as much plasmapheresis as would probably have resulted had there been one, national point of executive control, in turn leading to less plasma for fractionation, and a greater waste of blood donations.[545] It similarly made it more difficult to mount an effective coordinated national approach to achieving a greater use of packed red blood cells, and to introduce measures to help minimise the use of transfusions where possible. When it came to a need to pass information on to donors (through such as the donor leaflets produced in response to the HIV epidemic), to screen donors consistently, and to facilitate the screening of donations, a nationally coordinated response would likely have achieved more than was done: it was difficult to achieve it under the system as it stood.
This chapter describes the way in which RTCs were organised, their facilities and funding and their role in the purchase and distribution of blood products. It also describes the components which they produced, their approach to donor recruitment, arrangements for the supply of plasma to BPL and steps taken to obtain more plasma.
February 1972 report by Professor Cash “The Principles of Effective and Safe Transfusion” promotes use of red cell concentrates to help achieve self-sufficiency.
April 1981 “pro rata system” introduced: amount of concentrate returned to an RTC now reflects the amount of plasma provided to BPL by that RTC.
Autumn 1982 SAG-M available to make red cell concentrate easier to administer: reducing demand for whole blood, increasing blood available for plasma fractionation
1982 Belfast RTC starts sending plasma to PFC for fractionation.
April 1989 cross-charging system introduced: RTCs sell plasma to BPL and buy back factor products.
1989 National Provision of Donors Committee established.
Dr Tony Napier medical director, Welsh Regional Blood Transfusion Service
Professor John Cash medical director, SNBTS (1979 - 1997)
Dr Harold Gunson Manchester RTD (1980-1988), Director of National Directorate for the NBTS (1988-1993)
Dr Morris McClelland Northern Ireland RTD (1980-1994)
BPL Blood Products Laboratory
RHA Regional Health Authority
RMO Regional Medical Officer
RTC Regional Transfusion Centre
RTD Regional Transfusion Director
SAG-M mixture of saline, adenine, glucose and mannitol
The main function of the 14 regional transfusion centres (“RTCs”), [546] each of which had its own regional transfusion director, was as summarised in a 1987 NHS management consultancy study:
“RTC Functions
2.13 There is no comprehensive and common definition of what the functions of an RTC are or should be.[547] There is a range of ‘core’ functions common to all centres namely:
2.13.1 collecting blood;
2.13.2 testing the blood collected;[548]
2.13.3 separating blood into components and freezing harvested plasma for transmission to BPL [Blood Products Laboratory] for fractionation;
2.13.4 issuing blood and products to hospitals;[549]
2.13.5 providing a reference service to hospitals on grouping problems;
2.13.6 providing a source of medical advice on transfusion and product related problems.”[550]
Each RTC, as the name suggests, served its own region. Each developed in accordance with (a) the services required by the hospitals they served,[551] and (b) the adequacy of the funding provided by the regional health authority (“RHA”).[552] Many of the RTCs were in old, cramped, inadequate buildings, which curtailed what they could do.[553] Some were inadequately staffed.[554] This meant that only some of the RTCs carried out functions such as cross-matching and blood-grouping, acting as a regional reference centre for the hospitals in the event of transfusion problems[555] and autologous transfusion.[556]
RTCs were funded by, and thus accountable to, their RHAs,[557] with medical and scientific oversight from the regional medical officer (“RMO”),[558] or the regional medical director. The relationship between the RTC and the RHA and RMO varied according to the region. Some RTCs had very little to do with their RHA whereas some had close working relationships. In addition to oversight from their RHAs, RTCs were also subject to inspections from the Medicines Inspectorate. During the 1970s these were informal inspections and in a letter dated 18 May 1981, Dr Diana Walford wrote “the Medicines Inspectors will be starting their formal inspections of Regional Transfusion Centres later this year.”[559]
In Wales, where the South Glamorgan Health Authority was responsible for the Cardiff RTC after 1974, Dr Tony Napier, who was the regional transfusion director, described “reasonably harmonious and efficient arrangements”.[560]
A common arrangement was one where hospitals within the region had their own blood banks, which were supplied by the RTC. This could lead to a disconnect between those using the blood (at the hospital) and those who were concerned with securing future blood supplies (the RTC), which may in part be responsible for what was a sluggish change of practice from the over-enthusiastic use of whole blood for transfusion to both the more general use of concentrated red blood cells and a more sparing approach to giving transfusions.
So far as Wales was concerned, the Welsh Hospital Board was responsible for the Cardiff RTC from 1948 until 1974, when the Board’s functions were assumed by the Secretary of State for Wales who established area health authorities, including the South Glamorgan Health Authority. The regional transfusion director reported to the Welsh Office until 1982 when this passed to the South Glamorgan Health Authority. In his evidence, Dr Napier said “My personal medical accountability was to the Chief Medical Officer … in Wales but, in terms of the operational logistics of the service, it was under the care of South Glamorgan Health Authority.”[561]
There were five RTCs in Scotland.[562] They were part of what became the Scottish National Blood Transfusion Service (“SNBTS”), run by its medical director Professor John Cash from 1979,[563] which had its own headquarters.
One of the main differences between the RTCs in Scotland and the RTCs in England and Wales, was that as well as the functions of an RTC, four out of the five Scottish RTCs (all except the West of Scotland) carried out blood banking for the hospitals in which they were based. This meant that“if a doctor required blood for patients, the request would go to the transfusion service … The transfusion service blood bank laboratory would carry out the compatibility tests to ensure that they provided blood that was matched to that patient’s blood type, et cetera, and they would then, depending on the details of the request, they would either hold it for the patient, or they would send it to the hospital destination where it was to be transfused.”[564]
All five of the RTCs (and the National Headquarters) were centrally funded. Despite this, Professor Cash did not have any power to compel the RTCs to adopt any particular policy and so any decisions that were to be implemented nationally had to be reached by consensus.[565] It follows from this that the Scottish RTCs did not all provide the same services as each other. The RTCs, like their English counterparts, suffered from poor facilities[566] and inadequate staffing which in some instances limited what they could offer.[567]
The Common Services Agency and the health boards took the view that the RTCs were not entitled to claim Crown Immunity, which if they had been would mean they need not be inspected nor would they require licences.[568] Accordingly the Scottish RTCs subjected themselves to formal inspections from the Medicines Inspectors to obtain manufacturing licences. Inspections started in January 1980 and all centres had been inspected by March 1982.[569]
There was only one transfusion centre in Northern Ireland and this was based in Belfast. The Eastern Health and Social Services Board (“EHSSB”) held the budget for it and provided some management support. Thus while the EHSSB was not involved in the day-to-day running of the RTC, if the RTC wanted (for example), to recruit someone, they had to seek authorisation from EHSSB.
The first external inspection of the RTC in Belfast was a 1981 visit by the Protein Fractionation Centre (“PFC”).[570] The first inspection by the Medicines Inspectorate of the RTC was December 1982. Thereafter, inspections took place about every two years.[571]
The granting of a manufacturing licence to the Northern Ireland Blood Transfusion Service (“NIBTS”) was delayed due to the inadequacy of the premises. Indeed, this was a crucial factor in securing the eventual funding for a new NIBTS headquarters unit. The service relocated to the new (current) centre in 1995, and was granted a manufacturing licence once this had been inspected.[572]
Most of the RTCs (prior at least to the introduction of cross-charging)[573] provided plasma to the Blood Products Laboratory (“BPL”) for fractionation, received BPL’s fractionated products back, and then distributed them.[574] Practice as to how they disseminated BPL’s products within their region differed.[575]
Practice also varied widely between RTCs as to whether or not they became involved in the purchase of commercial Factor 8 for the region. Some had no role at all,[576] some performed a warehousing function, ordering what the haemophilia centre directors told them to and then distributing to the relevant haemophilia centres and hospitals,[577] whereas others had a central role in their purchase.[578]
There were differences of practice too as to who paid for the commercial products: in some areas the RHAs funded this directly[579] whereas in others they did so indirectly: the cost came out of an RTC budget.[580]
The system of obtaining and funding the provision of factor concentrates to patients had consequences. In 1989 there was concern at BPL that there was a lack of uptake of 8Y,[581] and that commercial concentrates might be being used instead. This seemed to at least one haemophilia centre director[582] to be a consequence of the awkward arrangements for ordering 8Y (three months ahead, via the RTC) and obtaining it (indirectly, through the RTC, rather than directly to the hospital). Dr Harold Gunson explained that this was because the Blood Transfusion Service held the budget for Factor 8 on behalf of the RHAs.
Prior to the PFC taking over the ordering of products nationally in the late 1980s, the different RTCs had different arrangements for the purchase and supply of commercial concentrates, and the distribution of PFC concentrates.[583]
Despite the fact that from mid 1982 Dr Morris McClelland attended an annual meeting with Dr Elizabeth Mayne to try to coordinate supplies of Factor 8 with usage and demand,[584] it seems that the Belfast RTC had no role in the purchase of commercial product (albeit that from 1985 the cost of the commercial products came out of the RTC’s budget). However, both BPL at first and then PFC thereafter did supply the Factor 8 allocated to Northern Ireland to the Belfast RTC, who would then in turn supply it to Dr Mayne.[585]
Increasing demand by clinicians for blood products[586] throughout the 1970s and most of the 1980s was accompanied by increasing demands for blood components from the blood services throughout the UK. Each RTC in the UK had two central targets to meet: one to satisfy the hospitals in the region each served; the second to cater for the demands of the two fractionators – BPL in England and PFC in Scotland. Its first aim was to collect the donations of blood the RTC needed to meet the demands of the hospitals in its area for whole blood and labile blood components.[587] These products the RTCs prepared and issued themselves. Its second aim was to meet the plasma needs of the fractionators, not just for the production of Factors 8 and 9, but also immunoglobulins, albumin, and other blood products.
In order to achieve these aims, the RTCs had, of course, to ensure that they had sufficient donors.
Blood itself had a short shelf-life even in the presence of an appropriate anticoagulant, and could neither be heated nor frozen. It had to be used, at first within three weeks, later within five or sometimes six. Accordingly, arranging supply was always complicated by the need to provide for a constant flow of donations to meet the anticipated needs for blood to be transfused, from season to season. It is a testament to the abilities of the blood services that they have managed this with as little panic and concern about shortfalls as there has been, though there have been “moments”.
As early as 1964, there were misgivings amongst regional transfusion directors about the ability to recruit sufficient donors necessary for the expansion of the National Blood Transfusion Service (“NBTS”). “Many Directors felt that N.B.T.S. was little known or taken for granted and that national publicity … and appeals by well-known personalities were wanted.”[588] They felt that “Annual recruitment of donors at the rate maintained over recent years was not enough; the rate should increase with the constantly growing demand for blood.”[589]To achieve this, it was decided that “An increasing proportion of donors had now to be recruited from less socially conscious members of the public, and more intensive and costly publicity was necessary in order to reach them.”[590]
At a regional transfusion directors’ meeting in 1965, Dr William d’A Maycock presented a short paper on the future development of regional transfusion centres, the aim of which was to attempt “to reach a better estimate of the blood needed in the next decade.” The information suggested that “in Canada, Australia and U.S.A. the number of donations collected annually was at present proportionally considerably greater than in U.K.”and on that ground it might be expected that the demands for blood would continue to rise: however the graphs presented at the meeting suggested that the amount used per patient had plateaued, and there was concern about being able to use all the blood which one set of estimates suggested.[591]
Despite this early focus on the national picture on donor numbers, until 1994 when the National Blood Authority started a national campaign,[592] campaigns were run at a regional level,[593] it being the responsibility of each centre to decide how best to recruit and keep new donors.[594] In particular, prior to the establishment of the National Directorate in 1988, centralised efforts to develop national advertising materials and strategies paid for from central government funds had limited success. Funding for recruitment campaigns was often an issue.[595]
Donor numbers did, on the whole, increase year on year. The fear of AIDS had some adverse effect on this. There was an initial decrease in the numbers of donors but in November 1985 Dr Gunson felt able to report that this drop had now righted itself.[596] There is nonetheless some evidence that donors continued into the 1990s to link giving blood and getting HIV: the Yorkshire RTC experienced a sharp decline in donor attendance in the late 1980s, and undertook some research which showed that a number of donors felt that by donating they were at risk of being infected with HIV. This led to the RTC mounting a multi media campaign including adverts on buses, at railway stations and in leaflets at doctors’ and dentists’ waiting rooms to reassure potential donors that there was no risk of infection involved in giving blood.[597]
Donor numbers were also affected by the makeup of the donor populations. Some people were reluctant to give blood for cultural and socio-economic reasons.[598]
In February 1989 moves were made to centralise recruitment and retention of donors by forming a National Provision of Donors Committee.[599] It was made up of representatives of RTCs from England and Wales, with observers from the Scottish and Northern Irish blood services. One of its successes was to get the National Directorate to use a national phone number for potential donors to call to make an appointment. This centralised system had a positive impact on the blood supply. At a meeting of the Committee on 10 October 1990, “A comparison with 1989 reveals that stocks are 40% higher and the bleed rate is up by 3%. If this rate is maintained the NBTS will collect 63,000 more donations this year over last year.”[600]
Keeping donors happy and returning to give blood was good not only for retention of donors, but also for their recruitment. It was widely believed that a happy donor would be more likely to become an ambassador for the blood service and thus help generate new donors.[601] Regional transfusion directors described how they had programmes to reward loyal donors with certificates and even gifts.[602]
RTCs produced a range of labile blood components for the hospitals in their area, including whole blood, red cell concentrates and cryoprecipitate. They set their own targets for these products each year in consultation with their haematological colleagues in the hospitals, and the RHA as the funding body.[603]
While the planning for this aspect of an RTC’s work may have been relatively straightforward, the execution of it was not always so. For some RTCs blood shortages were not uncommon. North West Thames RTC was one such centre, despite, according to Professor Dame Marcela Contreras, collecting “more than anybody else per thousand population.”[604] The blood shortages at North West Thames RTC were addressed in part by the RTC contracting with the Oxford RTC to collect donations on its behalf.[605]
Why did some RTCs experience shortages, while others did not? Some RTCs faced issues particular to them.[606] Others suffered shortages due to lack of staff and diminished budgets.[607] Professor Contreras’ explanation for the problems in the North London RTC was that the Centre served a number of London teaching hospitals, who made great demands for blood.[608]
In May 1985, Professor Cash was invited by both North East Thames and North West Thames RTCs to examine the problems that they faced in supplying sufficient blood to hospitals within their regions. In the course of his investigation, he also visited the South West Thames RHA. He reported in March 1986 that there were “very grave problems in maintaining the supply of blood and blood products throughout the London (Home Counties) area” and that “If no collective action is taken then within 3 years the matter will become one of genuine public concern and alarm.” Professor Cash described “acute shortages” occurring every day and clinical requests frequently not being met.[609]
The position he described had “arisen as a result of a long period of neglect with regard to management, primarily at RHA but also at RTC levels”, and he looked for a “plan to reorganise the London Transfusion Services as a whole so that they are … co-ordinated into an operationally cohesive consortium.”[610] He identified that North East Thames RTC (Brentwood) had untapped potential to increase donations; that North West Thames RTC (Edgware) was servicing some London hospitals which ought to have been served by Brentwood; and that it would benefit by an extension of the area from which it collected donations towards Oxford.
A particular problem was that of making provision for private hospitals, which disproportionately featured in London.
It is unsurprising that some RTCs were able to collect more donations than they actually required[611] while some RTCs were unable to collect sufficient donations to meet their needs – unsurprising because the characteristics of the donor population were different in each area,[612] as were the requirements for blood and its components. What is perhaps surprising however, is that there was no national system in place for RTCs who collected more than they required to help out RTCs suffering from acute shortages. Professor Cash, discussing the blood transfusion services in England and Wales as a whole, was extremely critical of a system which made it “possible, and on many occasions, for severe shortages of blood to arise in one part of the country while less than 10 miles away (in another region) the regional health authority is dismantling part of its blood collection programme because of sustained excesses.”[613] This criticism was not accepted at the time by Professor Contreras who accused Professor Cash of “gross exaggeration”.[614]
Without a national system to redistribute donations, there was no pressure on RTCs to exceed their own regional targets in order to assist other RTCs.[615] The need for a national system is highlighted by one remarkable finding made by Professor Cash. He recognised that in Hampstead, Bloomsbury and Islington there were a large number of private (haematological) patients from outside the UK. Because the RTC could on occasion not supply enough blood from its own resources, the private hospitals concerned obtained blood supplies from Europe. He added: “Of no less interest has been the finding that on occasions this European blood has been transferred from the private sector to NHS hospitals that cannot get sufficient supplies from their local RTC. It is my understanding that this latter feature may contravene the Medicines Act.”[616] A failure to organise blood supply on a national basis had in this instance breached an article of faith for blood transfusionists in the UK, by permitting the entry of blood from abroad. Further, reliance would necessarily be placed by the RTC on the private hospitals to satisfy themselves as to the safety of any source from which the blood had been taken, for it seems unlikely that if blood was needed urgently to meet a temporary regional shortfall the NHS hospital using it would carry out those checks.
Once Dr Gunson had been appointed the national director in October 1988, he set up a programme to coordinate the stocks of blood and its components in England and Wales on a daily basis. Each RTC would fax daily stock lists to Dr Moore at the National Directorate, “so that if anybody was short of anything centrally they would know who could bail them out, which was much more efficient than just ringing round, which was what would have gone on before, choosing your nearest neighbour first, of course.”[617]
While this clearly made a difference in plugging short-term crises,[618] arising ad hoc, it was not a strategic approach.
The setting and meeting of targets for the plasma to be sent to BPL for fractionation was altogether more complex.
Unlike the targets for blood and blood components which could be supplied directly from local transfusion centres, they were suggested to RTCs by BPL and the National Directorate, without much input from the regional transfusion directors.[619] As to how the targets were arrived at, the evidence suggests that this changed over time.
The starting position was for BPL to work out the amount of plasma it considered it needed to meet the needs of the populations of England and Wales (and Northern Ireland up until 1982 when they began sending their plasma to PFC in Scotland) for factor concentrates and other fractionated blood products. That overall target was set in consultation with (in particular) the Department of Health and Social Security (“DHSS”) and the haemophilia centre directors.[620] The overall target was then divided between the RTCs on the basis of the size of the population of the area covered by the RTC.[621]
There were three issues with this way of organising plasma collection:
The system was thus one of taking plasma from a region in proportion to its population; but delivering the product back in proportion to the numbers who had been treated in the last year, for which there were records. Yet the system for funding this approach (which was both national, and not obligatory) was regionalised. This meant, for example, that an RHA which funded its RTC to collect large quantities of plasma for supply to BPL, could find itself in effect subsidising areas of the country which did not produce as much plasma.[622] Yet it could not be required to collect as much. It is therefore unsurprising that RHAs were unwilling to meet requests by regional transfusion directors for money to finance ambitious plasma targets.
This was not a system that was conducive to achieving self-sufficiency.[623]
In April 1981 a new system was therefore introduced whereby the amount of concentrate that was returned to an RTC reflected the amount of plasma provided to BPL by that RTC.[624] This was known as the “pro rata system”.
While the pro rata system went some way to addressing the problems identified above, it still had a number of flaws:
A scheme which involved the setting of plasma targets for BPL on a national basis while trying to get regional bodies to fund the necessary work was fundamentally flawed and was ultimately unsuccessful in achieving self-sufficiency.[628] As Dr Gunson noted even the more committed regions would only provide finance for plasma supply in respect of their own population.[629]
In April 1989 a cross-charging system was introduced. This fundamentally changed the way that the RTCs were funded and blood and blood products were paid for. RTCs were now expected to sell their plasma to BPL, and then buy back the product they needed from BPL once it had been fractionated, selling those BPL products on (along with the products the RTCs were producing such as red cell concentrates and cryoprecipitate) to the hospitals in their region.[630] Thus RTCs were no longer fully funded by their RHAs. However, even the introduction of cross charging did not remedy issues in the system that acted as a disincentive for RTCs to increase their plasma offering to BPL. This was because the Department of Health set the cost BPL paid the RTCs for plasma without reference to the actual cost to the RTCs of collecting that plasma.[631] Thus the cost to many RTCs of obtaining the plasma exceeded what BPL would pay for it and RHAs had to subsidise the collection of plasma to be supplied to BPL.[632]
The drive to provide more plasma to BPL led to RTCs changing their practices in two key ways.
First of all RTCs aimed to wean hospitals off their reliance on using whole blood for transfusions where what was needed by a patient was the red blood cells in the donation. If the red blood cells and the plasma in a donation were separated, the plasma component could then be sent to BPL, and the red blood cells used for therapy. If platelets were required for a patient, they could also be separated out, leaving plasma and red blood.
Red cell concentrates were increasingly used; whereas in 1975, 90% of transfusions in England and Wales were of whole blood, and 10% red cell concentrates, by 1985 around 50% of blood issued for transfusion consisted of the red cell component.[633]
Regional transfusion directors had a role in trying to persuade their clinical colleagues to make the switch.[634] Different centres managed to achieve a reduction in the use of whole blood at different times. Scotland was well ahead of England throughout. As for England, the North London (Edgware) RTC was one of those centres which had early success. By contrast, in 1986 Dr Lloyd noted that the Northern area was one of the biggest users of whole blood in the country.[635] Likewise East Anglian RTC was still issuing as much as 40% of the blood it issued as whole blood in 1990.[636]
Secondly, as the chapter on Self-Sufficiency explains, an additive solution called SAG-M[637] was added to blood from (probably) the autumn of 1982 to make red cell concentrate easier to administer and thereby reduce demand for whole blood, increasing the amount of donated blood available to be used as plasma for fractionation. However, the introduction of SAG-M was initially slowed because it was regionally and not nationally funded. It appears that some RHAs were reluctant to finance the additional up-front costs.[638] A report from January 1984 stated that there had been difficulties in obtaining funds from RHAs in the latter part of 1983 and several regional transfusion directors had cancelled orders of SAG-M packs.[639]
Thirdly, RTCs had to consider whether to obtain plasma by way of plasmapheresis. Again, this is addressed in the chapter on Self-Sufficiency. All the RTCs had some form of plasmapheresis programme by the end of the 1980s or beginning of the 1990s, save for the North East Thames RTC.[640]
Self-defeatingly, the South West RTC in 1975 increased its plasma offering to BPL by getting agreement from treating haematologists in its region to restrict the amount of cryoprecipitate (produced from locally sourced plasma) being infused in favour of the use of Hemofil.[641]
There were a number of barriers to RTCs reaching their plasma targets, quite apart from the systemic problems set out above. For example, the Yorkshire RTC failed to meet its targets in 1989 because of an industrial dispute, an increased use of cryoprecipitate and fresh frozen plasma locally, and the loss of 10,000 donations.[642] This resulted in their target being revised down the following year.[643]
Dr Lloyd in his written and oral evidence identified three barriers to the Northern RTC meeting its plasma targets. First (and prior to 1985 when a new centre opened), was the limited and outdated nature of the facilities at the RTC. Second was the belief of those at the RTC that the hospitals needed whole blood, rather than red cells (and in any event they did not have the bags and the funds to use SAG-M which would have increased the plasma they could have collected in this way). The third was “prior to 1988 the RHA’s approach to funding plasma collection.”[644] In a document he produced in 1989 he mooted some different reasons for this third barrier:
Blood shortages were not unknown in Northern Ireland. There were occasions when supplies to hospitals had to be rationed or elective surgery had to be postponed.[647] Certainly in the late 1970s and early 1980s the closure of many factories made it more challenging to meet targets[648] since factory donation sessions were relatively easy to organise and generally very well attended by would-be donors.
The Northern Ireland RTC used telemarketing, which involved eligible donors being telephoned immediately prior to donor sessions.[649] As in England and Wales, media advertising in newspapers, on radio and on television was used to try to encourage more donors.
As to plasmapheresis, in the 1970s there was occasional collection by manual plasmapheresis for the collection of special reagents when donors or antenatal patients were identified as having a particularly valuable antibody. Later, collections were made by machine pheresis, and by 1990 NIBTS was collecting over 3000 plasma donations per annum in this way. This was the maximum throughput that could have been achieved in the (old) NIBTS building and represented about 10% of the total amount of fresh frozen plasma which was sent to PFC in Scotland.[650]
The Belfast RTC was one of the earlier centres to adopt SAG-M. By 1986 it had increased its output of red cell concentrates from something like 20% of the units sent out for transfusion, to 75-80%, in the space of about three or four years.[651]
Prior to 1982, the Northern Ireland RTC sent its plasma to BPL for fractionation. Due to difficulties shipping fresh or frozen plasma it was able to send only liquid plasma which was “time expired” - that is, had deteriorated over time such that (for instance) the Factor 8 activity in it had ceased. Liquid time expired plasma therefore could not be used to make Factor 8 concentrates.[652] Yet the haemophilia centre needed to provide treatment to its patients and before the pro rata system received a small amount of Factor 8 from BPL, probably in the region of about 200,000 units per year.[653]
Following the introduction of the pro rata system and from the end of 1982, all Northern Irish plasma was sent to PFC in Edinburgh.[654] Arrangements were made to transport it in a frozen state, so that it did not denature. There was however a slight delay in making the arrangements for this since the testing regime to which Northern Irish plasma had been subject was not identical to that adopted in Scottish centres, and there was concern about mixing Northern Irish and Scottish sourced plasma in the same pools.
Dr Morris McClelland told the Inquiry that “Education of clinical users of blood/ red cells and persuasion towards the use of red cell concentrates instead of whole blood was a key part of the strategy towards achieving self-sufficiency.” The rapid uptake of red cell concentrates from 20% of the Belfast output to 75-80% in the space of three to four years, was in his view, testament to the success of their work.[655]
Voluntary organisers from the local community helped to recruit donors. This approach was described by Professor Stanislaw Urbaniak as being “highly successful in maintaining a ‘repeat donor’ base of regular donors”.[656] Dr Brian McClelland described the role of volunteers being phased out in the 1980s in South East Scotland and an increasing role for radio and television advertising.[657] Dr Jack Gillon, the consultant in charge of the donor programme working with Dr McClelland, said this was effective at reversing dips in donor attendances in the 1980s and 1990s.[658]
There does not appear to have been an initial drop off in donors during the years that AIDS leaflets were first being provided to donors. On the contrary, attendances and donations increased up to 1985 in South East Scotland.[659] There was however a sharp drop off in donor numbers between around 1985 and 1987, which Dr McClelland and Dr Gillon attributed to the effects of AIDS messaging.[660] The position was sufficiently concerning that Professor Cash estimated that if the trend continued “sometime in mid 1988 the demand for products will exceed plasma supply.”[661]In response to this, a national media campaign to promote blood donation was agreed and at a meeting in April 1988, Professor Cash confirmed that donor attendances had increased in the first quarter of 1988.[662] He was able to report at the end of 1988-89 that “we now have some reason to believe that the decline [of the preceding 18 months] has been checked and certainly in some parts of Scotland it appears to have been reversed.” Professor Cash went on to say: “We cannot be content to rest on our laurels for we believe we need to increase our blood collection programme by a further 40,000 donations per annum to meet the many and varied needs of patients in the 1990s … the effort required to stand still seems to be greater than it was in the 1960s and 1970s.”[663]
As part of this initiative, Dr Cash secured the appointment of a national donor programme manager in Scotland.[664]
The Scottish transfusion centres did not seem to suffer difficulties of supply in the way described in England and Northern Ireland. In fact, the South East Scotland Transfusion Centre in Edinburgh, would sometimes send their surplus red cells to an English RTC to address their shortages.[665] Professor Urbaniak said that where North East Scotland could contribute “over and above” national targets based on population, they received “the funding required to facilitate this.”[666]
It was a national objective for Scotland to be self-sufficient in plasma products.[667] It was generally successful in this, as set out in the chapter on Self-Sufficiency.
A national target for plasma collection for Factor 8 was arrived at by the Scottish haemophilia directors estimating the number of international units of Factor 8 that would be required. This was then converted by the SNBTS into the weight of plasma in kilograms required to meet this, assuming a yield of approximately 200 international units of Factor 8 per kilogram. That target was then shared out between the five Scottish transfusion centres on the basis of population with some adjustments made for historical production.[668]
Dr McClelland’s recollection is that the SE Scotland RTC was hitting its targets fairly regularly and that generally, all the centres met theirs, save for the Glasgow/West of Scotland RTC which sometimes struggled.[669]
SNBTS took steps to maximise the use of blood components similar to those described above for England and Wales: encouraging the use of red cell concentrates over whole blood, using SAG-M, and adopting plasmapheresis. In 1974 the DHSS understood that 30-40% of donations in Scotland were issued as red cell concentrates, compared to less than 10% in England and Wales. By 1976, 46% of donations in Scotland were issued as red cell concentrates and by 1982, 60% of donations were being processed into red cell concentrates with 220ml plasma removed.[670]
From early on, Professor Cash considered that encouraging the use of red cell concentrates was an important part of the strategy to achieve self-sufficiency. In February 1972, he published a report entitled “The Principles of Effective and Safe Transfusion”, in which he urged clinicians to use red cell concentrates whenever patients did not require whole blood. He argued that the practice of giving whole blood had led to the wastage of several thousand litres of plasma and billions of platelets, and the alternative of using red cell concentrates was simpler and safer. In his opinion, the practice of using whole blood had become entrenched because SNBTS had, up to this point, seen no reason to conserve plasma and so had not made red cell concentrates available. This was not helped by the isolation of Scottish RTCs “from the bedside”, which meant it was difficult effectively to encourage the use of red cell concentrates. Professor Cash argued that clinicians and SNBTS ought to see routine whole blood transfusion as a “thoughtless habit”, and should not shy away from the realities of efficiency, which involved the optimal use of raw material.[671] In August 1980 he wrote to The British Medical Journal with a letter headed “Factor VIII supply and demand” criticising doctors who treated patients with whole blood rather than red cell concentrates, which he claimed resulted in thousands of litres of fresh plasma a year being diverted away from producing Factor 8 in the UK.[672]
The evidence on plasmapheresis is mixed. Professor Urbaniak said that with the drive for self-sufficiency in Factor 8, the target for North East Scotland was “to produce as much as we could, within logistical and financial constraints. This we did, producing more plasma per head of population than other Scottish centres, because of our stable donor population.”[673] Dr McClelland’s evidence was South East Scotland initially had three plasmapheresis beds in the early 1980s for the collection of plasma from donors who had high levels of antibody either to tetanus toxin or to the rhesus antigen to make specific immunoglobulin products, but then started a small automatic plasmapheresis programme. He would have been “keen” to expand it and submitted business plans but there was no enthusiasm at SNBTS or the Scottish Home and Health Department to pursue it.[674]
This chapter has described a system of collecting whole blood or plasma from voluntary donors and then dealing with it in two different ways. Blood went for transfusion or local production of cryoprecipitate or fresh frozen plasma for therapy in response to regional needs. Plasma, either obtained from whole blood, or as plasma following plasmapheresis, went in England and Wales to BPL, and in Scotland to PFC in Edinburgh, in response to national needs.
In fulfilling these tasks, the RTCs were custodians of a valuable natural resource (blood and plasma). As part of the careful husbandry of blood which this necessitated, they had a role in educating or persuading clinicians using blood for transfusion to do so less often, and when doing so to use it in lesser quantities.
The fact that the system was regionally funded and regionally controlled in England and Wales led to problems, and tensions within the service. So far as blood was concerned, there was a tension between the supply of it, and the clinicians’ demand for it. This rarely caused problems on its own, but when demand for plasma for fractionation rose, this demand, together with those of the clinicians, had to be balanced against the available supply.
The system was inefficient when it used whole blood for transfusion where only red blood cells were required, wasting the plasma, and also when whole blood was used as the source of plasma for fractionation or cryoprecipitate, wasting the red blood cell component. This chapter has also described how efforts were made to persuade clinicians to change their prescribing habits, and to adopt the use of SAG-M to enable the red blood cell component to be more easily used. Education and persuasion were ultimately reasonably successful. But this success could and should have been achieved more quickly than it was. Delay in this had an effect on the health of people with bleeding disorders. It meant that self-sufficiency was more difficult to achieve and more were likely to be put at risk.
Nonetheless there was general success in matching supply with demand so far as blood for transfusion was concerned. The UK was almost entirely self-sufficient in its supply for blood for this purpose. There almost never needed to be any reliance on imported blood, as such.[675] This is in many ways a remarkable achievement, especially in days when “just-in-time” manufacturing and distribution was a thing of the future: for blood is a short life product, which had to be obtained from willing donors in sufficient quantity to meet what would inevitably be a fluctuating demand. In any part of the country, emergencies might arise which would impose a strain upon the regional resource. It could however have been improved if a more systematic way of meeting a shortfall in one region could be met by providing blood from a region in surplus. This only proved possible when the National Directorate began in the late 1980s.[676]
This chapter has shown that some of the tensions would have been eased, and quicker progress towards self-sufficiency would have been achieved, if NBTS had been organised on a national basis, centrally funded.
This is not simply a decision of hindsight. The inadequacies of a system of regional autonomy beyond the late 1960s were memorably described within the DHSS by Thomas Dutton in 1976 in part of a report where he said “As long as the collection, testing and despatch of whole blood was the predominant occupation of blood transfusion centres they were able to function as independent regional units which were largely self-sufficient except in times of emergency. The adequacy of independent self-sufficient regional units was however greatly reduced with the introduction of component therapy on a large scale.”[677]
It took too long to remedy this. Responsibility is shared between those responsible for setting up the system as it was, and those who resisted repeated calls for change (successive governments), and by many in the medical profession who insisted on using whole blood when it was unnecessary (and wasteful) to do so.
Finally, although interventions by a Chief Medical Officer should be limited in number if they are to be at their most effective, there is a powerful case here that the Chief Medical Officer should have made it clear that, unless there were good reasons not to do so in a particular case, the red blood cell component should be used in transfusions rather than whole blood. This would probably have had the effect of accelerating the change of prescribing habits which was desirable.
This chapter considers the blood services’ knowledge of viral risks and their response to those risks over time. It discusses in particular donor selection and donor screening, the organisation of donor sessions, the role of the blood services in educating clinicians about the responsible use of blood and the production of AIDS donor leaflets.
1946 first guidance on donor screening Medical Examination and Care of Donors.
1952 WHO Expert Committee on Hepatitis recommends preventative measures to reduce the risks of serum hepatitis.
September 1973 RTDs discuss the continued collection of blood from prisoners.
May 1975 CMO advises that collection of blood from prisoners can continue.
1976 ISBT advises against collecting blood from prisoners and from donors with history of viral hepatitis at any time.
November 1976 DHSS circular allows those with history of hepatitis or jaundice to donate provided no symptoms in last 12 months and a negative HBsAg test.
February 1983 DHSS issues circular on record keeping and stock control arrangements.
May 1983 first substantive discussions on AIDS at RTDs’ meeting and at SNBTS meeting.
1 September 1983 first AIDS donor leaflet available for distribution.
March 1984 Collection of blood from prisoners in Scotland ceases; end of 1984 collection of blood from prisons in England and Wales ends.
February 1985 second AIDS donor leaflet available for distribution.
Professor John Cash medical director, SNBTS (1979 - 1997)
Dr Marcela Contreras medical director, North London Blood Transfusion Centre
(1984 - 1995) and executive director London and South East Zone, NBA (1995 - 1999)
Dr Harold Gunson director, NBTS (1988 - 1993)
Dr Patricia Hewitt lead consultant for Transfusion Microbiology, London and South East Zone (1995 - 2000) and national lead consultant, NBA (later NHSBT) (2000 - 2005)
Dr Brian McClelland Edinburgh & South East Scotland RTD (1979 - 2001)
Dr Morris McClelland Northern Ireland RTD (1980 - 1994)
Dr Tony Napier medical director, Welsh Regional Blood Transfusion Service (1977 - 1998)
Dr William Wagstaff Sheffield RTD (1974 - 1994)
BPL Blood Products Laboratory
CMO Chief Medical Officer
ISBT International Society of Blood Transfusion
NBA National Blood Authority
NBTS National Blood Transfusion Service
RTC Regional Transfusion Centre
RTD Regional Transfusion Director
SNBTS Scottish National Blood Transfusion Service
The risks that blood transfusion or use of factor concentrates could lead to serum hepatitis (or as it became known in the late 1960s Hepatitis B, and in the early to mid 1970s non-A non-B Hepatitis (“NANBH”)) were known before the Second World War, and became indisputable during it.
What the preceding chapters have shown is that the risk that blood transfusion or use of factor concentrates could cause AIDS was known in mid 1982, and became increasingly apparent as a serious risk until it came to be regarded as a near certainty in April 1984, after a press conference in the US at which it was announced that Robert Gallo had discovered a virus which was the cause of AIDS. [678]
Yet although it was strongly suspected before April 1984 that AIDS had a viral cause, the microbiological configurations of both HTLV-3/HIV and also NANBH/Hepatitis C (as they turned out to be) were unknown.
How best could such a risk have been reduced, or even avoided, when no one could either test definitively for the disease (they had, rather, to wait for symptoms to emerge) or screen what was being transfused to eliminate it (because there was no definitive test)?
The answer to this vital question is addressed in this chapter.
The first comment to be made is that the difficulties can be overstated. The problem is not a new one. For centuries, humanity has struggled with strange disease and found ways of warding it off. It has done so without needing precisely to understand how precisely it was caused. Knowledge is elusive: there is almost always more of it we do not yet know. What is important in ensuring public health is having enough knowledge to understand that there is a risk (and therefore to begin to search for ways which prove effective in warding it off) rather than to have certainty of the precise cause and effect. An effective public health system does not demand certainty before responding: though more knowledge may hone the response, it must not shrug and say “it’s not quite clear what’s happening here. It looks as if X causes Y, but we can’t be sure; and we’re certainly not sure how it can”, for such defeatism leads, as the word itself signals, to defeat. Thus, in the past we have been successful in recognising that something in the water supply caused cholera; that exposing people to cowpox protects against smallpox; that pasteurisation destroys the prospect of milk transmitting tuberculosis; that taking measures against insects will halt the diseases they carry – and so on.
In short, a lack of knowledge about the exact nature of the infective agent was no barrier to steps that could be taken to reduce the risks of the infection being caused.
The risk of contracting AIDS or hepatitis, whether by transfusion in the course of surgery or treatment for illness, or because of treatment with blood products, could be avoided if the transfusion or treatment simply did not take place at all. That is important to remember, given that single transfusions of blood carried a risk that the recipient might contract these diseases as a result, and there is considerable material to show that blood transfusions were often given unnecessarily and/or too many units of blood were given at any one time.
Otherwise, some element of risk almost certainly remained.[679] However, though a risk might not be eradicated completely, the risks which had been apparent since 1939 when the transfusion services were first set up[680] could be reduced.
How? An answer which has stood the tests of time was given by an Expert Committee on Hepatitis of the World Health Organization (“WHO”) in 1952.[681] In their report, the committee of experts dealt with the prevention of the spread of serum hepatitis “by Human Blood and its Products”.[682] After the general comment that national health authorities should alert the medical profession in their countries “to the dangers of transmitting hepatitis by transfusion of plasma and whole blood, and also by the use of certain blood derivatives, and should advise that plasma, particularly large-pool plasma, should not be used unless the advantages likely to be gained by its transfusion outweigh the risk of transmitting the disease”[683] it went on to identify the “preventive measures” that might be taken.[684] These were:
The Expert Committee’s report, and the measures it identified, acts as a blueprint for what follows.
A general measure which would help to ensure that the blood given to a recipient was as free of infection as could be expected was to ensure that it was given by people who had no incentive in making the donation other than to do good to a fellow human being (the “voluntary non-remunerated donor” principle). It was a true donation. By contrast, in many other countries blood and plasma were purchased from the “donor”. This was not in truth a donation, though it has been called that: it was a sale.[690] The motive in selling it was to make money, rather than to do good.
The blood services in the UK adopted the voluntary non-remunerated donor principle. Though some participants have reported that they were told by hospital staff that they had received “American blood”, the Inquiry has found no evidence to confirm that this was the case (except on one occasion, footnoted below).[691] If it had been, there would have been at least some records. There would have been some recorded or remembered need for it to have been imported.[692] There is neither, since the blood transfusion service was able to satisfy all the transfusion needs for whole blood or packed red blood cells (save in the case, very occasionally, of an exceptionally rare blood group, which was then sourced from elsewhere) – that is, with the exception of plasma. “Self-sufficiency” as a concept has sometimes been understood to apply to “blood and” blood products. In the context of this Report it refers to blood products alone.
So important was the voluntary non-remunerated donor principle that even when universal screening of blood for the presence of the Hepatitis B antigen was introduced, the prestigious US physician Dr Harvey Alter said that nonetheless “By far, the single most significant measure for the reduction of posttransfusion hepatitis is the total exclusion of the commercial donor.”[693]
Beyond that, in line with what the Expert Committee assembled by the WHO had identified in 1952, the lines of defence the UK had against hepatitis (and later, HIV) viruses, before universal screening for all of these viruses was not only available but effective, were as outlined below. Since they were the only tools available, it was incumbent on the blood services to apply them with rigour.
Even though reliance on voluntary donations was of huge importance, the risks could be reduced further. Careful recruitment of voluntary blood donors (“donor selection”) reduced those risks that were greater in some groups than others. This involved excluding people not because they were themselves individually shown to be a higher risk, but because they belonged to a group identified as giving rise to one, or were placed in a situation which experience suggested was liable to generate more risk. This is, in effect, a process which excludes donors on a “group” or “collective” basis.
At an individual, rather than at a group level, “donor screening” could be conducted. It differs from “donor selection” because it focuses on the individual who comes to make a donation, rather than the person not so much as an individual but more as a member of a group. Would-be donors could have been asked questions to exclude those whose recent medical or social history suggested that they might pose a particular risk. For instance, those who had recently suffered a bout of hepatitis, who were currently running a temperature, had a persistent medical condition which might indicate a disease, who had raised glands, or who had recently returned from a place where diseases such as malaria or dengue fever were rife.
It was possible, too, for “donor (or donation) testing” to occur – a donor could have their blood screened to see if it carried any virus or parasite which could be identified, though, generally, testing the individual donation after it had been given, rather than the donor beforehand, was the preferred course.
Where there was no test specific to a particular virus, because it had not yet been identified sufficiently to enable a test to be formulated, it could be possible to test for another virus or blood marker which appeared to be linked to the virus of interest. This (“surrogate testing”) would indicate a real risk (though not the probability) of infection, or at least that the donor or their donation was of a “higher risk”. The link might exist because it was indicative of a certain lifestyle: for instance, it might be thought that some people whose medical history was typical of many who have lived a “skid row” existence, whose blood test suggested they had been in contact with Hepatitis B, might be more likely than others to have come into contact with NANBH or the virus (if it was one[694]) which caused AIDS; the same could be true also of those whose liver function tests showed elevated levels of alanine transaminase (“ALT”) or aspartate transaminase (“AST”).[695]
The steps mentioned could be performed irrespective of whether the purpose of taking the blood donation was to transfuse it as whole blood, or to separate the red blood cells and platelets from the plasma, and use the latter to make a blood product. The protective measures already mentioned would apply to both. However, further steps (such as physically heating donations of blood components or chemically treating them) almost entirely relate to blood products, for they involve taking steps which will damage red cells, platelets or whole blood intended for transfusion. Red blood cells, and therefore “whole blood”, cannot be heated, for to do so destroys the red cells. Platelets too are susceptible to heat. It is not generally possible to treat red blood cells or whole blood, as opposed to plasma, with a chemical, or solvent detergent, which might inactivate a virus. Another theoretical possibility – irradiation – was shown in the early 1950s to have no effect in inactivating serum hepatitis. The viral inactivation of blood products is the subject of the chapter on Viral Inactivation.
The fourth measure emphasised by WHO in 1952 was keeping records, and reporting. A report from a donor that they had suffered jaundice, or begun to show signs which might be indicative of AIDS, could only lead to the withdrawal of their donation from the system if records had been carefully kept (records) and reporting of any symptoms arising after donation had been encouraged (reporting): but it would also require that the blood donation or any pool of plasma to which it had contributed had not as yet been distributed for use. This leads to the question of whether, and to what extent, blood might be quarantined.
Assuming reasonably careful donor selection, donor screening and donation screening (and any surrogate test if that is adopted as a system) it is possible to quarantine blood or blood products, and simply not issue blood which has been bagged ready for transfusion. If it has been issued already to a transfusion centre, ready for use, it may be recalled. These actions can follow if information reaches the transfusion centre that a donor may have given blood during a period when the donor has been incubating a virus, although displaying no symptoms of this at the time of the donation. For this reason, whole blood is not generally issued immediately for use.
Quarantine is not a wholly satisfactory solution to the problem of late-materialising infections. It can last no longer than the shelf-life of donated whole blood. Throughout most of the period with which the Inquiry is concerned, this was 21 days. That has now been extended to 35 days with the use of more advanced coagulant treatment. In contrast, plasma (included in the plasma portion of “time-expired” whole blood[696]) lasts for several months and if freshly frozen, up to three years. Ideally, both are better used fresh – like any natural product their quality gradually declines over the period within which they may safely be used.
Product recall relates principally to blood products made from plasma: the tracing of donors to ensure that they remain free of disease and have not contributed to a batch during an infective incubation period is more practicable than if the donation was to be used as whole blood. Recall will apply in particular to as yet unused batches of products or the batches which have been shown or are suspected to be infected.
At the start of the 1970s, a major challenge was that of hepatitis being transmitted by blood. As long before as 1952, the Expert Committee on Hepatitis of the WHO had, as set out above, identified, amongst measures to be taken to combat the risk of a transfusion leading to liver disease, the need to select donors. The Inquiry heard in evidence that Dr David Dane (who discovered the “Dane particle” which allowed Hepatitis B to be identified and screening tests developed) repeatedly drilled into his students that they should “know [their] donors”:[697]
“you must know your donor, you can’t know anything about … things which shouldn’t be in the blood … unless you know something about the donor: who they are, what they do, where they do it, how often they do it, who they do whatever it is with whoever they’re doing it … unless you know your donor you won’t know what transmission of agents they are at risk from … If you don’t know your donor, you’re relying entirely on testing.”[698]
The process of selecting a donor involves choosing whom to approach to give blood, screening those who answer the call. This chapter examines the approaches of the blood services to these two processes, and whether they effectively reduced risk as far as they reasonably could and should have done.
The context was the overall requirement for donations to be made in sufficient quantity to meet clinical need. According to a publication for the WHO an estimate frequently quoted was: “in countries with fully operational public health and blood transfusion services, the need for blood can be met if about 2% of the population are regular blood donors.” However, the development of open heart surgery, renal dialysis and other procedures requiring transfusion meant that by 1971 it was considered probable that this figure was too low.[699]
The considerable advantages of the voluntary, non-remunerated donor are set out earlier in this chapter. Reliance was typically placed on these advantages in inviting members of the public generally to come forward to give their blood freely.
Some may wonder why the words “voluntary” and “non-remunerated” appear together in the usual description of UK donors, and in the advice of the WHO; they may think that surely they express the same idea. That is not entirely true.
In one sense it can be said that where soldiers were lined up at a barracks to donate blood, for no financial reward, their donations were voluntary: but one only has to picture a regimental sergeant major (“RSM”) ordering the process to see that it may not truly be voluntary, since if (for instance) the soldier concerned, being a male, had engaged in sex with another man it would be improbable he would admit it with all the adverse consequences that doing so would probably bring for him; and he would be unlikely to defy an order of the RSM to give the donation.
Other pressures might similarly mean that a would-be donor could not easily refuse to donate without the refusal causing personal difficulty or embarrassment. The prisoner may be subject to the pressures in a penal institution to give blood to order, rather than by their own unfettered will; the worker in a large factory may find it awkward to refuse to donate, or, if interviewed by the person in charge of the donor session, to give them reason to think that their blood may be a higher risk to an end user than that of co-workers. Explaining why they did not on that occasion give blood, when it would be clear to the other workers coming forward that they had not, could create problems for their future relationships at work. Regional transfusion centres (“RTCs”) needed to be alert to the possibility of pressures such as these.
Quite apart from the possibility of such pressures resulting in some donations being accepted which would not have been had the position of the donor been fully appreciated by those taking their blood, some groups who posed a higher risk to eventual recipients were not only accepted but targeted to provide donations.
Prisons were regarded as a valuable source of blood donations from the 1950s until the 1970s. A 1971 publication described prisons as one of the institutions from which initial steps to form a panel of donors could best be taken, along with the armed forces, the police, large industrial or commercial undertakings, universities and social or religious foundations.[700] However, following the introduction of the screening of donors for Hepatitis B in the UK from late 1970, it became clear that there was a markedly higher incidence of Hepatitis B amongst prisoners than there was in the general population.[701] Indeed, in the US the American Red Cross stopped collecting blood from prisons on 1 July 1971 because the incidence of hepatitis was ten times greater among prisoners than among voluntary unpaid donors.[702]
Despite the knowledge of some of the regional transfusion directors (“RTDs”) about the higher incidence of hepatitis amongst prisoners, all RTCs still collected donations from prisons, borstals or equivalent institutions in October 1971.[703]
On 26 September 1973 National Blood Transfusion Service (“NBTS”) directors discussed whether they should stop collecting blood from prisons in England and Wales. Seven directors (Sheffield,[704] Edgware,[705] Brentwood, Cambridge,[706] Tooting,[707] Cardiff[708] and Birmingham[709]) voted to stop prison sessions and seven voted to continue (Newcastle, Leeds, Oxford, Bristol, Manchester, Liverpool and Wessex) on the grounds that Hepatitis B screening gave “adequate protection”[710] and the statistical significance of the data suggesting a higher incidence among prisoners compared to new donors from the general public should be examined.[711] The meeting agreed that if it were decided to discontinue bleeding prisoners, the Department of Health and Social Security (“DHSS”) should inform the Home Office before any local action was taken.
Following further research by the Advisory Group on Testing for the Presence of Hepatitis B Surface Antigen (“The Maycock Group”) on the continued collection of blood from donors in prisons, Dr Henry Yellowlees, Chief Medical Officer (“CMO”) wrote to all regional medical officers in England on 1 May 1975:
“There is a relatively high risk of hepatitis B being transmitted by the blood of prisoners. But there is probably an equally high risk in other groups of the population, eg drug addicts, who are not so easily identified in advance as prisoners, if they can be identified at all. The advice we have received is that it is not necessary to discontinue the collection of blood at prisons and similar institutions provided all donations are subjected to one of the more sensitive tests.”[712]
By way of comment, the idea that because there is a risk from one source, you may ignore the fact that there is a risk from a second source, makes no sense at all if the object is to avoid all risk as far as reasonably possible. The logic was clearly faulty. The object should have been to eliminate both risks as far as that could reasonably be done – and the first step in achieving that would be to cease seeking donations from prisons. The advice that it was unnecessary to discontinue donations looked at the wrong question: it should have been whether it was safer to do so. And the reason that it was “not necessary” was based on the efficacy of the latest tests for Hepatitis B. Not only did this entirely miss the possibility of NANBH which by now was known, and also missed “window period” infections, but it also assumed a reliability in detecting infective units of blood which the tests at this stage simply did not have. In short, the CMO missed an important opportunity to ensure that safety was the primary consideration and instead permitted – indeed, it could be said, encouraged – the continuation of a dangerous practice.
His letter left the question of continuing to take blood from prisons up to the transfusion directors. They had been split on the issue in 1973, partly on uncertainty about the reliability of the statistics. That uncertainty could no longer be a reason given the opening sentence of Dr Yellowlees’ letter, for he appears there to accept that he is satisfied that the risk is “relatively high”.[713] The tide of evidence, and sense of proper practice, was turning against the continuation of prison sessions. Though some transfusion directors acted reasonably quickly to stop such sessions, others did not.
I note that the Scottish National Blood Transfusion Service (“SNBTS”) in their closing submissions considered that there was probably an overreliance on Hepatitis B surface antigen (“HBsAg”) testing to provide safety for donations from prisons, due to an underappreciation of the concept of the window period and of the risk of transmission and severity of NANBH. As is clear from what is said above, I agree: my comments which go further, about the CMO, are of course in respect of the CMO in England, about whose particular actions I would not expect SNBTS to express an opinion.
Returning to the factual narrative: in 1976 the International Society of Blood Transfusion published guidance advising against collecting blood from prisoners,[714] and in 1981 a further study was carried out which demonstrated that in the west of Scotland HBsAg positive donations in the male prison donor population were almost five times higher compared with the general male donor population.[715]
It was not simply the high incidence of hepatitis that made prisoners unsuitable as blood donors. There were real concerns that they may not always be true volunteers, and that the environment in which they were donating was not conducive to them telling the truth about any risk factors they might have (such as being an intravenous drug abuser or having a viral infection).
Despite this, as late as the early 1980s, it was still Home Office policy to encourage prisoners to become donors as it was believed to help with their rehabilitation.[716]
A survey conducted by Dr Ewa Brookes of the East of Scotland Blood Transfusion Service on 13 September 1983 showed that Wessex, Bristol, Cardiff, Liverpool, and Leeds were still conducting donor sessions within prisons and that Oxford, Newcastle and Birmingham had only stopped that year.[717]
When understanding developed in the UK that HIV was transmitted by blood, that there was a relationship between hepatitis carrier status and AIDS, and that there was an “extremely high incidence of hepatitis carrier status” amongst the prison population, continued donations from prisons could be seen as fraught with risk. The realisation of a growing epidemic of AIDS signalled the beginning of the end for prison sessions for those RTCs still holding sessions in corrective institutions.[718]
The collection of blood finally stopped from closed prisons and borstals in England and Wales at the end of 1984 and from the last open prison in 1986.[719]
By way of comment, the predominant consideration in acquiring and supplying blood for transfusion should have been safety – of the blood, principally, for those who would receive it as a transfusion, or test or handle it in its journey from vein to vein, as well as the safety of the donor. Between it becoming clear to transfusion directors in late 1973 that there was probably a higher risk of hepatitis amongst prisoners,[720] as it was to at least seven of the fourteen directors at that meeting, and confirmation of the reality of that higher risk by the opening sentence of the CMO’s observations in his letter of 1 May 1975, they should have begun to phase out prison sessions. They were inhibited in part from doing so by the attitude of the Home Office (then the government department responsible for prisons) seeking to advance the rehabilitation of prisoners. However, between taking a step which would improve the safety of donated blood and minimise damage to the public health, on the one hand, and taking a step which might help contribute to the rehabilitation of a prisoner (only in a very few cases likely to contribute to public health) on the other, there should have been little contest. Blood safety and public health should have been predominant. I do not blame the Home Office for advancing its own cause: but the blood services should have resisted earlier and more effectively than they did, for they had the better case. Prison donations continued for much too long.
In Scotland, blood was collected from prisons between 1957 and March 1984.[721]
Similar debates occurred about whether prison collections should be stopped because of the increased risk of hepatitis. The decision, as in England and Wales, appears to have been left up to the individual transfusion directors.
Views as to the social utility of collecting blood from prisoners were also held in Scotland. For example Dr John Wallace, director of the Glasgow and West of Scotland Transfusion Centre, wrote in 1977 in the textbook Blood Transfusion for Clinicians that as “the incidence of HBs antigenaemia among male prisoners in Scotland is less than 1 per cent using the most sensitive techniques of testing … it is socially and psychologically undesirable to exclude prisoners … acceptance of prisoners helps to rehabilitate, and some of these volunteers become regular donors after release.”[722]
On 29 March 1983 Dr (later Professor) John Cash reported that the Medicines Inspectorate had commented adversely on the practice of collecting blood in prisons and borstal institutions, and he invited directors to comment on the practices in each region and to give their view on the Medicine Inspectorate’s criticism. It was reported by the directors present that sessions were held in penal institutions in all regions, although Dr Brookes and Dr Stanislaw Urbaniak intended to review the situation in their regions. The directors were unable to agree on future policy at that meeting.[723]
By December 1983, Dr Brookes told the SNBTS directors meeting that “the only Scottish region to continue holding sessions” was now Glasgow,[724] which held its final session on 25 March 1984.[725]
I have already noted the views of the SNBTS expressed in final submissions, and accept them. I would add only that the risks of NANBH were, for similar reasons, likely to be higher in penal institutions, and to take donations from them risked not only Hepatitis B, known to be present at higher rates, but those risks too and (as should have been appreciated after the start of 1983) implied a greater risk of the putative virus which caused AIDS as well.
In Northern Ireland, prison sessions took place across the country and the last session occurred in Belfast on 26 October 1983.[726] In his evidence to the Inquiry Dr Morris McClelland was asked: “Looking back now, and having regard not only to the fact that prisoners might be regarded as being a higher risk group, but also the fact that they may be less well placed to give candid answers to questions, may be less truly voluntary as donors, do you think that prison donations should have stopped long before October 1983?” He responded: “I think there is an argument for that, yes. I think there is an argument that they should have.”[727] He was frank in acknowledging this. He was right to do so. Prison donations in Northern Ireland should have stopped long before October 1983.
The armed forces were another source of blood donors throughout the 1970s and 1980s for a number of RTCs, for example Sheffield (formerly Trent).[728] Despite this cohort of donors giving rise to risks not far removed from those seen in the prison donor population, in particular the fact that they were in an environment that made it difficult to tell the truth about their personal risk factors, such as being gay, or being or having been an intravenous drug user,[729] there was less concern expressed by RTDs about donor sessions being held at military bases.[730]
Blood was also collected from the armed forces in Scotland. These sessions were less important to the service than the prison sessions (approximately 0.2% of donations was collected from the military). SNBTS has told the Inquiry that they are not aware of evidence that military personnel based in Scotland were at higher risk of Hepatitis B, HIV or Hepatitis C infection than the general Scottish or UK donor population.[731]
As in England and Wales, the Scottish transfusion directors did not consider this cohort to give rise to any special risks, albeit Dr Jack Gillon expressed a concern about the enthusiasm of the officers in charge of the blood collection in wanting the sessions to be a huge success. He recalled returning from a session “really quite concerned because I couldn’t be 100 percent sure that all of those donors were truly volunteers. I just had a feeling at the back of my mind that it was ‘You, you and you’ and I’d spoken to one or two of the donors personally. I think some of them did have reservations about answering the questions, and I came away from that session really feeling very uneasy.”[732] Dr Gillon also recalled that it was difficult to find an area private enough to be sure that the donor was telling them everything that they wanted to say.
In Northern Ireland, collections from the armed forces made “quite a significant contribution, especially in the 70s continuing in the 80s.” Dr Morris McClelland recalled “Quite a lot of sessions.” This is perhaps unsurprising because of the large army presence in Northern Ireland as a result of the Troubles. These sessions were, in the evidence of Dr Morris McClelland, a valuable source of donors at a time when the blood service was struggling to maintain the blood supplies.[733]
Unlike the RTDs from the rest of the UK, Dr Morris McClelland gave evidence that he was aware that “there was a higher incidence of hepatitis B among army donors, certainly”. He said that was his experience. However, he was unsure how much consideration he would have given to this, given how important these donors were.[734]
Workplace sessions were another important source of donors throughout the 1970s and 1980s.[735] Sessions took place at factories and other large workplaces during the normal working day. These sessions were planned by the donor management departments at the regional transfusion centres.[736]
The decline of heavy industry in the 1980s reduced these donor sessions, particularly in the more industrialised regions such as the North East of England.[737] Similarly, in Northern Ireland the largest factories had been a very valuable source of donors. Their closure, as well as the Troubles, had an adverse impact on donations.[738]
While there is no evidence to suggest that there were higher levels of blood-borne viruses in these donor populations,[739] given the context in which sessions were organised, there were risks that employees were (or at least felt) pressured to donate, and may have found it difficult to admit to risk factors that made them unsuitable to be a donor. Little consideration appears to have been given to this by any of the RTDs in the UK.[740] Much might depend on how a donor session was best to be organised: the next section in this chapter.
RTCs held donor sessions in a mixture of static and community sessions. The static sessions were those that took place in bespoke clinics.[741] In larger regions, smaller centres were set up across the region to make it easier for donors to give blood.[742] Plasmapheresis sessions took place in static clinics because plasmapheresis machines could not be easily moved.[743] For most centres, the majority of their donor sessions took place in the community and while practice varied from RTC to RTC, most centres tried to hold sessions in every part of the region they covered.[744] Sometimes sessions were held in community or church halls, sometimes at a place of work (such as a factory), sometimes in a public building such as a library and sometimes in a prison or a military establishment. Increasingly RTCs had mobile centres (“blood mobiles”)[745] that could be parked in a car park, and donors bled within the vehicle. Some RTCs used blood buses to transport donors to sessions.[746]
The number of sessions held by each centre depended on that region’s needs. Thus, for example, by 1988 the North London Blood Transfusion Centre had three static centres open between five and six days a week, together with twenty-three community sessions a week and five sessions undertaken in the blood mobile vehicle.[747]
Apart from casual or new donors attending drop-in centres, donors were invited by call-up cards. These were often postcards (North London for example used this system).[748] Other centres invited donors by letter: this was more expensive, but gave them the opportunity to provide leaflets which a donor could read in advance of a session.[749] These leaflets generally asked donors not to attend unless they could satisfy the criteria set out (in practice, that meant not being excluded by any one of a range of conditions, illnesses, or circumstances).[750]
As a general rule of thumb, between 100 and 200 donors would be bled at each session.[751] Given the voluntary nature of the donation, it was obviously important that the donor was not left to wait in a long queue before being bled. All of this meant that there was pressure on those running the sessions to process donors as quickly as possible.
Each donor would be booked in by a member of clerical staff who should have had a copy of the most up-to-date national guidelines produced by the RTDs.[752] Donors would be given written material on arrival, which set out the eligibility criteria. It was then the role of the clerk to ascertain (in the first instance at least) whether a particular donor was eligible or should be refused.[753] Although practices varied from centre to centre as to how this was done,[754] the only centre where these questions were asked orally rather than by presenting them in a written form appears to have been the Glasgow RTC.[755]
All donors would be asked to sign a form affirming that they had read and understood the information provided to them, albeit in the West of Scotland, the donors were asked to sign a separate register.[756]
The presence of some of the health conditions listed in the guidelines meant an immediate refusal. Some required referral to the medical officer for determination.
Given that the process of establishing whether a donor was eligible in the main involved either a non-medically qualified clerk asking the donor a list of pre-prepared questions about her or his health or the donor reading a leaflet about the eligibility criteria,[757] it was important that the written material was clear. However, the form that the donors were asked to sign, the NBTS 110, stated that donors must be asked whether they had ever had a number of infectious diseases including “jaundice”, but did not mention hepatitis on the revised form issued in 1985, despite the fact that at that time a donor would be ineligible to donate if she or he had had hepatitis in the previous 12 months.[758]
A medical officer[759] was to be in attendance. They would deal with any queries from the clerk (or the donor) about a particular donor’s eligibility. Such queries would in some circumstances have required the donor to be asked further questions about their health. In some cases, the query would be referred to the RTD for a decision to be made at a later date.
The fact that the majority of sessions were held in open spaces in community buildings, such as church halls and workplaces, meant that there was often, if not usually, little opportunity for private discussion between the donor and the clerk or medical officer. Thus, questions about whether or not the donor might have an infectious disease would often in effect be taking place in public,[760] and might easily be overheard. Some centres took screens so that donors could at least be separated from the main area, albeit presumably the conversation that gave rise to the need for privacy would have happened in the main area.[761] But as Dr Lorna Williamson candidly admitted “a rural setting is difficult for people who don’t want others in the village to know about their personal lives.”[762] The same could of course be said of a session that took place in a workplace, a military barracks or a prison. Following a visit to the New York Blood Center in 1984, Dr (later Professor Dame) Marcela Contreras developed an innovative system which was not adopted elsewhere. The North London Blood Transfusion Centre operated a system like a polling booth in which a donor would tick “Yes” or “No” to a questionnaire asking them whether they belonged to seven risk groups and post it in privacy into something like a ballot box, as a result of which a donation could be withdrawn if necessary.[763]
Different centres had different procedures for dealing with donors whom they considered (or suspected) were unsuitable to donate. At the Northern RTC for example, they had a book which was used to make notes about any particular donor that the clerical staff or the nursing staff felt warranted further investigation.[764] In South East Scotland there was, for a short period, a procedure where if staff had concerns about a particular donor, the donation would be taken and marked “? infective donation”. The donation was then not used.[765]
Even where donors were being asked to declare health conditions as a result of reading a leaflet rather than being orally questioned, most RTCs had no mechanism by which donors could declare themselves ineligible to donate, without losing face in front of other donors (and so perhaps fuelling speculation about the reason for their ineligibility). This problem became particularly acute when the blood service introduced leaflets setting out eligibility criteria for donors in response to the threat of HIV and AIDS, given the significant stigma associated with those infections. The exception to this was the North London Blood Transfusion Centre under the directorship of Dr Contreras, who in addition to other measures,[766] had the “polling booth” system already described.[767] This allowed donors who felt under pressure to donate (because for example they had come with work colleagues), to do the right thing and declare their health conditions without losing face.
The various different processes by which blood for transfusion was obtained for donors left open several possibilities that a donor might not realise they should not be donating blood, or felt compelled, having come to a donation session, to “go through with it” rather than withdraw. Donors had no easy way of alerting the donation team taking their blood to the possibility it might pose a risk. Opportunities to explore any issues with the medical professional supervising the session would be limited not just by time but by circumstance, for privacy could not be ensured. The constraints within which the blood services operated were not of their choosing, but there always remained loopholes through which an infected donation might slip. In better, or better resourced and equipped, sessions this might not have happened, or at least the possibility might have been reduced. It is surprising that more innovative approaches such as those implemented in North London were not adopted to provide donors with greater privacy in which they could say if their blood might pose a risk.
Donor screening is the process of assessing the risks and suitability of the individual donor who attends to make a donation.
From the early years of the blood service in England and Wales, there were attempts made by RTDs to set national standards for the selection of donors. They drew up guidelines. The first version, dated 1946, was entitled the Medical Examination and Care of Donors.[768] These guidelines were of course not binding on regional transfusion centres, for the reasons set out in the chapter on the Organisation of the Blood Services. The guidelines were updated on an ad hoc basis.
Initially donors in all four nations had to be between the ages of 18 and 65. By 10 October 1990, the North West and North East Thames RTCs had agreed that if donors had given blood at least four times in the previous five years, including once in the previous twelve months, they could continue to give blood for up to a further five years.[769] This became national policy in England and Wales (although not in Scotland) in December 1993.[770]
By the middle of 1990 in Scotland the SNBTS were recruiting donors from the age of 17.[771] The policy was described by Mairi Thornton, the National Donor Services Manager, as “an unqualified success.”[772] In Northern Ireland, they reduced the donor age limit to seventeen and a half with parental consent.[773]
In general, whole blood donors were called every six months but some centres believed that this was too conservative and encouraged more frequent donations. Dr Huw Lloyd told the Inquiry that once per every six months “was generally less frequent than was considered acceptable”[774]and by 1988/89 leaflets were amended to make it possible for donors to give blood every seventeen weeks.[775] At the National Management Committee of 16 April 1991 a decision was taken that a minimum interval of 12 weeks between donations for male donors would be accepted as a national standard.[776]
There was an emphasis on donors being healthy, or in “normal health”. This was primarily to be assessed by the donor him/herself who was said to be “the best judge”.[777] The blood services relied on donors answering the questions they were asked truthfully. This made it all the more important to set the donor sessions up in such a way that donors could refrain from donating without loss of face or worse in front of work colleagues, employers or members of their community.[778]
As the 1946 edition of “Medical Examination and Care of Donors” frankly admitted, the superficial physical medical examination carried out during the session was “in general, so incomplete and unrevealing that is in most cases not of great value.”[779] Nevertheless it was claimed that “The experienced doctor can detect at a glance the potentially unsuitable donor” and this language was modified only slightly in later editions.[780] It was acknowledged by some of the RTDs who gave evidence to this Inquiry that this is simply not so.[781]
The guidelines set out a number of different health conditions or lifestyle markers that would result in a donor being either rejected as a donor, or deferred for a period of time. From as early as 1945, when the English and Welsh RTDs began meeting, they expressed concerns about the transmission of jaundice to those receiving blood and blood products. As a result, the 1946 guidelines required first-time donors to be asked specifically whether they had had jaundice within the previous six months. The inference was that a donor who had a history of jaundice more than six months previously might be bled.[783]
On 8 August 1952 Dr William d’A Maycock, who had been made aware that the WHO’s Expert Committee on Hepatitis was about to recommend the exclusion of donors with a history of jaundice “at any time”, wrote to the RTDs recommending that the blood service should begin excluding “at once” any donor who gave a history of jaundice.[784] A decision was formally made by the RTDs to accept this recommendation at their meeting on 1 October 1952.[785]
The criteria for the deferral or rejection of a donor with a history of hepatitis or jaundice was revisited from time to time by the RTDs but remained largely unchanged[786] until November 1976 when the DHSS issued a circular which set out the recommendations of the Advisory Group on Testing for the Presence of Hepatitis B Surface Antigen and its Antibody that: “The practice of permanently excluding from the panel donors with a history of jaundice may be discontinued provided that HBsAg is not detected by reverse passive haemagglutination [(“RPHA”)] (or a test of equal sensitivity) and that the donor has not suffered from hepatitis or jaundice during the previous 12 months (paragraph 18).”[787]
This led the RTDs to update the Memorandum on the Selection, Medical Examination and Care of Donors in 1977. This updated version provided that individuals who gave a history of jaundice or hepatitis could be accepted as donors as long as they had not suffered from jaundice or hepatitis in the previous 12 months; or had not been in close contact with hepatitis or received a transfusion of blood or blood products in the previous six months and as long as their blood gave a negative reaction for the presence of HBsAg when tested by reverse passive haemagglutination (“RPHA”) or radioimmunoassay (“RIA”).[788]
While the donor selection criteria were subject to a number of further updates,[789] this particular provision remained unchanged[790] until after the introduction of Hepatitis C screening in the blood service.[791] The relaxation in 1977 was based upon a belief that tests for Hepatitis B would offer protection[792] (though these were notoriously poor at identifying all cases of infection when first introduced and, though improved, were still imprecise after introduction of the RPH test for it) and did not consider the possibility that donors who had been positive for Hepatitis B might be at increased risk of suffering from NANBH. The link between the lifestyle choices which often led to an increased risk of the former and the chances that they might suffer from NANBH was the basis for suggestions made not long after this that a surrogate test for NANBH in donations involved identifying those who had markers for Hepatitis B.[793] The relaxation should have been reconsidered much earlier than it was.
The evidence of Dr Colin Entwistle as to how this particular part of the guidelines came into being is informative. He was chair of the working committee tasked with producing these guidelines.[794] He nevertheless gave evidence that he himself did not agree with the practice of allowing those with a history of jaundice or hepatitis more than 12 months previously to donate. The guidelines were, according to him, “a common agreed policy which everyone can agree to”, in other words they should not be seen as a record of best practice.[795] This is open to the comment that the search for a policy all could sign up to can become a search for the lowest common denominator.[796] It ought to be the case that documents such as this were reflective of up-to-date and developing knowledge, so as to provide a lead – and it is plain from what Dr Entwistle had to say that it was not. I do not criticise him for this, for it is in the nature of working parties that some views must yield to others, but the result is not one which the working party should have adopted.
It is worth noting that both the DHSS circular and the subsequent publications of the Memoranda on the Care and Selection of Donors in 1983 and 1985[797] were at odds with two important international documents in so far as the acceptance of donations from those who had previously suffered from jaundice was concerned. First, the recommendations of the International Society of Blood Transfusion set out in its 1976 publication Criteria for the Selection of Blood Donors its recommendation that any prospective donor who gave a history of viral hepatitis at any time should be excluded (save where the history was within the first months of life).[798] Second, the equivalent American Red Cross leaflet envisaged the permanent deferral of persons with a past history of viral hepatitis, and was appended to the recommendations of the Committee of Ministers to the Council of Europe in June 1983 as an example of good practice for national blood transfusion services wishing to draw up their own leaflets.[799]
It is particularly concerning that the 1983 and 1985 repetitions of this approach came at times when there was widespread concern about keeping blood safe from being a carrier of the suspected (and latterly known) viral cause of AIDS. The introduction of a surrogate test for the cause of AIDS which was under consideration in 1983 aimed to use Hepatitis B markers as indicative of certain lifestyle patterns which it was thought would be more conducive to viral infections, such as the putative viral cause of AIDS. It is inconsistent on the one hand to accept evidence of having had hepatitis as a reason to screen out donations because of a possibly increased risk they might cause AIDS, and on the other to maintain criteria that at an individual level permitted the continued donation of blood by someone who fell in that category.
By at least 1960 the guidelines also included a provision that those who had been transfused with blood or plasma within the last six months were to be deferred.[800] Dr Tony Napier in his oral evidence explained that the rationale for this was the potential opportunity for the transmission of hepatitis and that by six months “it would become apparent whether infection had taken place or not.”[801]
From 1977 those who were suspected of or admitted to illicit drug-taking were to be debarred.[802] However, it is unclear how those who might have fallen into this category would be identified (unless there were needle track marks in the arm from which the donation was to be taken), or even what attempts might typically be made to identify them. The form which donors were asked to sign made no reference to such drug use as an exclusionary factor. Dr Patricia Hewitt could not recall any measures in place (other than in relation to the AIDS leaflets)[803] to prevent those with a history of intravenous drug use from giving blood and did not recall whether any consideration was given expressly to formulating leaflets directed at those who might have used intravenous drugs.[804] Dr Morris McClelland thought it would be based “on interview and the general assessment” but could not remember “that there would have been very much specific beyond that asked of donors that might have uncovered that kind of thing.”[805]
Like England, Scotland had, prior to at least 1980, rejected all those with a history of hepatitis, but by March 1980[806] were only excluding those blood donors with a history of jaundice within the previous 12 months. This was primarily because in Scotland they followed the English selection criteria.[807] This was unsurprising given that the working party responsible for drafting the guidelines had a representative of the Scottish RTDs on it.
In 1982 Dr Brian McClelland and his team at the South East Scotland Transfusion Centre at Edinburgh drew up their own guidelines entitled Guide to Selection of Blood Donors.[808] This stated that those with either jaundice or hepatitis should be deferred for a year, any donor who knew she or he was a carrier for serum hepatitis should be put off service and otherwise the guidance was “at their first donation 1 year after their recovery record ‘Hepatitis’ on donor’s name slip and inform Hepatitis lab.”[809] Dr Brian McClelland in his oral evidence said he could not remember why this was the case but thought it was so that the donation could be taken out of circulation.[810] If this was indeed the practice, it is not clear why the guidelines did not make it clear to the donor attendant (who could in turn inform the donor) that in fact a history of hepatitis debarred individuals from donating.
These A-Z guidelines identified some conditions for which the advice was to defer and some for which the advice was that the donor be regarded as permanently unfit to donate. In relation to drug abuse, however, the stipulated action was that the doctor or nurse should be consulted.[811] This was accompanied by advice that at least six months should have elapsed from the use of parenteral drugs before a donor could donate because of the risk of serum hepatitis, and that there should be borne in mind “the possibility that the history given by these donors regarding the abuse of drugs may be unreliable.”[812] In other words, the guidelines did not provide for the automatic exclusion or deferment of those with a past history of drug misuse. Dr Brian McClelland in oral evidence thought that donor attendants would defer such donors but could not say when permanent deferral became the practice, noting that: “It was always a problematical thing to judge and we did discover that there were people who told us they were not drug abusers, who turned out to be hepatitis C positive, and it transpired on full questioning that they had injected drugs perhaps once 20 years ago and did not consider themselves to be drug abusers. But I cannot give you an answer to your specific question.”[813]
In April 1986 the Scottish centre directors agreed that SNBTS should produce its own selection criteria for donors, based on South East Scotland’s A-Z document.[814] SNBTS published Guidance for the Selection, Medical Examination and Care of Blood Donors in November 1987.[815] This allowed:
The blood services of the UK came together in 1989 to publish under the UK Blood Transfusion Service/National Institute for Biological Standards and Control (“UKBTS/NIBSC”) Liaison Group, the first edition of what became known as the “Red Book”.[817] The criterion with respect to hepatitis and jaundice (they were separately listed) was that a donor should be allowed to donate 12 months after recovery.[818] This left open a possibility that carriers of Hepatitis C cases might continue to donate. That was unwise, since in the case of a chronic infection persisting after an initial acute phase, it depended on how “recovery” was defined in practice.
It was not until the second edition of the Red Book was published in 1993,[819] by which time Hepatitis C screening had been introduced throughout the UK’s blood services, that the guidelines explicitly rejected those infected with Hepatitis C.[820]
Because of the generality with which groups are defined, it is almost inevitable that individual – indeed, most – members of some groups may not be infective, though the group as a whole shows a higher prevalence of disease than the general population. These individuals may feel blamed for the attributes of others, and regard spurning a donation which they wished to give to benefit fellow humans as being churlish, discriminatory or worse. In the 1970s and 1980s gay communities were groups which viewed overall had within them a higher prevalence of infection. The same was certainly true of those who took (or had ever taken) drugs intravenously. Those in prison, viewed overall, were a group in which there was a markedly increased prevalence of infection. It has been suggested it was true of members of the armed services. Merely to be a member of such a group did not mean that an individual was infected. Nonetheless, in the absence of a reliable test for either HIV or NANBH, it reduced the risk generally to decline donations from anyone who was a member of such a group.
Unfortunately, blood continued to be taken from those in prison until the end of 1984 in the UK, long after it had been recognised that prisoners as a group were much more likely to suffer from hepatitis than those in free society. Whilst sourcing blood from serving prisoners persisted, the risk was increased, perhaps only by a little, but undoubtedly. The moral argument that prisoners should have the opportunity of being altruistic in donating blood, as part of the rehabilitative process, has much to recommend it. It echoes the rationale for having the sentencing option of requiring community service as one way in which a convicted person may be helped to live a better life in future. Where there is a serious threat to health, though, which can be reduced by avoiding taking donations from higher-risk groups, the altruism of the would-be donor is better served by standing aside from donation,[821] rather than giving blood, and the system as a whole should not ask such a donor to provide it, for to do so compromises both the health of the general population and suggests erroneously that the moral thing to do is to donate rather than not to do so.
The voluntary donation system helped the process of donor selection. In general, donors would not want to give a blood donation if they felt they might be creating a disproportionate risk of harm by doing so: spreading disease, rather than saving lives. Accordingly, information sheets advising would-be donors whether they should defer donating for the time being were of critical importance in helping the system to identify the most appropriate donors – or, put the other way round, to avoid donations from those who might be the source of increased risk. A significant emphasis was thus placed on “donor leaflets” in the fight against the spread of (first) hepatitis and (second) the cause of AIDS.
The Expert Committee on Hepatitis of the WHO, in 1952, identified not just donor selection but donor screening as necessary steps in seeking to reduce the impact of serum hepatitis. Both hold good, too, for seeking to reduce the impact of AIDS. Just as is the case with NANBH/Hepatitis C, so too HIV infection may have a long phase when few if any symptoms are apparent. Care needs to be taken, therefore, not to limit donor exclusions to those who are visibly suffering, or report significant symptoms. Taking personal history is a relevant part of donor screening. It is plain that this is best done by personal donor interviews, coupled with carefully worded donor questionnaires – if time, space, and resources permit it. They did not always do so. In Dr Brian McClelland’s evidence he spoke of the attempts made in Edinburgh and the South East of Scotland to introduce a comprehensive questionnaire (of especial value where the cramped nature of many places where donor sessions were held) which had to be abandoned due to insufficient staff; the best that could be achieved was a personal interview of all new donors, finally introduced in 1992.[822] This evidence shows that it would not necessarily have been easy to introduce direct confidential questioning of the private lives of donors: but it is regrettable that it was not done, at least in some form, when AIDS first broke, even if it were some combination of a personal questionnaire and a face-to-face encounter informing a donor of the need to signify[823] if their blood should be used for research purposes rather than transfusion because they were or had been associated with a group at higher risk of infection.[824]
In 1982, the DHSS Central Management Services published a report called Blood: Record Keeping and Stock Control.[825] This made a number of recommendations as to the role of the RTCs in promoting good practice in blood transfusion, including “economies in blood usage.”[826]
The DHSS issued a circular on 28 February 1983 to (amongst others) regional administrators which refers to Blood transfusion: Record-keeping and Stock Control Arrangements. This stated:
“To facilitate a Regional review of policies, it is suggested that RMOs [regional medical officers] should convene regular meetings between their Regional Transfusion Directors (RTDs) and the consultants responsible for the hospital blood banks in their Regions to consider matters such as current and future requirements for blood, the scope for economies in blood usage, the proportion of plasma-reduced blood to be supplied, the use of ad hoc deliveries and the amount of stock which becomes time-expired in blood banks. The meetings should also provide the forum for the exchange of ideas as to what constitutes ‘good practice’ in the Region with regard to blood supplies.”[827]
In June 1989 Dr Harold Gunson produced a report for the NBTS Co-ordinating Committee in which he stated that the NBTS saw its professional role as encouraging the minimum use of blood and blood products consistent with clinical need and patient safety. He encouraged RTCs to “question atypical and abnormally high orders” and issue some products on a “case by case basis”. He also envisaged the RTCs performing a monitoring role, which would only be effective if the RTCs remained the sole suppliers of Blood Products Laboratory (“BPL”) products to hospitals in their regions.[828]
The extent to which individual regional transfusion directors considered they had a role in educating their colleagues on the use of blood varied from RTC to RTC and also developed over time:
Of particular note was Professor Contreras’ oral and written evidence, which made it clear that she considered it to be a key role of the RTCs to educate clinicians about the responsible and ethical use of blood. In so doing she:
At the other extreme, Dr Entwistle, the director of the Oxford Centre, did not consider the education of his colleagues on the use of blood to be part of his role.[836] This is despite the fact that in Oxford the haematologists in the region used to meet every three months or so.[837]
The SNBTS directors examined the DHSS publication Blood: Record Keeping and Stock Control and produced modified recommendations applicable to Scotland, starting with a recommendation that RTCs “accept a formal responsibility for encouraging good practice” in the hospital blood banks they supplied.[838]
Dr Gamal Gabra recalled that Dr Wallace, then director for the West of Scotland, was an early promoter of using blood components rather than whole blood and that clinicians “gradually” accepted this approach.[839] Professor Urbaniak set up a Hospital Transfusion Committee in the Aberdeen Royal Infirmary to monitor usage and compliance with maximum surgical blood ordering schedules for each operation and procedure that might require a transfusion, apart from those with risk of massive rapid blood loss. As a result, the use of whole blood rather than red cell concentrates reduced and the total number of transfusions per operation was reduced.[840] Dr Boulton explained in his oral evidence how during his time in Edinburgh he did audits of blood usage around the hospital, working closely with cardiac surgeons to achieve a more rational use of red cell concentrates with less emphasis on the freshness of the blood.[841]
Dr Morris McClelland considered that he had a role in persuading colleagues to use less whole blood and more red cell concentrates; that “The most effective route of influence” was the haematologists and laboratory staff in charge of hospital blood banks who in turn influenced the clinicians in each speciality.[842] He told the Inquiry that he and Dr Chitra Bharucha took every opportunity to influence these staff who, in turn, were in a position to influence the clinical users of blood in each speciality. The rapid uptake of red cell concentrates from 20% of the Belfast output to 75-80% in the space of three to four years was, in his view, testament to the success of their work.[843]
One of the obvious steps that treating clinicians could (and should) have taken once it was understood that HIV was a blood-borne infection, was to reduce all patients’ exposure to blood and blood products as far as reasonably practicable consistent with providing treatment. This could be done in two ways. First, less product could be given.[844] The second way this could have been achieved was by prescribing products that had a lower chance of being infected with HIV, namely single-donor products, or small pooled products.[845]
RTDs were asked about the extent to which they played a role in persuading treating clinicians (whatever their specialty) to take either of these steps.
They did not, on the whole, consider that they had a role in trying to influence treating clinicians to prescribe one product over another on the grounds of safety. A principal reason for this was respect for the clinical freedom of doctors.[846] Two exceptions to this were both directors of the Trent RTC. Dr Charles Bowley sought to make a case for using better quality cryoprecipitate instead of imported factor concentrates.[847] His successor, Dr William Wagstaff, gave oral evidence that he tried to persuade haemophilia clinicians to revert to cryoprecipitate and keep away from commercial products as a result of HIV/AIDS. However, this had no impact on their prescribing policies.[848]
All RTDs who were in post in the years 1982-1984 before blood products were heat treated against HIV gave evidence that had they been asked to increase their production of cryoprecipitate (as a much lower-risk product) during the mid 1980s, they would have been able to do so, and quickly.[849] They were all clear that no such request was made of them by treating clinicians and so no steps were taken by RTDs to achieve this.[850]
Dr Morris McClelland, like his colleagues in England and Wales, did not consider it to be his place to question the prescribing practice of Dr Elizabeth Mayne,[851] the Belfast haemophilia director, stating: “I wouldn’t have seen that it was appropriate for -- that I could really influence such change in prescribing patterns.”[852]
Like the RTCs on the mainland, Belfast RTC would have been able to increase its production of cryoprecipitate to 20,000 packs per annum if they had been asked to. No such request was made.[853]
Dr Cash was not afraid to express his views about the circumstances in which different blood products should be used. For example:
Following a visit to New York in October/November 1983 and his participation in the WHO meeting on AIDS in November 1983, Dr Brian McClelland prepared a paper entitled “Acquired Immune Deficiency Syndrome and Transfusion” which he circulated to SNBTS and his haemophilia director colleagues. Unsurprisingly, the paper focuses on the steps SNBTS could take to reduce the risk of AIDS getting into the blood supply in Scotland. However, it does contain a section entitled Measures to Promote the Safe Use of Existing Blood Products which makes a number of proposals including that “The use of single donor or small pool cryoprecipitate for haemophilia therapy should be reassessed. In particular, the extent to which requirements of good manufacturing practice limit the production of small pool freeze-dried cryoprecipitate should be re-examined and the costs of this product estimated in relation to intermediate factor VIII concentrate.”[858]
The extent to which the views of Professor Cash and Dr Brian McClelland influenced the prescribing practices of haemophilia clinicians is doubtful.[859] There does appear to have been a modest response to the threat of AIDS from the director of the Aberdeen Haemophilia Centre, Dr Bruce Bennett. Following discussion between him and Dr Urbaniak, Dr Urbaniak increased the production of cryoprecipitate from 153 units to 425 units between 1983 and 1986.[860]
Dr Gabra in his oral evidence stated that the Glasgow RTC could not have increased their production in Glasgow of cryoprecipitate had they been asked, because they would have had to establish the facilities to do so.[861]
The responses of all four blood services acting as one, nationally, to screen blood donations are set out in the chapters on HIV Screening and Hepatitis C Screening.
Once a donation had reacted to a screening test (“a reactive donation”), or a report had been made to the RTC that gave rise to a suspicion that a particular donation had caused a transfusion-transmitted infection to the end recipient (from “an implicated donor”), then RTCs had to decide what, if anything, they should do.
This section considers what if any steps the blood services took to:
It is clear that none of these steps could be taken without the RTC having accurate and searchable records on all of their donors, and the fate of all of their donations. The issue of records and record-keeping is addressed below.
This section does not address:
The evidence from the RTCs was that they had reasonably robust processes for dealing with a reactive donation. The first step was immediately to quarantine the reactive donation while further confirmatory testing was carried out. This was certainly the practice at the North London RTC.[862] In the event that the confirmatory tests were positive, the second stage in the process was to trace:
This appears to have been fairly standard practice, and was for example something that the Yorkshire RTC did.[864] The third stage was to identify whether any plasma from the donor had gone to BPL, and if so, inform BPL of that.[865] There is certainly plenty of evidence of RTCs making reports to BPL of infected donations having been provided to them.[866] RTCs could expect BPL, after investigation, to notify them of the batch numbers of any fractionated products to which the potentially infected donations had contributed, and ask the RTCs for their assistance in finding out where those batches went, so that the patients could be followed up.[867]
What is less clear from the evidence is the extent to which, prior to the formal lookback programmes,[868] individual RTCs investigated whether previous donations from an infected donor might have been infected and if so, what happened to them. Certainly until the formal lookback programmes were instituted, there was no obligation on the RTCs to undertake this work.
The expectations on RTCs in England to notify and then counsel donors who were found to be positive for HIV was clearly set out in the CMO’s “Dear Doctor” letter to all doctors in England dated 1 October 1985. This states “donors will be interviewed and counselled about the significance of test results by senior NBTS medical staff who have received training in counselling.”[869] Thus for example, the North London RTC always counselled donors who tested positive for HIV themselves.[870]
There was however no clear guidance to RTCs setting out their obligations to inform and counsel donors found to be positive for Hepatitis B or Hepatitis C. Thus, unsurprisingly, practice differed:
Indeed, donors who were found positive in the three-centre trial of Hepatitis C screening kits prior to the introduction of Hepatitis C screening in September 1991 were not to be informed, followed up or counselled.[875]
The actions of SNBTS in 1984 in response to the news from Dr Christopher Ludlam on 25 October of that year, that six of his patients from the Edinburgh Haemophilia Centre had developed antibodies to HTLV-III after exposure to the Protein Fractionation Centre (“PFC”) batch 023110090 (“the PFC batch”), is worth setting out in a little detail. Initially a decision was made by Dr Brian McClelland and Dr Cash not to recall the PFC batch.[876] By 2 November Dr Ludlam had confirmed to Dr Brian McClelland that in fact 16 of his patients had developed the antibody, and all of them (or possibly 15 of them), had been exposed to the PFC batch. On 3 November Dr Brian McClelland and Dr Boulton contacted all the Scottish RTCs and the Northern Irish RTC to recall any of the batch that was still being held.[877] Dr Brian McClelland told the Inquiry in his oral evidence that: “As it emerged, there was very little of that batch to recall, apart from a few units that were still in the Aberdeen Transfusion Centre. All the rest of it had been transfused some time previously.”[878] No other batches were recalled.[879] The donation which had infected the batch was not identified.[880]
From as early as the 1940s, the importance of record-keeping was emphasised as an essential part of any strategy to reduce the risks of transmission of infections such as hepatitis.[881] It is not surprising therefore that:
One of the consequences of a system of RTCs operating as separate fiefdoms[885] was that each centre had different record-keeping systems. While there were attempts made by the RTDs to standardise some key documents,[886] local practices developed.
Of course during the 1970s and into the 1980s, RTC records were on paper. Keeping accurate records was a challenge. Records about the donor and their donation history were generated at donor sessions in the community,[887] while records in relation to the donation itself were generated in the main at the RTC during the processing phase. Clearly the two types of records had to be reconciled, and importantly, searchable, so that any donation (together with all its component parts) could be traced, and information obtained as to where it had been sent.
Added to this, some RTCs kept the records of donors who tested positive for HIV and hepatitis separately from their other records, presumably to ensure their confidentiality.[888]
One of the major problems the RTCs had in tracing the eventual fate of the products that they supplied to hospitals, was that unlike in Scotland, where four of the five transfusion centres also carried out blood banking for the hospitals in which they were located, the English and Welsh RTCs had no access to the records of the hospitals and haemophilia centres that received their products. Thus once a labile component, or even a vial of Factor 8 produced by BPL, left the RTC, the RTC had to rely on the information provided to it from the recipient hospital to learn its fate. The Inquiry heard a wealth of evidence to suggest that hospitals were not complying with their obligations to keep accurate records of the transfusion of blood and blood products “to enable each unit of blood to be traced from donation to disposal” as required in the 1983 guidance.[889] The Inquiry has repeatedly heard evidence from individuals who have had a blood transfusion with no record at all being made in their medical records, and countless more where the serial numbers of the transfusion were not recorded in the patient’s records.
Professor Contreras considered the problem to stem not from the hospital blood bank, but from the record-keeping of the clinicians actually receiving the blood from the blood bank.[890]
Even once records were computerised, the RTC computer systems remained separate and were not necessarily compatible with one another – they did not communicate one with the other.[891] In England in 1995 a national computer was introduced, but the system was divided into the three separate zones that were created at that time, and records initially could not be shared across the zones.[892] It was not until July 2008 that a truly national system was developed.[893] In Scotland, a Scottish national computer system was introduced in the late 1980s (DOBBIN), but the records of each of the five RTCs were segregated one from the other and could not be shared.[894] It was not until 1997/1998 that records could be shared between and across the RTCs.[895]
This meant that where a donor had been rejected by one transfusion centre, there would be nothing stopping them from trying to donate at another since checks on new donors to see whether they had already been rejected by another RTC were not possible.[896] Some attempts were made to remedy this obvious deficiency in the system. Dr Jean Harrison in her statement recalls the consultants responsible for microbiology sharing details of those donors who were unsuitable to donate.[897] Her RTC had a system of “blacklisted” donors – but this operated only within the RTC.[898]
As well as paper records, RTCs began keeping samples of donations, thus making tracing and lookbacks more effective. For example:
Prior to 1992, the recommendation in the first edition of the Red Book was that records should be kept for 15 years.[903] In 1992 Dr Lloyd, Dr Alan Beal and Mr Tony Martina produced a report entitled Record Storage Report for the National Blood Transfusion Service in England and Wales for the National Directorate. This recommended that donor and donation records and policy and management records, as well as records directly linked to donor and donation records such as QA reports, should be kept for 30 years.[904]
In 1946 a system was devised of reporting cases of serum hepatitis to Dr Maycock.[905]
At a meeting of RTDs in November 1973[906] it was agreed that:
By 1980 the system for reporting transfusion reactions was for Dr John Barbara to collate known cases, and send a report annually to the Centre for Disease Surveillance and Control at the Public Health Laboratory Service.[910] It appears that these reports did not simply record the data from the North London Blood Transfusion Centre: there is evidence of other RTCs sharing information with Dr Barbara concerning the number of donors found to have HBsAg, so that he could report it for the national survey.[911]
On 29 January 1985 the Expert Advisory Group on AIDS agreed unanimously that statutory notification of HIV was not required and that an informal approach was to be preferred.[912]
This informal approach involved RTDs reporting incidents of HIV-infected donors to
Dr Gunson.[913]
At a meeting of the SNBTS directors on 20 June 1985 it was agreed that a system for reporting AIDS cases to the Communicable Diseases (Scotland) Unit should be agreed.[914] At the meeting on 19 November 1985, there was agreement that the Unit’s form should be used.[915]
The focus of information sharing at the Belfast RTC was for donor selection. The Belfast RTC encouraged hospital clinicians and GPs to report to them cases of transfusion-associated hepatitis but rarely received reports from GPs.[916] Dr Bharucha recalls only two blood donors who tested positive for HIV who were followed up and did not donate again.[917]
In early July, probably before the Centre for Disease Control and Prevention (“CDC”) published its report that people with haemophilia in the US had contracted AIDS after receiving factor concentrates,[918] the NIBSC[919] was alerted to reports that plasma from homosexual drug-takers “contains a sort of virus” which might lie undetected but “when used for Factor VIII … becomes active again” and that “It seems that 400 haemophiliacs in the USA have exhibited signs of the virus.” Dr Joseph Smith at the NIBSC informed Dr Gunson in his capacity as consultant adviser in blood transfusion. Dr Gunson then in turn alerted civil servants at the DHSS to this.[920] This happened on, or possibly before, 16 July 1982.[921] However, months would elapse before AIDS became the subject of collective discussion by the RTDs in England and Wales or by the SNBTS directors.
The RTDs held one of their regular meetings on 20 September 1982 but there was no discussion of AIDS.[922] Nor was the threat of AIDS considered at the inaugural meeting of the UK Working Party on Transfusion-Associated Hepatitis on 27 September 1982, a meeting attended by Dr Gunson and several RTDs.[923] It was not raised at the next meeting of RTDs on 14 January 1983,[924] nor at the meeting of the Advisory Committee of the NBTS on 10 January 1983.[925] A brief mention came, finally, at the second meeting of the UK Working Party of Transfusion-Associated Hepatitis on 18 January 1983.[926] However, whilst Dr John Craske “summarised the current situation and mentioned the involvement of homosexuals”, and the minutes recorded that in the US “it is recommended that homosexuals with AIDS be deferred from donating blood or organs”, there was no consideration of the UK following suit. It was not until the Working Party’s third meeting on 20 April 1983 that the possibility of taking action was mooted for the first time and in the following, rather tentative, terms: “Dr Gunson asked members of the working party to bear the topic in mind and consider the possibility of producing a pamphlet for donors illustrating the AIDS risk groups. He was aware that this might have adverse repercussions for donor recruitment etc.”[927] However, the potential effects on arrangements to supply plasma to BPL came under consideration. The Working Party anticipated that the uptake of cryoprecipitate would rise, particularly for those who had not previously received concentrates[928] and that this would mean a drop in supply to BPL.
A week later, at the meeting of the Central Blood Laboratories Authority on 27 April, Dr Gunson reported that the RTDs “had considered all the American literature on this subject, and at the next meeting of their Committee it would be recommended that no further measures be taken, apart from those already being carried out.”[929] As no specific measures had yet been taken by RTDs (and indeed as the subject had not yet been discussed at a meeting of RTDs), the reference to measures “already being carried out” is likely to refer merely to existing donor screening practice.
AIDS was finally discussed at the regular meeting of RTDs on 18 May 1983, some ten months after the Morbidity and Mortality Weekly Report of three cases of suspected AIDS in people with haemophilia in the US.[930] Four options were identified by Dr Gunson for consideration by RTDs:
A pamphlet prepared by Dr Brian McClelland was also considered.[932] The RTDs rejected options (1) and (2).[933] Instead it was agreed that contact would be made with the Gay Society stating that, until more was known, homosexuals should be asked not to donate blood, and that Dr Tom Davies and Dr Barbara would draw up a leaflet on AIDS which would be circulated to RTDs for comment.[934] It appeared to be understood at that stage that this was something that required relatively quick action: the minutes record the hope that the leaflet could be ready for printing in six weeks and that Dr Diana Walford would try and have it printed through the DHSS as quickly as possible.[935]
Following the meeting Dr Wagstaff wrote to RTDs on 7 June 1983 to ask for feedback on questions raised by senior staff within the DHSS, who were said to be “a little perturbed that the low key approach being recommended by the NBTS is at odds with the more aggressive measures being taken in the United States”.[936]
Dr Wagstaff sent the proposed leaflet to RTDs on 6 July 1983. His covering letter explained that most RTDs strongly felt that the approach to donors should be as low key as possible and were reluctant to hand the leaflet to every donor or send it out as part of the call-up material, but that a small number of RTDs might be asked to run a kind of trial by posting or handing out the leaflets. He recorded the general opinion that the “illness notice” be amended to include unexpected loss of weight and whether the person was in good health or had needed to see a doctor recently.[937]
It was not until 1 September 1983 that the AIDS leaflet was finally published.[938] The reasons for that delay, and the limitations of the leaflet’s wording, are explored in the chapter on Role of Government: Response to Risk. However, it would have been open to RTDs to take their own local action and produce their own leaflets in the meantime. The Birmingham RTC did so,[939] as did Edinburgh,[940] but most centres waited for the DHSS’s leaflet.
When the RTDs met again on 22 September 1983, Dr Wagstaff reported that centres had been encouraged to use differing methods of distribution. The three methods being used were: posting of leaflets with call-up cards, handing leaflets to donors, and making leaflets available at sessions for donors to pick up. The DHSS requested feedback on donor reaction to the leaflet by the end of November at the latest.[941]
A few days later, at the meeting of the Working Party on Transfusion-Associated Hepatitis, it was agreed to minute, and bring to the attention of the RTDs, the Working Party’s preference for a uniform approach to the use of the leaflets.[942]
The next regular meeting of RTDs took place on 25 January 1984, at which it was reported that no offence had been caused to donors regarding the introduction of the AIDS leaflet at sessions.[943]
The Advisory Committee to the NBTS discussed the AIDS leaflet at its 10 April 1984 meeting. The six-month trial of the leaflet was now complete and the survey of RTDs showed little adverse comment. The DHSS now proposed to prepare, in consultation with RTDs, a revised version of the leaflet for submission to ministers. Dr Keith Rogers suggested that RTDs should adopt “a more aggressive approach” to discourage high-risk donors from giving blood. The Committee recommended that although the method of distribution during the trial period had been left to the discretion of RTDs, ministers should now consider whether the revised leaflet should be sent with the call-up cards in all regions.[944] At the meeting of RTDs the following day, the importance of discouraging high-risk groups from being blood donors was stressed as was the awareness of sessional medical officers in ensuring the fitness of potential donors.[945]
At the meeting of RTDs of 11 July 1984 it was reported that the Divisions had sent comments on the proposed revised AIDS leaflet to Dr Alison Smithies and that the draft would be revised.[946] There was no discussion at the next meeting in October.[947] By the time of the meeting of the Advisory Committee to the NBTS on 8 November 1984 it was reported that ministers had accepted the recommendation of a uniform system of distribution and that the leaflets would shortly be distributed to RTCs for issue individually to every donor. The Committee “advised on the particular problems of getting the leaflet to new donors, and in its use at industrial sessions, and also noted that there would be some cost implications for Centres using a card call-up system.”[948]
A paper prepared for the Working Group on AIDS meeting on 27 November 1984 suggested that it was possible to go further than the use of the leaflets and discourage high-risk donors not to give blood by organising (as was said to have been done in some centres) “more intensive interviewing of donors”, which might be particularly appropriate in areas where it was known that there was an increased population of homosexuals and drug abusers.[949] However, the Working Group was not in favour of closer questioning of donors “to see if they were homosexual etc”, concluding that the leaflet was sufficient: “There was concern that too close a questioning might be counterproductive”, according to Dr Michael Abrams’ report on the meeting to Dr Harris.[950] Notes by one attendee at the meeting reported on the questionnaire being trialled at the North London RTC, offering donors the chance to elect for their blood to be used for research; it was also noted that Dr Contreras and Dr Richard Tedder had met with “London Gay Reps” the previous week and “Got strong message that some homosexuals are still continuing to donate.”[951]
By December 1984 the promised revised leaflet had not yet been made available although, according to a meeting of Western Division NBTS consultants on 7 December, four centres had produced their own.[952]
At their January 1985 meeting, the RTDs expressed anger at the continuing lack of the revised leaflet (as well as frustration at a lack of information regarding progress in relation to AIDS more generally). Dr Gunson reported that the new leaflet would be available on 1 February and that it was expected that a “positive approach to its distribution” would be insisted upon.[953] There was also some discussion about an AIDS poster for donor sessions, which Dr Smithies was said to be proceeding with.
The second version of the AIDS leaflet was at last made available for distribution in England and Wales from 1 February 1985.[954] The reasons for the delay in the production of the second leaflet, and the significance of the changes in the leaflet’s wording, are explored in the chapter on Role of Government: Response to Risk.
In the meantime the Expert Advisory Group on AIDS (“EAGA”) held its first meeting on 29 January 1985, with Dr Abrams in the chair and the CMO, Dr Donald Acheson, in attendance for part of the meeting. It concluded that the blood donor leaflet (likely to have been a reference to the revised leaflet about to be introduced) was not “sufficiently forceful” and needed some redrafting, “particularly with regard to its objective of persuading homosexuals not to donate blood. Consideration should be given to the introduction of some means by which the ‘closetted’ [sic] homosexual – possibly faced at a visit to a NBTS Centre with advice not to give blood – could unobtrusively withdraw from the system.”[955] It seems, therefore, that even before publication of the second leaflet it was recognised that it did not go far enough. However, there was no consideration of this at the next meetings of RTDs on 17 April 1985 and 10 July 1985.[956]
A third version of the AIDS leaflet was available from September 1985.[957] When, in early October 1985, the Eastern Division consultants in the NBTS met, the new AIDS leaflet was criticised and it was recorded that “most Centres were sending an explanatory letter in addition.” The most worrying aspect of the leaflet was said to be that it implied that the anti HTLV-3 was a test for AIDS.[958] The focus of discussion at the next meeting of RTDs on 9 October 1985 was the imminent introduction (on 14 October) of screening and there was no further discussion regarding the leaflets or their use.[959]
Neither the SNBTS directors regular meeting on 14 September 1982 nor the directors’ next meeting on 14 December 1982 contained any discussion of AIDS.[960] AIDS was briefly considered at a meeting on 21 January 1983 between SNBTS directors and haemophilia centre directors in Scotland: Dr Cash drew attention to recent articles in the US and UK (and circulated a Morbidity and Mortality Weekly Report extract) and Dr Ludlam referred to a letter and questionnaire being sent to UK haemophilia centre directors.[961] There was, however, no exploration of any possible action for the transfusion service by way of risk reduction.
The SNBTS directors met again on 29 March 1983. Although consideration was given to the collection of blood in prisons and borstals, the trigger for this was the Medicines Inspectorate’s criticisms of the practice, rather than any particular concern regarding AIDS risks, which (surprisingly) did not feature in the meeting at all.[962]
SNBTS directors finally discussed the implications of AIDS for blood donation at a meeting on 24 May 1983 of the SNBTS Co-ordinating Group. Dr Ruthven Mitchell had introduced into the health questionnaire to donors a question inviting those who were worried about AIDS to consult the doctor at the session. Dr Urbaniak had decided not to do anything locally, “his view being that once a donor had entered the session it was too late to make an approach and the problem was minor in NE Scotland”.[963] Dr Brian McClelland had prepared a leaflet (which he tabled), detailing those donors who should refrain from donating blood.[964] Dr Cash reported on what had been discussed at the recent meeting of RTDs and agreed to contact Dr Barbara for information about the proposed leaflet, after which he would arrange a meeting with the Scottish Home and Health Department (“SHHD”) to discuss the provision of information which directors could use if they wished.[965]
At the SNBTS directors meeting on 14 June, attended also by Dr Gunson, the latter explained that he had edited the leaflet currently being considered for England and Wales, adopting a question and answer format, after DHSS officials expressed the view that it would not have the required impact, and that he had identified homosexual men (especially those with multiple partners), drug addicts and anyone who had sexual contact with an AIDS sufferer as donors who the blood service would prefer not to see for the time being. Dr Brian McClelland explained that he had amended his leaflet following discussion with the Scottish Homosexual Rights Group.[966] The meeting acknowledged that if the purpose of the leaflet was to deter donors it would have to be issued before they attended a donor session. There was also discussion on how best to deter certain donors without causing offence to others, with the suggestion that a wide audience could be addressed through radio and television (although this suggestion does not appear to have been acted upon).[967] Dr Brian McClelland told the Inquiry that he made clear to the other directors that the leaflet was “public property”; ie that it could be used by them.[968]
By August 1983 the expectation was that SNBTS would use the leaflet that was being produced by the DHSS and would be published on 1 September. The Co-ordinating Group of SNBTS met on 30 August 1983 and its minutes note that each RTC now had a supply of AIDS leaflets pending the lifting of the embargo on their release throughout the UK by the Minister for Health, and that Dr Cash had written to each RTD to explain that the method of issue was at their discretion.[969]
In Scotland a range of different methods for use of this leaflet were deployed:[970] in the north the leaflets were on display with other publicity leaflets at donor sessions and in plasmapheresis rooms;[971] in the North East they were available at all mobile and fixed site sessions;[972] and in the East they were “on display at the clerking desk” and anyone requesting information was referred to the medical officer on duty. In the West the leaflets were available on request with the medical officer at sessions and Dr Mitchell had incorporated into his “health notice” the question: “Have you heard about AIDS? If you wish to know more you may ask the Medical Officer at the session in confidence or your General Practitioner or write to the Transfusion Director.”[973] In the South East the leaflets were made available at the donor sessions.[974] In Belfast, Dr Morris McClelland had not as of mid September received the leaflets but would make them available at donor sessions once he did.[975]
The SNBTS directors discussed the methods of distributing leaflets again at their meeting on 8 December 1983, where it was agreed that a more active approach would now be “acceptable”.[976] It was felt that each donor should receive a copy and that the health questionnaire should include the question: “Have you read and understood the leaflet on AIDS?” It was also considered that the leaflet should be revised and the plan within SNBTS was to do so without waiting for the DHSS. It was agreed that no further action would be taken until a revised leaflet had been issued and Dr Brian McClelland agreed to produce a revised version for consideration by the Scottish directors.[977]
At a meeting of SNBTS directors and haemophilia centre directors on 2 February 1984 there was a discussion about the effectiveness of the leaflet and it was felt that “some modifications might be made” and emphasised that the leaflet must, in the absence of a screening test, be given to all prospective donors.[978] Dr Brian McClelland’s revised draft was considered at the SNBTS directors’ meeting on 13 March 1984, which recorded agreement that a leaflet should be sent once to each blood donor as an enclosure with the call-up letter; directors undertook to send Dr Brian McClelland comments on the draft within two weeks. The minutes noted that “While the leaflet had been mailed to all blood donors in some English Transfusion Regions, in Scotland it had been made available at donor sessions and at some STD [sexually transmitted disease] clinics and the Scottish Directors felt their position would be strengthened by mailing to all blood donors.”[979]
Further comments (in addition to those received since the last meeting) on Dr Brian McClelland’s draft leaflet were made at the SNBTS directors’ meeting on 12 June 1984 and it was finalised.[980]
In Scotland, whilst the text of the revised SNBTS leaflet had been agreed, it appears that the leaflets had not yet been ordered as at 20 November 1984. It was, however, decided that each Scottish RTC would incorporate into their health questionnaire the words: “I have read the SNBTS AIDS leaflet (Important Message to Blood Donors) and confirm that, to the best of my knowledge, I am not in one of the defined transfusion-related risk groups.” It was also agreed that the leaflet must be distributed: with the call-up letter; at sessions to every donor who attended; to the organisers of workplace and college/university sessions; with the registration book to new donors; and (after donation) to the home address of donors who, not having been called to a session, attended nonetheless. The overall aim was that “as many donors as possible should have seen the message before attending a session.”[981]
Dr Brian McClelland told the other SNBTS directors at their meeting on 11 December 1984 about a leaflet from the Terrence Higgins Trust with a “clear explanation” and said it might be necessary to redraft the SNBTS leaflet again.[982]
The SNBTS’s Co-ordinating Group met on 19 February 1985. Dr Brian McClelland was proposing to amend the item he had added to the health questionnaire to read: “If you think there is any reason why your blood should NOT be used for transfusion, please tick this box and you will not be questioned further”, which he intended to run on a trial basis for two weeks.[983] It was agreed to await his experience. He was also now intending to mail all donors; Dr Whitrow expected to do the same but Dr Mitchell “repeated the impossibility in his region of writing to every donor.”[984] At the SNBTS directors’ meeting on 27 February 1985 it was agreed that the leaflets should be mailed to all active donors “wherever possible”, although it was recognised that some centres might have great difficulty in achieving it.[985]
At the meeting of RTDs on 9 July 1986 Dr Smithies asked RTDs to consider “again” the effectiveness of measures to exclude high-risk donors, in particular an arrangement which would allow donors who had reached a point in the sessional procedure where it was impossible for them to withdraw without embarrassment, to sign their blood away for research or some other purpose. The minutes record the following contributions in response: “Dr Harrison pointed out that staff would be very reluctant to bleed such donors. Dr Hewitt argued that such donors will give blood anyway and that the risk to the staff is therefore no greater than what exists at the moment. It was felt that to designate such donations for ‘research’ might encourage donors from high risk groups to attend and donate.” No specific action appears to have been agreed. There was also discussion of the latest iteration of the AIDS leaflet.[986]
EAGA acknowledged at its September 1986 meeting that people in high-risk groups were still coming forward to donate blood.[987]
By October 1986 the revised (fourth) leaflet had been printed and distributed to RTCs, with the expectation that it be distributed with donor call-ups.[988]
In January 1987 the RTDs at their regular meeting agreed that those who had engaged in prostitution should be added to the list of risk groups on the next AIDS leaflet. Dr Smithies envisaged another reprint within four months, and it was agreed by Dr Smithies that RTDs could see and comment on the final draft of the next leaflet, “though Dr Smithies pointed out that final wording could be influenced by the publicity section at DHSS.”[989]
The April 1987 meeting of the Eastern Division of NBTS consultants reported that the North London RTC had a confidential unit exclusion form for the donor to complete so that a high-risk donation could be excluded. This was said to be working well but required additional staff. The RTC also excluded prostitutes (male and female) and their contacts. Both Cambridge and South London RTCs indicated that they would find this system difficult to introduce and relied on the self-exclusion of donors.[990]
The issue of allowing donors a means of opting out was raised by Dr Smithies again at the meeting of RTDs in April 1987. She reminded RTDs that the discussion at the previous meeting had concluded without examining the opportunity for donors to opt out at some point during the donation process. All divisional chairs reported that this had been discussed “and felt to be difficult, complicated and probably unworkable.” The draft of the new (fifth) AIDS leaflet was circulated with Dr Roger Moore asking for comments by the end of April.[991]
At EAGA’s May 1987 meeting, Dr Smithies reported that the last leaflet had been issued in September 1986 and that the time had come for a revision. She sought advice that the leaflet correctly stated all those at risk from AIDS who should not give blood. It was agreed that a further risk group (“people who know they are infected”) should be included.[992]
A further (fifth) version of the DHSS leaflet was printed for distribution in July 1987.[993]
The absence of a uniform approach is apparent from the evidence given to the Inquiry by RTDs across the UK.[994]
Dr Morris McClelland did not give any serious consideration to producing a leaflet for Belfast: he was aware that a national leaflet was in the pipeline and thought it was appropriate to follow the national approach.[995] Once the leaflet had been received (some time after 13 September 1983[996]), the method of distribution, until late 1984, was simply to display the leaflets at all sessions. In late 1984 the centre began to hand a leaflet to each individual donor, although it was noted that donors often had insufficient time in practice to read it properly before donating and a few had shown resentment. Dr Morris McClelland recognised the difficulty for any donor to exclude themselves at a donor session and the desirability of sending the leaflet to each donor with the call-up letter. This was not possible, as the centre used postcards and did not have the clerical capacity to send enclosed leaflets.[997] Northern Ireland was “quite a conservative society” and Dr Morris McClelland felt there might be some merit in a gradual approach to introducing the leaflet.[998] He thought an amended questionnaire with a question along the lines of “Have you read the AIDS leaflet?” might have been introduced in around 1985/1986.[999]
Dr Napier, the RTD for Cardiff, attended a Welsh Office meeting on 4 May 1983, at which the view was recorded that, given the very low reported incidence of AIDS in the UK, “we might be confident that we are not collecting potentially contaminated blood.”[1000] He was reported in the Western Mail as saying that no links between AIDS and blood transfusion had been proved, and that “we do not take blood from anyone who is harbouring any sort of infective problem, and prospective donors are always asked about their medical history.”[1001] Cardiff’s method of distribution was to make the leaflets available at sessions; the leaflets stayed within sessions and were reused.[1002] They did not have the facility to incorporate the leaflet with the postal call-up process. At a Welsh Office meeting with the Chief Medical Officer for Wales on 19 November 1984, it was acknowledged that it was “still thought unsafe to rely upon this [the leaflet] as the sole means of weeding out the homosexual population from amongst potential blood donors”and noted that “The matter of a more detailed questionnaire could usefully be pursued.”[1003] A question asking the potential donor whether they had read the AIDS leaflet was in use or about to be introduced as at December 1984.[1004] By January 1985, Cardiff’s arrangements were that a leaflet was placed on each chair in the waiting area, and all donors were asked to sign that they believed themselves medically fit and had read the leaflet.[1005]
Dr Wagstaff, at Trent, took the more proactive option once the leaflet was available in September 1983 of sending the leaflets out to donors with the call-up cards and handing them out at sessions. He thought the leaflets did have the effect of putting off high-risk donors.[1006] Dr Wagstaff did not know why it took so long for the second version of the leaflet to be produced, but did not give any active consideration to the introduction of additional measures in the Trent region in the meantime.[1007]
Dr Entwistle was aware from 1982 that the question of infection with the AIDS virus was associated with transmission via blood in some form.[1008] However at Oxford (and in common with most RTCs), in the period leading up to the production of the first AIDS leaflet in September 1983, no particular steps were in place, beyond the usual standard processes, to screen out high risk from AIDS donors.[1009] The leaflets were then made available on display at sessions but not sent out with the call-up cards. Dr Entwistle suggested this was “not the most appropriate way, not least because that would not cater for the walk-in donors.”[1010] As at March 1984 the Centre held a stock of 13,000 leaflets, had issued approximately 1,000, and had a “now negligible” rate of usage per month, meaning that donors were not picking up and removing the leaflets from where they were displayed.[1011]
In North London RTC a slightly different approach was taken. On 23 May 1983, shortly after the first meeting of RTDs to discuss AIDS, Dr Davies wrote to colleagues at the RTC anticipating that a pamphlet would soon be available but that in the meantime “there must be no questioning of donors about their private lives.”[1012] Once the national leaflet had been produced, it was made available at sessions: Dr Contreras told the Inquiry that it could not be sent with call-up cards because they were sent as postcards, and that the service did not have the staffing to give it individually to donors. Instead it was left on the chairs in the waiting area “the donor attendant said, well, some of them read it and some of them don’t.”[1013] However, in mid 1984 Dr Contreras and Dr Barbara visited the New York Blood Center to find out how they were dealing with high-risk donors, and learned that a self-exclusion questionnaire was used which the donor could answer in confidence in a cubicle. On their return they introduced a trial of a self-exclusion questionnaire in North London in July 1984.[1014] By October of that year, fed up with waiting for the revised leaflet to be produced by the DHSS, their existing leaflet had been overprinted so that the words “Practising homosexuals” replaced “having had many sexual partners”. They also produced their own additional leaflet titled “Some Reasons Why You Should Not Give Blood” which set out a list of reasons as to why someone should not give blood “but emphasising the AIDS risk.”[1015] North London was not, however, able to fully comply with the requirement in the DHSS circular issued with the second leaflet, which required that the revised leaflet be brought to the attention of each donor on an individual basis: the call-up system using postcards meant that the leaflet could not be sent out at the same time: “We educated our donor attendants and receptionists on handing the leaflet, but I cannot say with certainty that it was handed to every single donor, I’m afraid.”[1016] The confidential exclusion questionnaire that had been trialled in July 1984 was rolled out across North London’s remaining donor sessions by July 1985.[1017]
The blood services in the UK were slow – too slow – to react to the threat of AIDS. In the detail of the chapter, the starkness of the chronology may be lost. It is this.
The underlying context was that of a growing epidemic. AIDS was known about in 1981. It was largely in the US, but (as things which start in the US often do) it had reached the UK – the first reported death from AIDS in the UK came in December 1981. It had become well enough known about in the UK by mid 1982 to justify a charity to support its victims (the Terry Higgins Trust).[1018] It was thus generally to be appreciated that it was not a disease restricted purely to the US.
Against this background, on 16 July 1982 the blood services – in England and Wales – and the Government became aware that its cause might well be blood borne. The only defence against this immediately available was careful donor selection and donor screening.
It was not until 18 May 1983 that there was any discussion amongst the directors of the regional blood services which together formed the NBTS in England and Wales about AIDS and its implications for donor selection and screening.
It was not until 1 September 1983 that a leaflet was produced for a six-month trial period.
It was not until a further year and five months later (1 February 1985) that the initial leaflet was revised, because the first lacked sufficient strength: and it was recognised even before it was distributed as not going far enough. Yet it took until September 1985 for a further revision.
As for the blood service in Scotland, SNBTS was probably aware of the potential risks at much the same time in 1982. It was slightly behind England in discussing what best to do: its first recorded discussion was on 24 May 1983.
By contrast with England, though, in the West of Scotland questions were already being asked on the donor questionnaire; and for Edinburgh and the South East, Dr Brian McClelland had already prepared a draft letter aimed at deterring donors whose donations might be risky.
In December 1983 it was thought that a more active approach was acceptable, but it was not until 13 March 1984 that a revised draft was considered. It does not appear to have been circulated until later in the year or early the next.
Four features in particular may explain (but not excuse) this history of delay.
Firstly, Dr Brian McClelland’s sense – which is borne out by the narrative set out above – was that most transfusion personnel “took some time to realise the seriousness of this infection” and that there was “some reluctance in some quarters, including within the UK transfusion services to acknowledge the gravity of what was emerging.”[1019] He thought that there was a belief in the transfusion community, particularly those who were engaged with the donor and donation side of it, “that blood donors were a particularly worthy and meritorious population … the thought that they could, in any sense, in the public mind be linked with behaviour which was certainly subject of enormous prejudice … there was a deep-seated reluctance to accept that there was any kind of link”.[1020]
There was also overconfidence in the voluntary donor system as a protection against infection. It is not always easy to question cherished notions: and it was right to have confidence that a system of voluntary non-remunerated donors offering their blood was and would be safer than the alternatives. However, “safer” does not mean “safe”. A moment’s reflection might have told those in the transfusion system that the voluntary nature of donations had not prevented the transmission of hepatitis at any time since the services were set up in the 1940s and that the greatest safety that could be achieved in the absence of a totally reliable screening test depended on the selection of “good” donors, and the rejection of those who were a greater risk.
Secondly, there was the same confusion of incidence and risk as bedevilled clinical responses to AIDS. The fact that someone might think themself to be in good health because they are not symptomatic, does not mean that they are not a carrier for the disease in question. Where a disease has a long incubation period before it shows itself the appearance of symptoms may be too late. For instance, Dr Napier in Wales observed “we do not take blood from anyone who is harbouring any sort of infective problem”[1021] which relies on the appearance of symptoms, rather than the association of a donor with a risky cohort, as a result of which they may, unknown to them, be incubating an infection.
Thirdly, there was the lack of a “centralised approach by the UK Transfusion Services.”[1022] There were multiple forums in which issues were being raised – the meetings of the RTDs in England and Wales, the meetings of SNBTS directors in Scotland, the SNBTS Co-ordinating Group, the UK Working Party on Transfusion-Associated Hepatitis, the CBLA, the Advisory Committee to the NBTS, the Central Blood Laboratories Authority’s Working Group on AIDS – but no single body with responsibility (and resourcing) to “address the problems of AIDS in relation to transfusion in the UK.”[1023] The primary responsibility for this lies not with the blood services but with central government and is explored elsewhere in this Report,[1024] but the blood services could and should have addressed this by setting up (as they did in relation to hepatitis in September 1982) a UK-wide working group the sole focus of which could have been AIDS and the steps that could be taken to reduce the risk to transfusion recipients.
Fourthly, it is undoubtedly the case both that the DHSS wanted to take the lead and that, having done so, there were significant delays on its part. This no doubt made it more difficult for the blood services to have in place uniform and robust measures.
Nonetheless, it remains the case that – whatever the DHSS was (or was not) doing – it was incumbent upon the blood services to take whatever action could be identified to reduce the risks of AIDS transmission to transfusion recipients. They did not do so.
The failure on the part of the blood services to give any kind of collective consideration to what could be done prior to May 1983, when the matter was properly considered for the first time by the RTDs and by SNBTS, was wrong. It should have been obvious that testing was inevitably still some way off. Deterring or preventing those in high-risk groups from donating should therefore have been a priority. It was not treated as such.
Few centres took proactive steps in advance of receipt of the first AIDS leaflet in September 1983. That some centres (eg Birmingham, Edinburgh) did use leaflets of their own devising rather than simply wait for the DHSS means that all centres could (and should) have done so. Although the possibility of using posters was raised by more than one RTD,[1025] there is no evidence that this simple, but potentially effective, measure was implemented across the UK.[1026]
A much more active approach to distribution of the leaflets should have been adopted from the outset, so as to ensure that the information within the leaflets came to the attention of all donors. Distribution with the call-up cards was one measure which should have been more widely adopted.[1027] Another way was to provide the information directly to all donors at the sessions. Thus by January 1985 the South London Centre was providing “Dear Donor” letters to all donors, giving them time to read the letters and asking them to confirm that they had. The letter, from the RTD Dr Rogers, identified the high-risk groups and then continued with a personal plea:
“My message to those in the above groups is ‘FOR GOD’S SAKE DO NOT GIVE BLOOD TODAY – YOUR BLOOD MIGHT KILL SOMEBODY’. If you would rather we did not know that you are in a risk group then tell the nurse at the bed you think you may be developing a cold, a sore throat, or feel unwell TODAY – anything – BUT DON’T GIVE BLOOD … Your co-operation will be as important as actually giving blood and we thank you.”[1028]
Practical measures to ensure that all donors understood the risks and were helped to take the right course of action if they were in an at-risk group could have been implemented by all centres in 1983 but were not.
That centres could find a way of alerting donors to the risks is clear, because this is what centres were required to, and for the most part did, do following the ministerial circular in February 1985. Thus, for example, at Brentwood a system was instituted with effect from 1 February of handing the leaflet to each donor as they registered and telling them that it was “most important” to read the leaflet.[1029] In East Anglia, where previously the old leaflet had been made available on display at sessions, the routine was “stiffened up” so as to ensure that all donors were made aware of the contents of the new leaflet.[1030] In North London, the “Some Reasons Why You Should Not Give Blood” additional leaflet was devised to overcome the reluctance of donors to pick up and read a leaflet on AIDS.[1031]
On 4 January 1983 a meeting lasting eight hours in Atlanta brought together representatives of the National Hemophilia Foundation, American Red Cross, various blood bakers, the National Gay Task Force, some state health departments, the Pharmaceutical Manufacturers Association, the CDC, Food and Drug Administration (“FDA”) and National Institutes of Health (“NIH”). On occasions the argument grew heated: Dr Donald (Don) Francis of the CDC at one stage banged on the table, asking how many deaths there had to be before meaningful action was taken. The US Assistant Surgeon General circulated a summary report of the meeting afterwards which conveyed these differences in more measured terms: “A consensus was reached that it would be desirable to exclude high risk donors to reduce the risk of AIDS transmission via blood and blood products. However, no consensus was reached as to the best method of doing this.” It recorded that participants had: “differing perceptions of: 1. The likelihood that AIDS is caused by a transmissible agent; 2. The risk of AIDS from blood donation (both whole blood and pooled plasma); and 3. The best approach for establishing altered guidelines for blood donation, donor screening or testing and donor restriction.” He called at the end of this note for each public health agency to provide candidate sets of recommendations for the prevention of AIDS in patients with haemophilia and for the other recipients of blood and blood products to Dr Jeffrey Koplan, assistant director for Public Health Practice at the CDC, with a view to the agencies developing a uniform set of recommendations.[1032]
Dr Francis took up the invitation and replied, to Dr Koplan as asked, on 6 January 1983. The recommendations he made are worth repeating here in full. They show that the views this Inquiry has reached as to what might have been done are not simply a product of hindsight – a submission to the Inquiry being that hindsight should be avoided – but demonstrate that similar views were set out, prospectively, in clear terms by an expert in public health. He wrote:
“I think the following recommendations should be promulgated by CDC with hoped for, but not essential, agreement of FDA:
There is good evidence that this will eliminate over 3/4 of AIDS ‘infected’ donors. It will also defer about 5% of U.S. blood donors and add about $5 to each unit of blood and plasma. These seem to be small prices for preventing a serious disease and a potentially dangerous panic.
Only small pool (less than 100 donors) concentrate or cryoprecipitate be used on hemophiliacs starting immediately (after supplies become available). This recommendation should stand until either: 1) knowledge of AIDS permits more accurate recommendations or 2) plasma becomes available which has been collected using the previously stated donor deferral.
I understand that these recommendations will be controversial and that there will be objections by industry and blood bankers. I think we should get comments from these groups and should keep them informed of our to-be-published recommendations. However, to wait for their approval of our recommendations will only endanger the public’s health.”[1033]
This letter should make uncomfortable reading for those who were in decision-making roles in the UK in 1983 to 1985, including those in the blood services. The UK was in a position to learn from the US experience. It should not have regarded AIDS as a purely US problem, but rather one which was highly likely to spread to these shores: contact between UK and US citizens in person was frequent. The US experience was available to inform reactions in the UK. Though it is right to note that the US did not change the pool sizes it used, and it did not mandate the terms of the exclusions suggested by Dr Francis across the whole country, it shows what could and should have been under urgent consideration here. When this letter, with its clarity of recommendations and sense of urgency, is compared to the length of time spent in the UK refining the niceties of text for donor leaflets, and the sluggish nature of the initial response in the UK to the threat of AIDS, it is clear that the benefit of hindsight is not required to find the UK wanting, as I do.
Doing more, more quickly, would have saved some infections. Acting sufficiently, and promptly, was not just the responsibility of ministers, the DHSS and the SHHD, though it was in part theirs, as will be discussed later. It was also the responsibility of the blood services. Sadly, though some within the services did more, more quickly, this was not true overall: in general the blood services did too little, too late.
This chapter explores the system for the licensing of commercial factor concentrates and in particular whether the decisions to grant licences and thus permit the importation of these products in the 1970s exposed UK patients to unnecessary risks. It examines in detail the July 1983 decision of the Committee on Safety of Medicines not to prevent further imports and the failure to keep that decision under review. It also looks at the extent to which the Committee on Safety of Medicines discharged its function of communicating the risks of hepatitis or AIDS from blood products to healthcare professionals.
1970 First use of commercial concentrates in the UK on a named patient basis.
October 1972 inspection of Hyland by Dr Duncan Thomas on behalf of the DHSS.
10 January 1973 CSM advises the grant of a licence for Hemofil.
February 1973 CSM advises the grant of a licence for Kryobulin.
22 May 1975 licence granted for Profilate.
12 November 1975 CSM(B) advises the grant of a licence for Factorate.
9 December 1975 DHSS Divisional Management Group meeting following World in Action documentary Blood Money.
21 January 1976 Meeting with Dr Owen at which Factorate application is discussed.
22 January 1976 CSM advises the grant of a licence for Koate.
28 March 1978 Kryobulin licensed as red packs (European plasma) and cheaper blue packs (US plasma).
1983 - 1984 licences for heat-treated Hemofil and Factorate are refused.
24 March 1983 FDA recommendation of steps including avoiding use of high risk plasma in US blood products.
9 May 1983 paper from Dr Galbraith recommends suspending importation of US blood products.
13 July 1983 CSM(B) decides not to recommend action to stop continued importation of commercial concentrates; recommendation endorsed by CSM.
28 September 1983 confirmation that import of factor products made from higher risk pre-March plasma will continue.
22 November 1984 CSM requests Licensing Authority to invite early applications for licence variations to permit distribution and sale of heat treated concentrates.
Dr R D Andrews senior medical officer, DHSS
Professor Arthur Bloom chair,UKHCDO
Dr Leslie Keith Fowler medical assessor, Medicines Division, DHSS
Dr Spence Galbraith director, Communicable Disease Surveillance Centre
Dr John Holgate medical assessor, DHSS
Dr Joseph Smith CSM(B) chair
Dr Duncan Thomas senior medical officer on the secretariat of the CSM(B)
Dr Diana Walford DHSS senior and later principal medical officer, DHSS
CSM Committee on Safety of Medicines
CSM(B) Sub-Committee on Biological Products of the CSM
FDA Food and Drug Administration, US
This chapter explains the way in which the state controlled the supply of blood products manufactured abroad. After setting out the historical context, it considers (1) decisions to permit the importation and distribution of clotting factor concentrates made in the 1970s which exposed UK patients to unnecessary risks; (2) how a decision was taken in July 1983 not to ban further imports of factor concentrates, and whether this was flawed or appropriate; (3) similarly, whether the response to the importation into the UK (“dumping”) of factor concentrates which were manufactured from “riskier” plasma than that which was acceptable in the country of manufacture was sufficient and appropriate; and (4) whether any review of these decisions after mid 1983 was appropriate and if so when.
The first two of these decisions are of central importance in setting in train a series of events that led to widespread infections of hepatitis and HIV in people with bleeding disorders. Once the state considered the products sufficiently safe, all things considered, to be permitted access to the UK market, decisions as to whether to use them became dependent on a range of issues. These included convenience, finance, clinical preference and treatment policies, continuity of treatments, the “efficiencies” of production of NHS concentrates, and the way in which blood services were structured rather than placing a premium on the safety of the patient.
I have concluded from the facts available that the decisions in 1973 to license the importation of commercial factor concentrates were wrong on grounds of safety; that the decisions in 1976 to licence the importation of further factor concentrates paid insufficient attention to safety; that the decision of July 1983 was both wrong and flawed in the way it was reached; that in any event there is no evidence that the decision was kept under review as would have been appropriate; and that the approach to “dumping” was not justifiable.
It has been known for centuries that traders selling “medicinal products” may expose consumers to risk. As early as 1540 legislation protected them against the grosser malpractices of traders. This empowered physicians of London to appoint four inspectors of goods sold by apothecaries.
In the 19th century the Pharmaceutical Society of Great Britain was established, and legislation was introduced to control the retail supply of poisons. In 1858 statutory provision was made for the publication of the British Pharmacopoeia. The Sale of Food and Drugs Act 1875 [1034] helped control the adulteration of drugs. The regime did not yet extend to biological products, such as vaccines and sera, the quality of which could not be assayed by chemical analysis. This had to wait for the Therapeutic Substances Act of 1925 which provided for the licensing of, and control of the strength and quality of, a product. The Pharmacy and Poisons Act 1933, like later Acts dealing with antibiotics and certain other products, set out lists of medicines which could only be supplied on prescription.
Weaknesses in the system were exposed by the Thalidomide tragedy in the early 1960s. As a consequence, the need to see that drugs were safe to use and to ensure the protection of the public resulted in legislation being strengthened, ultimately by the passing of the Medicines Act which came into force in October 1968.[1035]
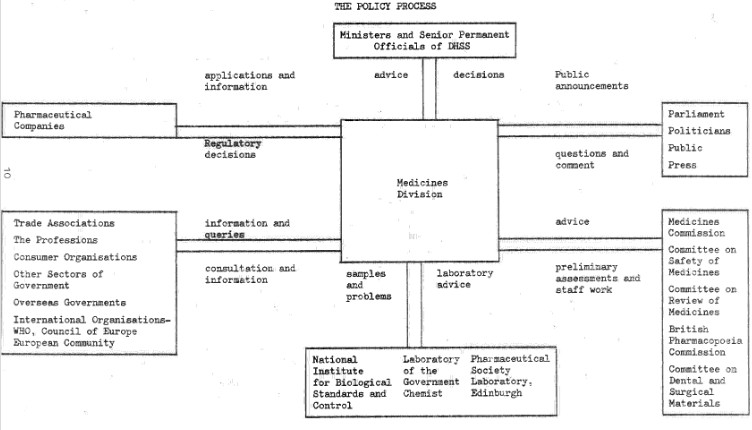
The Medicines Commission was established by the Act. Committees of independent experts were appointed by ministers on the advice of the Medicines Commission. One such committee was the Committee on Safety of Medicines (“CSM”), in effect a continuation of the former Committee on Safety of Drugs. Its role was to advise “the Licensing Authority” (the Secretaries of State for Health and Agriculture, together with the respective ministers for Health and Agriculture in Scotland, Wales and Northern Ireland, exercising their powers jointly). Its advice was concerned with the safety, quality and efficacy in respect of the human use of any substance or article to which any provision of the Medicines Act 1968 was applicable.
In practice, the advice of the CSM was accepted by the ministers who constituted the Licensing Authority at the time. Again, in practice, the functions of the Secretaries of State for Health of the UK as Licensing Authority under the Medicines Act 1968 were discharged on their behalf by the Medicines Division of the Department of Health and Social Security (“DHSS”) in London.[1037]
Dr Diana Walford, who began her work as a medical civil servant in 1976 by occupying a post in the Medicines Division, was asked in evidence what role the Medicines Division had in licensing. She had a clear recollection: “Oh, completely … it was manufacturing licences and product licences. That was their job.” She was asked about clinical trial certificates or clinical trial exemption certificates. She responded: “Well, it was Medicines Division. I mean, again, if somebody applied to the Medicines Division or the licensing authority, as they actually were deemed, for a clinical trial certificate or a clinical trial exemption certificate that was to be considered. It fell to be considered by Medicines Division, whether it needed to go entirely to a Committee on Safety of Medicines Meeting I think might have depended on the product.”[1038] In short, the Medicines Division was effectively in control of the process.
The CSM established a number of sub-committees. One of those was the Sub-Committee on Biological Products (“CSM(B)”). It worked on its own.[1039] The organisation of the sub-committees changed over time. However, there was always a sub-committee dealing with biologicals, and another dealing with adverse reactions.
When an application was made for a licence to distribute pharmaceutical products,[1040] it was considered in the first instance by the Medicines Division. A pharmacist and a doctor who worked for the Medicines Division would each assess the application, along with a toxicologist. The assessor(s) would produce a report. Where the reports related to blood products, they were usually submitted to the CSM(B). The CSM(B) in turn would consider the reports and formulate a recommendation. Its members would know the views of the Medicines Division staff, for their reports did not simply summarise any danger but expressed a view on it.[1041] The Sub-Committee considered the reports, then formulated their recommendations for the main Committee. That Committee’s role was advisory. Technically speaking, the CSM and CSM(B) advised the Licensing Authority, but in practice the Secretaries of State had delegated their decision-making powers to the Medicines Division. Thus the same body, the Medicines Division, two or three of whose assessors had first expressed their views in a report to the relevant Sub-Committee of the CSM, ultimately had to take a decision: a degree of circularity recognised by Professor Sir Michael Rawlins[1042] when he gave evidence.[1043] If the CSM felt unable to advise that a licence should be granted, it had to offer the applicant a chance to appear before it, or to make written representations. The same applied if it was thought that an existing licence should be revoked, suspended or varied. If the Committee still intended to advise against the grant of a licence, the applicant had a right of appeal to the Medicines Commission itself, and in some cases had the right to a further onward appeal.[1044]
Until Freedom of Information legislation came into force, the proceedings of the CSM (and the proceedings of its Sub-Committees) were kept confidential. The Medicines Division (which provided the secretariat) together with members of the Committee alone knew the reasons for the decisions made and what discussions there had actually been. For some time before the Freedom of Information Act 2000 the CSM had concerns about its secrecy of operation.[1045] It believed that disclosing the reasons underpinning its advice would have public health benefits. It would enable prescribers to understand more fully the reasons underlying dosage instructions, contraindications and warnings, and would enable those advising prescribers to offer a better service to their readers and clients. It would permit more informed decisions by NHS purchasers and providers. But the CSM, though believing this, had never itself pressed for openness and transparency in this way until the Freedom of Information legislation presented the opportunity. Commercially sensitive information, often included in an application, could remain confidential, and did: but it would have been in the public interest for other matters such as the risks posed by products and the extent of those risks to have been made known earlier than they were.[1046]
Given the passage of time since licensing decisions were made in the early and mid 1970s, the confidentiality which prevented detail of any discussion being known, and no one now being available from whom the Inquiry can seek an explanation, the evidence is incomplete at best. The quality of the decisions of the Licensing Authority to license blood products to be imported into and distributed within the UK, which were first taken in 1973, thus has to be assessed on the basis of evidence I wish had been fuller. Greater material is available concerning decisions in the early 1980s, but this too is still incomplete.
Two other bodies had some input into the decision-making processes of the CSM/CSM(B). These were the National Institute for Biological Standards and Control (“NIBSC”) and the Public Health Laboratory Service (“PHLS”). Neither had any formal role in respect of Scotland or Northern Ireland.
NIBSC began its work in 1972. As words in its full title (“Standards and Control”) suggest, it was not concerned directly with the criterion of safety: its remit was, and remains, concerned with controlling standards – the purity and potency of licensed biological products used in human medicine.[1047] Though these had some impact on safety, its primary focus (in terms of the three central statutory criteria which informed licensing) was on quality and efficacy.[1048] Its role in licensing was on an informal “on request” basis, if the formal advisory bodies – the CSM and CSM(B) – or Licensing Authority asked for it, in order to take advantage of individual scientific expertise.[1049] It had a more formal role in the control of biological products after licensing, such as when products were required under the terms of a licence to undergo a “batch release” process. This required manufacturers to submit to NIBSC, on a batch-to-batch basis, protocols describing the results of in-process tests made during the manufacture and, in most cases, samples[1050] of all such batches. If a batch failed this scrutiny that batch could not then be distributed in the UK – and for this reason an adverse decision was known as a “stop order”. Dr Trevor Barrowcliffe, who worked for NIBSC as a scientist and later senior scientist and head of haematology between 1974 and 2006, understood that all blood products had to undergo the “batch release” process as a condition of their being licensed.[1051] This did not however apply to unlicensed products supplied on a “named patient” basis.[1052]
The functions of NIBSC described above were provided for by statute after 1975, when the National Biological Standards Board was established.[1053] That board took over management of NIBSC.[1054] The relationship between NIBSC and CSM(B) was particularly close.[1055]
PHLS was responsible for providing a bacteriological service for the control of infectious diseases. It was thus more directly concerned with safety than was NIBSC, and less with quality and efficacy. Until more recent times, it operated 52 area and regional diagnostic laboratories in England and Wales, providing diagnostic services and support for outbreak investigation to local hospitals, public health authorities, and environmental health departments. Each laboratory provided surveillance data, and sent microbiological samples for reference testing to the central PHLS units at Colindale, and took part in national investigations into infectious diseases.[1056] It had an epidemiological arm, based at Colindale with a Welsh unit at Cardiff,[1057] which kept human disease under surveillance (the Communicable Disease Surveillance Centre (“CDSC”)), and a research facility at Porton Down, the Centre of Applied Microbiology and Research (“CAMR”).
The Medicines Act 1968 required the Licensing Authority to take into particular consideration the safety of the product (which needs no further definition),[1058] its efficacy (ie how well it did what it was intended to do) and its quality (its manufacture in accordance with the specified method of manufacture, and the quality control which was exercised over this).[1059] The Licensing Authority was to disregard any question whether medicinal products of another description would or might be equally or more effective,[1060] but it was expressly provided that this did not apply when considering safety. In short, the Act itself permitted the Licensing Authority in deciding whether to recommend the grant of a licence to consider whether another product, even if equally or more efficacious, might be safer.
Every medicine is likely to have or carry a risk of side-effects. Some of those side-effects may be more severe than others. The fact that side-effects are caused by taking a medicine does not mean it is necessarily unsafe. As Professor Sir Michael Rawlins said, “safety is a balancing act between … what is being used to treat and what the adverse effects are. So if you’re treating some lethal condition, then you’re prepared to put up with more adverse reactions, perhaps, than something relatively mild. So it was a judgment of balancing safety and efficacy.”[1061]
The extent to which regard was had to licensing in other jurisdictions is not easy to determine. Professor Sir Michael Rawlins’ comments on the degree of weight given to licensing decisions in the US are particularly revealing. Asked “if something had gone through FDA[1062] approval, did that carry particular weight?” he replied: “Yes, it would indicate that a relatively strict licensing body had found it was appropriate.”[1063] He added “if a product had already been on the market in the United States [there] might be more information on what had happened once it had gone on the market, about safety in particular.” This shows his general view of the rigour of the FDA: that it was “relatively strict”. This view does not sit easily with much of the material about the FDA considered nearly 30 years ago in the Krever Inquiry into contaminated blood in Canada. The report of the Krever Inquiry found gaps in protection: for instance, licences were not required and nor were inspections conducted by the FDA for most of the US blood centres that sold recovered plasma to fractionators. Thus commercial concentrates manufactured in the US were likely to contain material which came from sources which had neither been licensed nor inspected. When viral inactivation methods were claimed by manufacturers, “Neither the Food and Drug Administration in the United States nor the Department of Health and Social Security in the United Kingdom performed these studies. They were done by the pharmaceutical manufacturers themselves as part of the research and development involved in the manufacture and marketing of new drugs.”[1064]
A somewhat less favourable view than Professor Sir Michael Rawlins took of the rigour of the FDA’s processes was expressed by Dr Duncan Thomas. He was a senior medical officer on the secretariat of the CSM(B) between 1971 and 1974 (therefore during a period when the first licences for commercial distribution of Factor 8 were granted) and as such had a role in advising the CSM(B) whether it should recommend granting a licence.[1065] In his evidence he said:
“We would liaise closely with the FDA but this was not a rubber-stamping exercise. We still checked every application carefully and we would not be influenced or swayed by licensing within another jurisdiction. From my perspective, I recall that occasionally we were reluctant to accept evidence from the Americans where they said a product had already been licensed for a few years without causing problems and that we should take this into account. We would look at all the evidence carefully but we were not influenced by other jurisdictions’ licensing processes or decisions.”[1066]
Over 20 years after the first blood products were licensed for distribution in the UK, a committee to study HIV transmission through blood and blood products was set up in the US by the Institute of Medicine at the request of the Secretary of Health and Human Services. A number of the leading experts in various disciplines throughout the country undertook a two-year study and reported in July 1995.[1067] Their report was critical of the FDA in the way it had managed regulation of blood and blood products in the early 1980s, in particular finding that it had failed to take a proactive approach to regulation and had relied too heavily on the pharmaceutical industry. It noted that there was evidence that the agency did not adequately use its regulatory authority.[1068] The FDA had a blood products advisory committee which, though it contained members drawn from a variety of scientific disciplines, in the 1980s had a substantial membership drawn from those involved in blood banks and fractionators – representatives of the very bodies that were potentially subject to regulation – despite what the Institute of Medicine committee seems to have regarded as a potential conflict of interests.[1069]
The best reconciliation of these differing perspectives is that Dr Thomas was reflecting the approach as he knew it best, largely informed by his experience in the early 1970s, whereas Professor Sir Michael Rawlins was speaking of the approach as it developed in the 1980s. Given what was suggested by the Institute of Medicine study it would have been a mistake to place any determinative weight on the views taken by the FDA and (in particular) to assume that because it approved or licensed plasmapheresis centres and manufacturing plants these facilities operated as safely as they were supposed to operate. There can be little doubt about the impressions which British sources had reached about the probable quality of plasmapheresis centres. As described below, in 1972 on behalf of the CSM(B) Dr Thomas himself had inspected a plasmapheresis centre operated by Hyland. He returned to the UK less than impressed by what he had seen; and some three years later in 1975 a Granada World in Action documentary[1070] (with significant input from a well-recognised expert, Dr Arie Zuckerman[1071]) highlighted the same troubling picture. The apparent fact that those concerns had persisted for some three years in the case of some Hyland facilities suggests that the criticisms expressed by the Krever Report and the Institute of Medicine study may have been well-founded: but, more pertinently, were there to be appreciated in the UK in the early to mid 1970s if not for longer.
A licence was not required before a blood product could lawfully be sold in the UK in just two particular circumstances. First, a clinician could obtain supply of an unlicensed product on a “named patient basis”.[1072] The supply was intended for such treatment of a particular patient as their clinician thought was required.[1073] In such a case, if it were later proved that the product unreasonably did harm to the patient, the prescribing doctor could in theory be required to answer for their use of unlicensed products either in response to a complaint to the General Medical Council or in a legal action against the doctor under the law of negligence. Though neither was very likely to occur, it would be wrong nonetheless to say that there was no form of regulatory control which might have been exercised over its prescription simply because the CSM did not provide it.[1074]
Second, a clinical trial exemption certificate might be applied for.[1075] This had the useful function of allowing products to be tested in use for human therapy, usually in anticipation that if the trial endorsed the benefits anticipated by the manufacturer an application to license the treatment would follow. Again, there was in principle a degree of regulatory control over this: ethical approval to conduct a trial would be required, and be subject to the local ethical committee’s decision; those people receiving treatment in the trial were meant to be told that it was a trial treatment, what its purpose was, what the potential downsides and advantages were, and (latterly) the manufacturer might be required, as a condition of the grant of exemption, to offer compensation to anyone who suffered unanticipated harm as a result of the treatment.
The first use of commercially produced concentrate in the UK appears to have been under one of these exemptions. In 1970, Kryobulin was first used in the UK.[1076] By 1972, improved factor concentrates became available, and clinicians began to use them more. They were not yet licensed. The named patient exemption permitted their use.
No doubt because the demand increased as a result of these initial supplies, both the makers of Kryobulin (through their UK-based company Serological Products Ltd[1077]) and of Hemofil (made by Hyland, based in California[1078]) applied in 1972 for licences to permit distribution more widely in the UK.
For each application, Dr Thomas provided a report of his assessment to the Sub-Committee, containing his recommendation. Although his recommendation did not have to be accepted, since the Sub-Committee was itself composed of experts formed from different disciplines (including haematology) and could reach its own independent conclusions, it would in general accept the recommendation of its assessor, and that would in turn be accepted by the CSM itself. However, Dr Thomas observed that “licences were often given with conditions which demonstrated the CSM spotted deficiencies and assured they were rectified before the product was released on the market.”[1079]
On 24 October 1972 Dr Thomas inspected manufacturing facilities of Hyland in California, preparatory to reporting to the CSM(B) on its application relating to Hemofil. He also inspected a blood bank in Los Angeles which was owned and operated by Hyland and supplied plasma to them. In his summary report he noted that there was a hepatitis hazard associated with the products Hyland manufactured, as a result of two things: the nature of the donors (who “do not inspire confidence”[1080]) and the “very large plasma pools”.[1081] He noted that “the firm make no attempt to disguise this potential hazard.”[1082] Indeed all bottles of Hemofil stated “the risk of transmitting hepatitis is present. No warranties are made or created. Warranties of fitness or merchantability are excluded”.[1083] According to Dr Tom Cleghorn[1084] (speaking to an investigative journalist, Michael Gillard, in October 1975), Hyland said that all their plasma was by then collected from the US mainland and was individually tested for Hepatitis B antigen by radioimmunoassay (“RIA”), but also admitted[1085] that plasma to manufacture initial supplies of Hemofil for the UK had not been individually RIA tested and had come from Puerto Rico, where they had a blood bank.[1086] It may be assumed that, if so, the CSM(B) was unaware of this and should have been told.
In his medical comment[1087] Dr Thomas wrote that Factor 8:
“represents a major advance in the care of patients with classical haemophilia. Such concentrates have enabled corrective orthopaedic procedures to be carried out, and for the first time there is a prospect of domiciliary treatment.[1088] The major disadvantage of currently available commercial preparations, such as HEMOFIL, is that they are prepared from very large plasma pools, and carry the risk of transmitting hepatitis virus … no attempt is made to disguise the risk of hepatitis, and it may be considered that the decision to use this material could be left to the individual clinician who can balance the potential hazard against the anticipated therapeutic benefit to the patient.”[1089]
It was on that basis that he assessed that the grant of a licence should be recommended.
CSM(B) recommended the grant of a product licence for Hemofil at its meeting on 10 January 1973. The minutes do not reveal any discussion regarding hepatitis risks.[1090] Given that Dr Thomas had drawn attention to these risks, specifically, and they were openly admitted in the application, this is surprising. The CSM accepted the recommendation from its Sub-Committee, and advised the grant of a product licence at its meeting on 25 January 1973. Though the practice was generally to accept recommendations from its specialist Sub-Committees, again no discussion regarding hepatitis risks is recorded in the minutes.[1091]
In respect of Serological Products Ltd’s application for a licence for Kryobulin, Dr Thomas reported that all donors were tested at each donation and any donor who had a history of pathological transaminase, or a positive hepatitis-associated antigen level, was permanently excluded from the donor programme. Despite these precautions, he commented that “the risk of transmission of serum hepatitis can only be diminished and not completely eliminated.” The manufacturers themselves made no secret of this. Dr Thomas reported that it was prepared by “large scale fractionation” obtained from plasma pools of 1,000 donors. The information from Serological Products Ltd was that the donors came from Austria and Germany. There was no suggestion that the donors were volunteers.[1092]
Dr Thomas observed that the factory had not been visited recently and that the Sub-Committee “may consider that the Austrian Authorities should be requested to carry out an inspection.”[1093] The CSM(B) considered the application, and Dr Thomas’ report, at its meeting on 10 January 1973. The minutes record that “The Sub-Committee was informed that the manufacturer of Kryobulin PL/0215/0003 had not been visited recently, but the licensing authority intended to ask the Austrian authorities to carry out an inspection on its behalf.”[1094] It is unclear from the minutes why the CSM(B) recommended the grant of the product licence without waiting for the inspection to take place and considering its findings.[1095]
The recommendation of the Sub-Committee was put before the CSM at the meeting in February 1973 and CSM advised that the product licence should be granted, which it was in March 1973.[1096] It was not until May 1973 that Austrian inspectors conducted an inspection of the manufacturing facilities,[1097] followed by an informal visit by the DHSS the following month.[1098] But Kryobulin was not actually marketed in the UK until July[1099] – and it is therefore to be assumed that the inspections proved satisfactory – satisfactory, that is, in the eyes of the inspectors: for when he spoke in September 1975 to Michael Gillard who was researching sources who could assist in his production of a factual report for Granada,[1100] Professor Zuckerman told him that he had visited Immuno in Vienna, and thought it a poor facility, which lacked medical back-up and had “dubious sources of plasma”.[1101]
No reference was made in either of the reports produced by Dr Thomas, or in the minutes of the CSM(B) or CSM, about contemporary understanding of the relative safety of commercial products such as Kryobulin and Hemofil when compared with domestically produced concentrates or with cryoprecipitate. It is a feature of this understanding which may cause some puzzlement: why was it that the licence applications were not rejected on safety grounds?
Though some of the relevant material is discussed elsewhere in this Report, it is convenient to draw it together here in order to place the licensing decisions in respect of Hemofil and Kryobulin in context.
First, in October 1970 Bio Products Laboratory (“BPL”) began to screen blood products for Hepatitis B antigen: by November 1971 all plasma received at BPL was screened.[1102] The tests then performed were imprecise.[1103] More sensitive screening tests[1104] only began to be used in 1975, and even they did not “catch” all infections by Hepatitis B. It seems likely that similar tests were being adopted in the US as well as in Austria (and less certainly in those places from which plasma was sourced for production in Vienna). Batch testing would form a further line of defence albeit using a similar, imperfect, screening test. Although at the start of the 1970s many (perhaps most) will have assumed that post-transfusion hepatitis was caused by one virus, rather than by two major ones as turned out to be the case,[1105] there were early, authoritative indications that this might not be the case. Professor Joseph Garrott Allen wrote in 1970 that “it appears that at least two immunologically separate agents are capable of producing hepatitis from the transfusion of blood or the administration of many of its products”, and cited the work of Dr Saul Krugman in support.[1106] However, the risk of contamination of the blood used to make the products would be reduced by the testing available for one of those agents, and within the near future was likely to be reduced further as tests improved.
There were growing concerns about the source material (the blood and plasma) from which commercial products were made. It was considered that the risk of causing hepatitis from blood taken from paid donors was markedly higher than that of blood from unpaid donors: not only had Professor Garrott Allen said as much in “Commercially Obtained Blood and Serum Hepatitis”[1107] but researchers at the US National Institutes of Health had found the same.[1108] Richard Titmuss had published his influential work The Gift Relationship in February 1970 to the same effect so far as risk was concerned.[1109] It was known by fractionators that the plasma used to make factor concentrates carried a risk of transmitting hepatitis, patients contracting it, suffering serious liver disease and dying.
Alter et al[1110] and Grady et al[1111] (both published in 1972) showed that the hepatitis risk from commercial blood was markedly higher than that of blood from unpaid donors, but also that even after excluding Hepatitis B Ag positive donors, much post-transfusion hepatitis remained.
Professor Garrott Allen repeated his earlier message in The Epidemiology of Posttransfusion Hepatitis – Basic Blood and Plasma Tabulations in 1972.[1112]
In early 1972 President Richard Nixon delivered a Special Message to Congress on Health Care, calling for “a safe, fast and efficient blood collection and distribution system”. Hospital Week reported this, stating that authorities in the field regarded the present system as inadequate, pointing out that hospitals in many cases were forced to buy blood from commercial blood banks “which often accept blood from such donors as derelicts and drug addicts who may be the transmitters of such diseases as hepatitis, syphilis and malaria. A study made two years ago indicated that 30,000 Americans contract hepatitis each year through transfusions of contaminated blood with 1,500 of them dying from the effects of the diseases.”[1113] The message was clear that blood from paid donors was riskier than that from volunteer donors.
Importantly, insofar as the CSM(B) and CSM wished to consider whether another, safer product might be readily available to treat patients, leading luminaries in the field of clinical haemophilia therapy in the UK, Dr Rosemary Biggs and Dr Katharine Dormandy, in an international forum reported in Vox Sanguinis 1972[1114] clearly assessed that patients with haemophilia could be adequately maintained with the use of cryoprecipitate. A number of the contributors to the forum observed that major surgery, emergency surgery and even prophylaxis could be achieved by using it. A major advantage of cryoprecipitate was seen to be a lower risk of hepatitis. The reported discussion tended to suggest that Factor 8 would be superior to cryoprecipitate only when this hepatitis risk was addressed.
This was not the view of a select few in isolation. The forum was international in its perspective. Nor was it simply the view of an international symposium. Within the UK itself Dr Peter Jones had written to say “cryoprecipitate is now the product of choice in major surgery, allowing the potent but antigenic animal fractions and expensive human concentrate to be reserved for major complications, the emergency treatment of patients with FVIII inhibitors, or, in the case of concentrate, for prophylaxis.”[1115] He regarded cryoprecipitate as responsible for a remarkable change in life expectancy of those with haemophilia. In the US, Dr Carol Kasper and Shelly Kipnis published in the prestigious Journal of the American Medical Association in mid 1972. They concluded that, for older children and adults who had had little exposure to blood products, especially those with mild haemophilia, “single donor products are preferable.”[1116]
Articles such as these reflected a high level of concern amongst a range of different clinicians and researchers, many of whom were established leaders in their field, that the risks of hepatitis (which were serious) were increased considerably where donors were paid and where large pools were used for manufacture.
Another aspect of the context at this time is that haemophilia centre directors were aware that larger pools theoretically came with a greater risk of causing “clinical” hepatitis.[1117]
It is impossible to know if, and if so how far, material such as this was discussed in the CSM when it came to make its licensing decisions about the safety of Hemofil and Kryobulin. Dr Thomas’ reports make no specific reference to any of these or similar sources, but knowledge of their thrust may have been assumed by him without the need to spell it out, since he did express concern about the risks posed both by the donors and the size of pools used in manufacture. There is however no reference in Dr Thomas’ reports to the ready availability of cryoprecipitate which, as the clinical views of the time establish, was regarded by many as the product of choice, except for major surgery and where inhibitors had developed in the patient.[1118]
Although Professor Sir Michael Rawlins spoke of the balance which it is necessary to strike between risks posed by products, on the one hand, and the advantages they bring through treatment of a difficult condition on the other, it would seem that the opinions reflected in the extracts quoted above would show that the general view was that cryoprecipitate ensured a treatment which was safer than that offered by commercial concentrates. This was notwithstanding that commercial concentrates did have significant advantages over cryoprecipitates in terms of convenience of administration, increasing the quantity of clotting factor which could be administered without causing circulatory overload, giving a lower risk of creating inhibitors, making it easier to determine whether a given dose would be sufficient or not, facilitating home treatment without the need for storage at very low temperatures, and allowing high-dose regimes to manage inhibitors. These are significant advantages, especially in respect of convenience of use, but on analysis they have only a limited effect on safety.
The opinions would also suggest that NHS concentrates of the time were safer. This was for two reasons. First, they were made from very much smaller pools. Second, the donor population was voluntary. So far as was thought at the time, the general population from which these donors came was one in which the prevalence of serum hepatitis was less than that of the populations in the US from which paid donors came. These features were most probably known to members of the CSM(B). However, no reference is made in the papers to the fact that NHS concentrates were available (though it seems likely this was known to the CSM(B)) even if supply was limited. There is no sign that these virtues of NHS concentrates were discussed in the course of any examination of the relative safety of commercial as contrasted with NHS product; indeed there is no evidence that there was such an examination at all. Dr Thomas saw two features as giving rise to a particular concern about the risk of hepatitis, an infection and illness which he would have known could be serious: pool size, and paid donations. The first of these two particular concerns, both of which he expressed in the case of Hemofil, did not apply with the same force to the NHS product, made as it was from smaller pools; the second did not apply at all. If it was not actually clear, it should certainly have been clear from the information available at the time that NHS concentrate was thought to give rise to a lower risk of hepatitis.
What does not feature in Dr Thomas’ reports or in the decisions of the CSM(B) or CSM is another aspect of the context. Although some 80% of the supply of clotting factor replacements came in the form of cryoprecipitate, and in 1973 (viewed overall, and thus including a period of time after the licensing decisions had been made to permit importation for general distribution to haemophilia centres) the balance of 20% was in the form of factor concentrates, split roughly half-and-half between NHS and commercial products, there was an increasing demand from clinicians for a greater availability of concentrate, especially where it was freeze-dried.[1119] At the end of 1972, Professor Edward Blackburn[1120] wrote on behalf of haemophilia centre directors to the Chief Medical Officer (“CMO”).[1121] He said: “The Directors feel that there is an urgent need to increase supplies of Factor VIII Concentrate, in particular of the freezedried [sic] concentrate. Many feel that if a British preparation cannot be made available very shortly, the commercial preparations should be bought.”[1122] Though Dr William d’A Maycock’s view was that self-sufficiency should be the aim “at present insufficient freeze dried antihaemophilic globulin concentrate is made in the UK. There is thus considerable pressure from those who treat haemophiliacs for foreign commercial material to be bought. There is indeed, at present, the need to supplement the existing UK supply but the facilities for larger scale fractionation that will become available in England and Scotland should eliminate the need to use foreign commercial preparations or go a long way towards doing so.”[1123] There was thus a general sense among many clinicians that more freeze-dried concentrate should be available; that NHS-produced concentrate was preferable; but that any need to supplement supplies by importing foreign-made products, rather than, or alongside with, augmenting supplies of cryoprecipitate, should[1124] be short-lived. There is no means now of knowing whether this was in the mind of the CSM(B): however, it can be noted that if it was it fell far short of reflecting any sense that there was a crisis of supply which was imperilling the lives of patients.[1125]
Indeed, the fact that it was (not unreasonably) thought at the time that the need for any importation would be short-lived makes it all the more puzzling that in the interim period between importation and the expected early date when sufficient concentrate would be available from domestic sources, a population of patients should be exposed to a risk when taking it was not critical to their health, and those who wished (after consultation with their treating doctors[1126]) to run that risk could take advantage of the named patient exemption.
After the first two products (Hemofil and Kryobulin) had been licensed, the DHSS opened a “call-off” contract with Serological Products Ltd and Travenol Laboratories Ltd for the supply of up to five million international units of each product to haemophilia centres.[1127] Not only was this set at half the quantity that had initially been anticipated[1128] but in the first full year demand for the product was “disappointing”. Only 47% of the allocation of Hemofil[1129] was taken up; and a mere 8% of Kryobulin.[1130]
The licensing of Hemofil and Kryobulin was followed by that of Profilate in May 1975.[1131] The plasma used for Profilate was said to have been tested by RIA, a more sensitive test for the presence of Hepatitis B than the electrophoresis tests used in respect of Hemofil[1132] and Kryobulin, but one which still led the manufacturer to acknowledge there might be some risk of hepatitis.[1133] The medical assessor made no separate reference to this risk, but noted that there had been no inspection of the manufacturing facilities.[1134] A list of the centres from which plasma came was provided by the manufacturer. The centres were operated by two different companies. Yet nothing is said in the report about the approach of either to the selection of donors or their rejection rate.[1135] Nor does there seem to have been an inspection made of any of the donor centres on behalf of the CSM(B) before the decision to grant a licence subject to conditions.
However, there is nothing to suggest that the product, though it came with risk, was any less safe than Hemofil or Kryobulin.[1136] If licences had been refused for those two products on the grounds of safety, no doubt a more rigorous examination would have occurred in the case of Profilate; but once the decisions in 1973 were made as they were, it is difficult to see how the CSM could recommend that a licence be refused for Profilate on the grounds of hepatitis risk. It would have been inconsistent with its previous decisions to do so, unless circumstances had changed sufficiently in the meantime. Furthermore, in 1974 there had been considerable pressure from haemophilia clinicians to increase the supply of factor concentrates. Their aim was that this demand should be fulfilled by NHS products (which were likely to be safer, and may well have been cheaper), but this was only likely to be achieved after a while. In the meantime, they sought an increase in the supplies of commercially produced concentrates.[1137]
The licensing of Koate was applied for in October 1975.[1138] Dr R D Andrews had noted in his assessment report[1139] that the plasma for the product was supplied from 54 different firms under various ownership, including US State prisons, and “suffers from being prepared from multi-centre donations which cannot be properly controlled by inspection.” He pointed, however, to his understanding that each donation was RIA tested for HBV antigen and there had been no reports attributing hepatitis to Koate since its introduction in the US in February 1974.[1140] The date of his report was 17 December 1975 – just after the second episode of the Granada World in Action documentary Blood Money concentrating in part on the poor quality of donors on the one hand, and the claims made that the quality of the screening process was poor on the other, where (presumably) FDA regulations were in force.
However, in his report, Dr Andrews said that in the past the CSM had recommended conditions, which included the number of donations and information about the rejection of donors or donations, centre by centre. In early January 1976, the CSM(B) recommended the grant of a licence. It was subject to conditions. In particular, it sought information about the pool size, and the reasons for and rate of donor rejection on a centre-by-centre basis.[1141] The latter requirement appears to have been in order to form a view as to how rigorous the screening process was. One in which very few donors, if any, were rejected, might give rise to concern. The information as to pool size would be supplied in February.[1142] None was given as to the rates of donor rejection.
The CSM considered the recommendation of its Sub-Committee on 22 January 1976. It confirmed it, including the condition as to information about the reasons for and rate of donor rejection.[1143]
On 2 February 1976, Dr Andrews wrote to Bayer UK Ltd[1144] to say that a licence for Koate would be granted subject to conditions.[1145]
Correspondence followed about those conditions. Bayer UK telexed Cutter in the US on 18 February about their acceptability. Five days later, Cutter responded. In answer to the proposed condition to require ongoing information as to the reasons for, and the rate of, rejection of donors or donations, centre by centre, Cutter said:
“We do not collect information of this nature. Such information would be of dubious value in evaluating a plasma derivative product’s safety or efficacy. In the manufacture of Koateᵀᴹ, all Source Plasma (Human) used as the starting material is collected and handled according to regulations described in Title 21 of the U.S. Code of Federal Regulations. Similarly, all plasmapheresis donors must be acceptable according to the criteria described in these regulations. All plasmapheresis centers from which our source material is obtained are licensed by the U.S. FDA. Thus, the FDA insures [sic] that all donors and units of Source Plasma (Human) are handled according to the regulations.”[1146]
The letter also objected to batches of Koate being subject to the batch release procedure. This was on the basis that each lot was subject to rigorous testing by both Cutter and by the US Bureau of Biologics before being released to distribution. Accordingly, any “additional routine testing would be redundant”. This, it would appear, was a similar objection to that which was made to the request for donor information. In effect, it was being said that in each case reliance could be placed on the existence of the regulatory regime in the US. To argue that was to argue against lessons of experience that had already been learned in the DHSS: as Dr John Holgate put it in May 1975 “It is one thing to have regulations and another to learn of the enthusiasm with which they are carried through.”[1147]
The Bayer UK/Cutter communication was forwarded to Dr Andrews on 4 March 1976.[1148] There followed a series of communications between Dr Andrews and Bayer UK. These concerned outstanding issues about the conditions, in particular the question of whether Cutter would submit to the batch release procedure. NIBSC, who would be due to conduct batch testing, told Dr Andrews that the licence should be refused unless Bayer UK/Cutter agreed that it should occur.
It is, however, important for what follows to understand why the batch release system was insisted upon by NIBSC. NIBSC said on 18 March 1976 that they would not agree to the licensing of a product unless there were batch release procedures because “Experience with all such products so far licenced has revealed deficiencies in proper formulation of information on protocols, as well as unacceptable assay biometry and methods.”[1149] In short, reliance could not necessarily be placed on all being done elsewhere as it was supposed to be done.
On 20 April, Bayer UK/Cutter pushed back on batch release for testing, arguing that it was sufficient to rely upon the work done by the US Bureau of Biologics.
NIBSC offered to explain the quality control difficulties to a representative of Bayer UK, if it “should wish to send someone to NIBSC Hampstead”.[1150] It did. In the event, Bayer UK capitulated (as it had to do if it were to be licensed).
The correspondence did not address any further question of the donor rejection rate. This is particularly surprising for two reasons. First, the apparent inability of Cutter to do that which the CSM(B) and CSM had both recommended, does not seem to have been substantively considered within the Medicines Division of the DHSS. Nor did the Medicines Division ask CSM(B) or CSM for further deliberation or recommendation on the point. Further, the DHSS continued to insist that there had to be a batch release process, and plainly did not think it satisfactory for Cutter to say that it would be sufficient for the UK licensing authorities to rely upon the fact that they might expect the regulatory authorities in the US to have given their approval. Nonetheless, they did not appear to insist in the same way on the observance of a condition as to donor rejections which both the CSM(B) and CSM had recommended.
Cutter then agreed with Speywood Laboratories Ltd that Speywood would import, sell and distribute Koate (and Konyne) on the UK market. Towards the end of August, Bayer UK withdrew its application for a product licence for Koate, since under the agreement it had reached with Speywood the importation and market would be solely in the hands of the latter. Accordingly, when the product licence was granted it was granted to Speywood. The licence contained no condition requiring the provision of ongoing data about donor rejections centre by centre, or at all.[1151]
In March 1975 an application was made for the importation and distribution of Factorate.[1152]
Dr Andrew’s report for the CSM(B)[1153] noted that there was a hepatitis risk associated with Factorate. He commented that it was not clear who supplied the donated plasma.
In November 1975, the CSM(B) recommended[1154] that a licence be granted, on similar conditions to those which Cutter had been asked to supply in respect of Koate, including information about the rate of rejection of donors, centre by centre, together with confirmation that the only plasma which would be used would be that from donor centres from the US or from other certified countries.
The importance of the proposed condition relating to the rate of rejection of donors or donations was emphasised by observations of Dr Holgate at a Divisional Management Group meeting in the DHSS on 9 December 1975. This was the day after the screening of the second part of Granada’s Blood Money documentary.
The meeting considered the criticisms which the World in Action documentary had made of Travenol’s production of Factor 8 in the US. The minute of the discussion continues:
“The criticisms were in conformity with an inspection report carried out on behalf of the Division. The Minister of State had been briefed and was concerned about the supply of the Factor and about the hazards of using it. A similar product manufactured by Armour had recently been cleared by the CSM; [this is obviously a reference to Factorate] Supply Division were anxious that it should be licensed as it would be available at a lower price than the Travenol product. There was some doubt as to whether the collection of blood products for either product was satisfactory. Dr Holgate said that he doubted whether inspection of the American collecting centres would be useful. What was needed was to strengthen the requirements in the product licence, and to insist on returns from each collecting centre including the rate of rejection of donors or donations.”[1155]
The reference to there being doubt as to whether the collection of blood was satisfactory can relate only to safety. By contrast, being “anxious” to license the product relates only to price. This shows that there was a pressure to license not because a product was safer, but because it was cheaper.[1156] It is not clear why a product which might be unsafe was to be licensed and what is of particular note is Dr Holgate’s observation that the DHSS should “insist” on returns from each collecting centre including the rate of rejection of donors.
The potential lack of safety is emphasised by the two following sentences from the discussion: “Dr Holgate said that doctors would prefer the British products as being safer. Indeed, once a pure supply is available, doctors will want to use the product in situations in which the currently available Factors would be too great a risk.”[1157] Importation of commercial concentrate was thus being licensed when the DHSS believed it to be less safe than UK products.
The Granada programme led to a meeting at which the Minister of State for Health, Dr David Owen, was present. He asked to see any further applications for product licences to authorise the importation of Factor 8. Accordingly, a submission was prepared for him regarding the application from Armour. A related minute echoed the theme of cost addressed in the December meeting, saying: “I understand that Supply Division have received a ‘very favourable’ tender from the company for the supply of Factor VIII to haemophilia centres but, of course, action on this depends upon the granting of a product licence.”[1158] The author was part of the Medicines branch of the Medicines Division.[1159] The Medicines Division was, according to Dr Walford, effectively the Licensing Authority.[1160]
It is difficult to avoid an inference that at this time cost pressures were playing a role they should never have been permitted to play in licensing decisions. That inference is strengthened by the facts discussed in the next two paragraphs.
The submission itself contained the assessment that inspections were limited in their usefulness and it “seems best to assume that all blood products of this nature coming from the USA may be obtained from plasma taken under the worst circumstances and any protective measures should be achieved by other means.”[1161] Those means are not spelt out: but it is clear that civil servants considered that the sources of plasma were likely to give rise to a significant risk that the plasma itself would contain infections.
The submission was preparatory to a meeting on 21 January 1976 where the Factorate application was expressly considered by Dr Owen.[1162] The “worst case scenario” assumed by the submission resulted in additional conditions being proposed. One of those conditíons was that “plasma will be obtained only from donor centres in the USA or in other countries specified in respect of which the licensing authority is satisfied as to the donation arrangements, being premises in respect of which you provide an undertaking that they may be inspected by or on behalf of the United Kingdom licensing authority.”[1163] Armour’s reply did not contain any such undertaking. It did say “We confirm that the plasma will be only from donor centres in the USA, and from USA sources.” It also responded regarding the rate of rejection of donors centre by centre by simply saying “the rejection rate at blood collection centres is below 1% for accepted donors.”[1164]
These responses leave a lot unsaid:
There is no evidence that the Licensing Authority took any further steps to clarify these matters, as might be available if they did. If, as I infer from the lack of evidence, they did not press Armour further, then given the assumption of the “worst case scenario” and the knowledge, as it had become, that collection of plasma in the US invited rather than assuaged risks of infection, this was a failure of regulation.
It is when these decisions as to the licensing of Koate and Factorate are viewed in context that the need for a clear understanding of the reasoning of the CSM(B) as to safety becomes clear. No material is now available to tell the Inquiry what it was. Arguably, however, circumstances had by now developed further from the times when licences were granted in respect of Hemofil, Kryobulin, and Profilate. 1975 in particular was a year in which concerns about the transmission of hepatitis by imported blood products mounted.
1975 started in the knowledge that in November 1974 there had been an outbreak of hepatitis amongst people with haemophilia in Bournemouth.[1165] This came under the spotlight. Of the 11 cases reported as constituting the outbreak, 7 had hepatitis which was neither Hepatitis A nor Hepatitis B. Dr John Craske spoke about this to the UK Haemophilia Centre Directors’ Organisation (“UKHCDO”).[1166] It is reasonable to think that what he said to them was to the same effect as he later wrote in respect of the same episode in The Lancet for August 1975.[1167] There he drew the attention of a wider audience than leading haemophilia clinicians to his concerns that commercial concentrates carried a much greater risk of transfusion hepatitis than did cryoprecipitate. He argued that their use should be reserved for life-threatening bleeds, and major operations. (If so, this is open to the comment that the use of NHS concentrates would have provided lesser risks than commercial concentrates, and if reserved for such incidents it is likely there would have been no shortage).
At the turn of the year from 1974 to 1975 therefore, hepatitis transmitted by commercial concentrate had become an issue of some momentum, at least amongst those treating haemophilia patients.
Then, in January 1975, Dr Owen expressed his belief that it was vitally important that the NHS should become self-sufficient as soon as practicable in the production of Factor 8 including AHG (antihemophilic globulin) concentrate: “This will stop us being dependent on imports and make the best-known[1168] treatment more readily available to people suffering from haemophilia.”[1169]
Also in January 1975, Professor Garrott Allen (from Stanford University) wrote to Dr Maycock (since he was consultant advisor to the CMO).[1170] He expressed his concern about commercial blood products being purchased by Britain from the United States.[1171]
In August The Lancet article by Dr Craske about the Bournemouth outbreak was published. Hemofil was implicated.
Then on 1 December 1975 Granada screened its World in Action programme Blood Money – Part 1.[1172] This highlighted the risk of hepatitis sourced commercially from prisoners and “skid row” paid donors, and featured an investigation into the facilities of Hyland. Its findings were consistent with the description of those giving blood at such facilities given by Dr Thomas in 1972. It was followed by Part 2 a week later.[1173]
As noted above, this led to a rare ministerial intervention in the licensing process, and a request for more stringent conditions being made in respect of Factorate.
Reverend Alan Tanner, chair of the Haemophilia Society, also described how in 1975 he was invited to see Dr Owen and that he “spoke very forcibly to Dr David Owen to let him know that we were not prepared to accept the risk of hepatitis coming from the blood products issued from the United States.”[1174] The meeting can be dated to 11 December 1975. According to the Society, “Dr Owen stated that in 1977 we would be fully self-sufficient in concentrates. The whole question of commercial concentrates, plasmapheresis, the regional structure of the BTS [National Blood Transfusion Service], and other matters were fully discussed.”[1175]
The following month Dr John Cash wrote to the British Medical Journal: “There is no doubt that the import into the United Kingdom of factor VIII concentrates derived from external sources, however well screened for hepatitis viruses, represents an unequivocal pathway by which the level of a potentially lethal infection into the whole community is being deliberately increased.”[1176] Though Dr Cash was given to expressing himself in forcible terms his use of the word “deliberately” is striking. It must represent a view that those who were responsible for allowing the importation made a conscious choice to do so and, because they had the knowledge of what that choice was likely to lead to, were by that deliberate act knowingly facilitating its consequences. It may be that readers dismissed the expression as hyperbole; but at the least it indicates a strength of view amongst some of the professionals whose work related to the use of blood products about the (lack of) desirability of continued importation.
There is also evidence that the DHSS was indeed well aware of the dangers which the importation of commercial concentrates posed.[1177] The evidence for this comes from a sequence of letters in November and December 1975. Dr Theodore Cooper, US Assistant Secretary of Health, wrote to the UK CMO (then Dr Henry Yellowlees) following Granada’s production. He had been approached by Michael Gillard, the journalist investigating matters prior to the Granada broadcast, who had indicated that there was the feeling in the UK that the hepatitis warning in the leaflets accompanying antihemophilic factor concentrates was not strong enough. Dr Cooper commented: “We feel that the warning is quite direct and adequate; in fact, it is generally appreciated in the U.S. that every lot of this particular product is probably contaminated with hepatitis B virus.”[1178] Dr Sheila Waiter took on the task of responding to this. She noted that:
“while it is generally accepted that the benefits of having Hemofil available for the treatment of bleeding episodes far out-weigh the risk of acquiring hepatitis B nevertheless the statement that ‘every lot of this particular product is probably contaminated with hepatitis B virus’ will come as a surprise to many clinicians using the product, especially if the practice of issuing a warning on the label has been discontinued, as is indicated in the letter from Dr Cooper.”[1179]
She was dealing only with Hepatitis B. By early January 1976 Dr Maycock, to whom the correspondence dealing with the Assistant Secretary of Health’s letter had been copied, observed that the prevalence of hepatitis in the UK associated with UK blood and blood products had “long been smaller” than that in the US, but added (in chillingly prescient terms):
“However, until concentrate prepared from UK plasma is available, I would have said the benefits attaching to Hemofil and other similar concentrates of antihaemophilic factor, used with discrimination, outweigh the risk. There is always the problem of non-B hepatitis; some American authorities now say that this may account for 90% of transfusion associated hepatitis. This opens a new vista of complications.”[1180]
Set against this background, with concern about the detectability of hepatitis contained in plasma, the nature and motivation of the paid donors, reports on national television of how at least one company’s plasmapheresis centres operated, and a heightened concern to eliminate a need for reliance upon imported concentrate, the decisions to license two further commercial concentrates need some explanation. This is all the more so given that there needed to be reassurance as to the source from whom plasma was collected. Yet there appears to have been no site examination of any of the collection centres.[1181] Within the DHSS there was doubt over collection practices. Yet conditions which were thought should be insisted on as of real significance in ensuring as much safety as possible – the rate of donor rejections in collecting centres, centre by centre, in respect of the Factorate application – simply were not followed up on in respect of Koate and not provided in the specified detail for Factorate. There is however a hint that cost played a role it should not have done: such as the minute in which the Supply Division were stated to be “anxious” that Factorate be licensed as it was cheaper than Hemofil.[1182]
These events all tend in one direction. On the other hand, at this stage testing of plasma used in commercial products from abroad had improved: hence the variation of the licences in respect of Hemofil and Kryobulin to permit the use of RIA testing, which was a better screening test than had originally been used. Thus it was to be expected that the risks of transmission of Hepatitis B though not eliminated would be reduced, and although NANBH was not directly identified by such a test, it too might have been reduced since to an extent a test for Hepatitis B could be a surrogate for NANBH.[1183]
Though the dangers of making a judgement in hindsight must be borne in mind, the grants of the licences for Koate and for Factorate are highly questionable. There may have been reasons for what on the face of it appears to have been a decision to take a further risk which seems an unnecessary one to take, and should have been seen as such at the time. Given the events just described, there may well have been discussion. However, on the evidence available to the Inquiry, if safety were to be the primary consideration as it should have been, they are decisions which are difficult to justify. Unfortunately, such documents as remain reveal nothing beyond Dr Andrews’ report which can assist with the nature of them. The evidence, such as it now is, suggests an absence of consideration of plainly relevant factors. The process appears lacking, and the decisions flawed.
In November 1976 an application was made by Immuno to vary the product licence in respect of Kryobulin.[1184] The firm sought permission to use plasma from licensed plasmapheresis stations in the US in its manufacture, in addition to plasma from Europe. Kryobulin produced from the US was to be sold in a blue pack, Kryobulin produced from European sources in a red one. The former was said to be cheaper. In the minutes of a meeting of haemophilia reference centre directors on 6 April 1979, it was suggested that the implication was that the cheaper product carried the higher risk of plasma viral hepatitis and this worried some directors.[1185] Although a first version of the minutes recorded that Professor Ilsley Ingram[1186] had been in contact with Norman Berry, the managing director of Immuno Ltd, who had said they “aimed at making available to clinicians material which may carry less risk of transmitting hepatitis”,[1187] an amendment at Professor Ingram’s request was adopted at the next meeting. The amendment substituted that Norman Berry “had said that the American (‘blue’) material was offered for those who wished to take advantage of the lower American price, whereas the European (‘red’) material was still available for those who felt that it carried a lower risk of conveying hepatitis, although the Company regarded both products as equally safe.”[1188]
When the application to vary the licence was made the reason was set out in this way:
“It is possible to sell Factor VIII Concentrates produced from plasma of US origin at lower prices than European based material. Because of the preference in the UK market for this lower priced material, we also wish to make it available. Packs of Kryobulin from alternative source material will be of a clearly distinguishable colour e.g. blue as compared with present red. We will continue to make available European as well as the proposed new concentrate derived from American Plasma.”[1189]
Despite the apparent reasoning – to offer clinicians both a choice of product, depending on their views as to product safety, and a choice of price, to compete more effectively with cheaper US-made alternatives – when marketed neither the labels on the packaging nor the accompanying information sheets distinguished between them on the basis of the origin of the source plasma.[1190] Reference centre directors were however plainly aware of the difference, hence the discussion about it in their minutes of April, about which they would have been reminded in October 1979 when Professor Ingram corrected the record of the earlier discussion. However, neither patients nor other clinicians would necessarily have been aware. Nor would they have been alerted to the concerns of those reference centre directors who thought that the US-sourced product was cheaper because it carried more risk of hepatitis.
Internal documentation from Immuno AG, the manufacturing company, suggests a different reason from that signed off on the application for a licence. The documents are in German: an English translation is used here. The managing director of production at Immuno, Dr Otto Schwarz, is reported as having had a conversation with Norman Berry. A “Note for the Registration Department” states:
“In the future, two types of KRYOBULIN concentrate will be sold – KRYOBULIN 1 and KRYOBULIN 2. KRYOBULIN 1 = Made from European plasma (with a lower hepatitis risk) KRYOBULIN 2 = Made from US Licensed Source Plasma (proven to have a significantly higher hepatitis risk) KRYOBULIN 2 will be significantly cheaper than KRYOBULIN 1 because the British market will accept a higher risk of hepatitis for a lower-priced product. In the long-term, KRYOBULIN 1 will disappear from the British market.”[1191]
If, indeed, the concern expressed at the April meeting of reference centre directors was well-founded, it is troubling to note that sales of Kryobulin (blue pack) licensed thereafter exceeded those of Kryobulin (red pack) by 4.5 times.[1192] The last sentence in the quote above would be shown accurately to have predicted what would happen.
However, there is no evidence that the Licensing Authority was aware of the view expressed in the translation noted above. It was merely being asked to authorise Immuno to distribute a product sourced from US plasma, in the same way as it had licensed other products made by commercial rivals of Immuno from similar sources.
Though it might be argued that the Licensing Authority should have been more critically alert, and interrogated the reasoning more carefully, on balance it should not be criticised for permitting a less safe product (if it was) to be marketed in place of an existing product. To do so, it would have had to conclude that the plasma being used was less safe purely because it came from the US, to the extent that it should be banned. But the Licensing Authority had previously authorised products made from very similar sources, and continued to do so. It is difficult to see how it could have excluded blue pack Kryobulin without reviewing, and excluding, all those other products made from US-sourced plasma (or, indeed, made from plasma sourced from paid donors in any country).[1193] Kryobulin was no different from other commercial products in being made from the plasma of paid donors, from large pools. The time for refusing a licence because those two factors (paid donors and pool sizes) adversely affected safety was when Hemofil and Kryobulin were first licensed: so the “ship had sailed” and the authority was caught by the approach it had taken to its own earlier decisions.
However, those decisions should have been reviewed in the light of the development in 1975 and early 1976 reported above: yet the decisions in respect of both Koate and Factorate left much to be desired, for the reasons given above. Though it is clear that the regulatory regime as a whole did not fulfil its functions in respect of the importation and licensing of blood products commercially produced, if the decision in respect of blue and red pack Kryobulin is examined on its own, then for the CSM(B) to recommend that there should be no variation of the licence it would have to have been aware of a reputable study[1194] showing that paid German and European donors were significantly less likely to be infected with hepatitis than donors in the US. It follows that to find that it should have made a different decision would be to require too much of it.
There can be little doubt that although applications had to be judged against three criteria – safety, quality and efficacy – the paramount consideration among these three was that of safety. Three things reveal this. First, the inspiration for the governing legislation was what had been experienced with Thalidomide.[1195] To prevent a similar disaster happening again was primarily a question not of efficacy (whether the product “did what was claimed on the tin”), nor quality (consistency of manufacture, and ensuring that pharmacologically the product was as it was intended to be) but of safety. Second, the Medicines Act 1968 itself permitted consideration to be given to whether there was a product that might be safer which was already licensed, whereas it excluded an equivalent comparison in the cases of quality and efficacy. Third, the name of the recommendation-making committee was the Committee on Safety of Medicines. The name says it all.
Since safety is not necessarily an absolute, it involves balancing risk against benefit. However, where there are sufficient products already on the market, the introduction of a product which acts in a similar way, which does essentially the same job as they do, and is of similar quality means there is no or no sufficient benefit to set against the known risks to which that further product gives rise. When licences were given to Hemofil and Kryobulin in 1973 they did essentially the same job as NHS concentrates and locally produced cryoprecipitates, that of increasing Factor 8 levels in recipients. They acted in a broadly similar way.
Why, then, was the safety of recipients risked by permitting a more widespread distribution of commercial concentrates than was the case when they were imported on a named person basis? Certainly, one of the reasons for the licensing of imported commercial products to treat bleeding disorders may have been to satisfy a desire of clinicians in the UK to use a product with the advantages which factor concentrates (both commercial and NHS) had. These are undoubted when it comes to convenience and ease of administration but, as observed above, have only a tangential bearing on safety. The major change in haemophilia therapy since the Second World War had been the introduction of cryoprecipitate from 1966 onwards. It was the product principally in use in 1973 when the first licensing decisions were made in respect of concentrate. It was thought desirable that there should be more factor concentrate to reap the advantages which factor concentrates gave. But given that those advantages were, on analysis, matters principally of convenience of administration,[1196] the price of having more factor concentrates which were from large pools and paid donors was the taking in of products manufactured in a way which significantly increased the risk to recipients that they would incur serious, and sometimes fatal, disease.
There is limited documentation which bears upon the reasoning of the CSM(B) in 1973 and 1975 of which we now have sight. Before the Committee would have been the licence application, and the medical report by the medical assessor (in the cases of Hemofil and Kryobulin this was Dr Thomas; in the cases of Koate and Factorate, Dr Andrews). No other significant documentation has come to light. There is no record of the discussion. The Sub-Committee kept its deliberations under wraps. No one not a party to the discussion would have known of it. No witness who was present, and is still available to be asked, has a sufficient memory to fill in any of the details of what was said.
The supply of products on a named patient basis places an onus upon the medical practitioner to justify their choice of product should need arise and if it appears they may have chosen badly. By contrast, once a product is licensed practitioners choosing it for use in therapy are likely to consider that the fact of it being a licensed product is an indication of its safety, quality and efficacy. They will know that regulatory authorities whose primary concern is safety have authorised its marketing and distribution: the burden of justifying the choice of product is then some distance towards appearing justified. Summarising what one clinician ruefully said to the Inquiry, surely, if it was licensed it was safe?[1197]
A possible basis for the decision made by the CSM(B)/CSM, at least as far as Hemofil is concerned in 1973, is Dr Thomas’ final argument in his report that “no attempt is made to disguise the risk of hepatitis, and it may be considered that the decision to use this material could be left to the individual clinician who can balance the potential hazard against the anticipated therapeutic benefit to the patient.”[1198] However, what was required was a judgement by the CSM as to the safety of the product. It was for it, not others, to draw the balance. If those words, however understandable they may seem, were adopted by the CSM in its reasoning (it, and not Dr Thomas, had responsibility for any decision) it would be accepting an approach which abdicated that responsibility. If the CSM were to take this approach, it would have to make it clear to the clinician (and ultimately the patient) that a decision as to overall safety risk/benefit was what was expected of the clinician: it could not be assumed from the fact of licensing. It could have considered that clinicians, some of whom might be quite junior, who were in practice likely to be exposed to pressures of time and emergency in a hospital setting, do not always have time and leisure to reflect and research overall risks and benefits. It might have reflected that an Act intended to assure the safety of medicinal products after the Thalidomide tragedy would not have been satisfied by a decision that it was for a clinician to determine the risks and benefits of prescribing that drug; but, rather, that there are some decisions as to safety which are best routinely[1199] taken out of clinicians’ hands. In short, if leaving it up to treating clinicians to decide on the safety of the product for use, was the basis for the decision of the CSM to license it, it was unacceptable.
Given the belief at the time the initial licensing decisions were made in 1973 that commercially manufactured blood products sourced from paid donors and manufactured in large pools were less safe than either NHS concentrate (made from smaller pools of plasma derived from volunteers) or cryoprecipitate (less likely to transmit infection because of the very small pools or single-donor nature of the product, and also made from volunteers), which was a rational and evidenced viewpoint, and given the absence of any information showing that patient safety was at risk by reason of a failure to import factor concentrates,[1200] the decisions to license Hemofil and Kryobulin are not easy to understand.
The decision to license Profilate is justified only by the fact that it followed the licensing of Hemofil and Kryobulin. The decisions in respect of Koate and Factorate however occurred against a different background, especially since it was now becoming widely appreciated not only that testing for Hepatitis B was imprecise, but also that the majority of infections were of a form of hepatitis for which there was a supposed viral cause but no available test (neither Hepatitis A nor Hepatitis B but a virus or viruses which were blood borne: non-A non-B Hepatitis). Conditions were proposed which were aimed at reducing the risks of infection: but they were not insisted on as they should have been, and answers to requests for information could be unrevealing, and ambiguous.
It is surprising, given the changing context summarised above, the developing knowledge of the potential risks of non-A non-B Hepatitis, and the general view that factor concentrates were likely still to cause infections with Hepatitis B, that the renewal of licences (a process which occurred every five years[1201]) was not accompanied by detailed discussion of whether it was sufficiently safe for the products to remain licensed. There is no evidence that this detailed consideration took place.[1202]
In February 1980 there is a somewhat curious example of an exception to this. Speywood had a product licence to distribute Koate (as set out above) following an agreement with the manufacturer, Cutter, to do so. That agreement expired. Cutter did not propose to renew it. Accordingly, in February 1980 Speywood obtained a variation to its product licence to allow it to: (a) sell its remaining stock of Koate for one year, and (b) import unlabelled vials of Factor 8 concentrate manufactured by Cutter for relabelling and sale under the name Humanate. Later documents show that Humanate was Koate re-labelled.[1203] However, NIBSC raised concerns that since Speywood and Cutter were no longer in contract, they could not obtain details from Speywood as to the source of the plasma, the place or method of manufacture, such that the licence could no longer safely be continued. The Licensing Authority wrote to Speywood to vary the licence because:
“Humanate could no longer be regarded as a product which could safely be administered for the purposes indicated in that product licence since evidence of access to data relating to the original manufacture, as evidenced by the absence of protocol data relating to the source of donor blood and in process control, was now lacking … Without this evidence, there was no means of ensuring that the product had been manufactured under conditions which could be shown to minimise the risk to patients of contracting, for example, NON-A and NON-B hepatitis. The action which was proposed would be taken in respect of any product licence for a biological product under similar circumstances”.[1204]
Speywood exercised its right to argue an appeal before the CSM. The hearing maintained its advice that “because of the risk to patients arising from lack of evidence as to the origins and provenance of the donor blood, the Committee were not satisfied as to the safety of the product.”[1205]
There is a contrast between the approach taken here – in essence, that if there was not full access to knowledge of “the origins and provenance” of donor blood the product would not be licensed on safety grounds, and the approach taken in respect of the licensing of, for example, Koate, where that information was not provided,[1206] but the licence was granted.
Reconstructing the past as it was inevitably has shortcomings, given the limited material available. As a result, I have no adequate information[1207] to explain a recommendation that it was on balance safe to license Hemofil and Kryobulin when they were first licensed. On the face of the applications, to use the products exposed patients to a real risk of hepatitis. The risks were, if anything, emphasised by the report of Dr Thomas in respect of Hemofil. Safer products were already in use (though it is unlikely that the practice of the CSM involved any detailed comparison of safety). The best insights into the reasoning now available are the reports of the medical assessor for both. The reports contain much to concern a reader in respect of safety, and nothing other than general convenience in use to balance against those concerns. Such reasoning as these reports offer, if adopted, would not be a proper basis for the decision, for no acceptable balance is struck; no other reason to justify licensing is apparent; and there is no discussion of the context in which safety fell to be assessed, that of safety concerns being expressed by respectable commentators.
I have concluded that on the evidence before the Inquiry, such as it is, there was evidence of a lack of safety. The risk was a serious one. Though safety is a balance, and not an absolute, there is no material now[1208] available which shows what it was that may have tipped the scales in favour of licensing. I have concluded that the decisions were wrong.
They led to the decisions about Profilate, Koate and Factorate, in respect of which (so far as the last two are concerned) there were further reasons[1209] to think the decisions flawed. The requirement was to give particular consideration to safety. The evidence available to the Inquiry suggests that safety was not put first. Having considered all the available evidence, I have ultimately to conclude that the decisions should not have been taken as they were: they should certainly not have been left to individual clinicians to take.[1210]
In March 1981 members of the Haemophilia Centre Directors’ Organisation became alarmed by reports in the press about the importation of blood products into the UK. Their chair, Professor Arthur Bloom, expressed two concerns to Dr Holgate of the DHSS.[1211] The first was a concern that material produced by a US company had been sold “through brokerage or other means”to Speywood where it had been relabelled as a product of their own.[1212] A second concern was that it had been reported by Dr Geoffrey Savidge that a firm (Inter-Pharma) intended to market cut price Factor 8 obtained from Cutter and from Hyland, and he was concerned that the material was cleared for use and had passed the “normal control mechanisms”. This was especially since the Hyland material might be high potency, rather than the cheaper intermediate variety which had “been marketed in the ethical way in the UK.” The UKHCDO were aware that it might be difficult to be sure of the exact origin of plasma used in any of the currently available concentrates.
Dr Holgate replied. He suggested that the Speywood issue was “being dealt with”, and that Inter-Pharma was necessarily subject to licence requirements. He stated (when responding to the Speywood issue): “As I am sure you are aware one of the cornerstones of our philosophy for the licensing of ‘biological’ products is to have detailed knowledge of and control over early stages of manufacture and in-process control – this including source material.”[1213]
In doing so, he made a bold claim. There is little, if any, evidence to back it up. Certainly, in the early 1970s Dr Thomas visited Hyland facilities in order to compile his report in respect of the licensing of Hemofil. However, no similar report was made to the CSM(B) when it was considering the applications for licences made later in the 1970s. When she worked in the Medicines Division, Dr Walford also recalled a visit she had undertaken with two inspectors to the US, to examine two blood product manufacturing facilities on sites fairly close to each other. She recalls it because she ended up writing the report. In summary, she described it as “not a happy one” for the manufacturers. She said “We were very unhappy … about the facilities … [there was] the big clean area that was not a sterile area … and the toilets opened up into and off the clean area and people were just toing and froing and there was no changing of clothes, and so on, and that was not good practice, and we wrote it up, amongst other things.”[1214] As already mentioned, Professor Zuckerman visited Immuno facilities in Vienna shortly before 1976[1215] and was not impressed by what he saw. Dr Thomas had informally been permitted to see the Immuno factory not long after Kryobulin had first been licensed, and thought parts of what he saw were concerning.[1216] It is unclear how “control”[1217] was exercised over facilities such as these, in another country and subject to their own regulatory systems. It was also a surprising comment for Dr Holgate to make given that he had been minuted at a meeting in 1975 as saying that “shortage of funds inhibited visits to manufacturers’ premises abroad”.[1218]
It is difficult to think that there was anything approaching a comprehensive system of inspection and control of the sources of plasma used in manufacturing commercial blood products.[1219] Some was sourced from prisons.[1220] Some was, at least for a while, sourced from countries outside the US. There was a considerable trade in plasma; some was supplied to companies by plasma brokers. It is difficult to know where the original source was – yet it was this in respect of which the UKHCDO had sought some clarity. Occasional visits of the sort described by Dr Thomas and Dr Walford, echoed in the Granada World in Action programme to which Professor Zuckerman had contributed, do not, on the face of it, justify the claims that Dr Holgate was making – there should be far more evidence, such as correspondence showing that the DHSS had learned lessons from similar depressing reports (when and if they were made) and was taking manufacturers to task, then re-inspecting the facilities and processes to satisfy themselves that improvements had been made, under the threat of revoking licences or of imposing conditions to require those improvements. All that would be necessary before claims of the sort Dr Holgate made could be accepted.
This is, however, taking Dr Holgate’s claims as standing in isolation from their context. The context was a response to the particular situation regarding Speywood, and its marketing of Humanate. The Licensing Authority could and did exercise some degree of “control” through imposing conditions on the product licence, for example specifying the warnings that should be used, the use of international units as measure, and requiring information about donor rejections,[1221] donor sources, detailed accounts of how the product was manufactured, and the results of tests done during and on completion of manufacture. All of that control was indirect: but it was backed up by the power to refuse a licence and/or batch release to a company that did not comply. An example was Speywood. It could not supply the information requested. In consequence, its product was not released onto the UK market.
As a general statement, Dr Holgate’s comment that the UK Licensing Authority had “detailed knowledge and control over early stages of manufacture and in-process control” may be criticised for overstating the degree of control exercised. The specific context of the letter to which he was responding may provide mitigation: but it remains the fact that only some inspection as such occurred, and the indirect controls described in the last paragraph depended centrally on knowledge derived from the manufacturers themselves.
I have set out in an earlier chapter the story of the developing knowledge of AIDS in the Western world, starting in June 1981. It is nonetheless necessary to set decisions taken in March 1983 by the FDA, and then in July 1983 by the CSM(B) and the CSM in context.
By early 1982, The New England Journal of Medicine carried an article suggesting that the recorded cases of the principal symptoms included in the syndrome (PCP and Kaposi’s sarcoma) might only represent the tip of the iceberg in terms of the prevalence of conditions associated with AIDS.[1222]
By August 1982, it had been reported to the World Congress of Blood Transfusion (Budapest) that it was suspected in the US that an infective agent in blood concentrates resulted in people with haemophilia dying of AIDS.[1223] Later that month, Alpha committed to stop using plasma collected from donors who were Hepatitis B surface antigen (“HBsAg”)[1224] positive in order to manufacture Factor 8 and Factor 9 concentrates, a move that recognised the possibility that there was a viral cause of AIDS which was transmissible by blood products.[1225] Dr Denis Donohue of the FDA asked the pharmaceutical companies to stop using blood collected from donors likely to have high levels of antibodies to hepatitis.[1226]
By September haemophilia doctors in the UK were alerted to the possibility (or risk, by another word) that whatever caused AIDS might be a virus, and that this could be transmitted by blood or blood products.[1227]
By September 1982 it was reported in the Morbidity and Mortality Weekly Report (“MMWR”) by the Centers for Disease Control (“CDC”) of the US that there had been 593 cases of AIDS, 243 of whom had died;[1228] by October 1982, it was reported that the CDC had been notified of 684 individuals who had been diagnosed with Kaposi’s sarcoma (“KS”) and/or serious opportunistic infections resulting from an acquired immune deficiency[1229] and that at least 260 (41%) had died;[1230] by December 1982 the MMWR figure was 788 cases.[1231] If the same mortality rate were to occur in people with haemophilia, then the risk of dying from AIDS would be far greater than from any other cause. It could also be seen that the number of cases was doubling numerically roughly every six months.
By November 1982 Dr Craske expressed his view that there were three possible causes of AIDS. He discounted the first two of these – the taking of amyl nitrite, and the immunosuppressive effects of CMV.[1232] He thought an infectious agent was the likeliest of the possible causes he identified.[1233]
By the end of 1982 – according to Dr Charles Rizza of the Oxford Haemophilia Centre – it was clear (and should therefore have been known by all UKHCDO directors) that there was a real risk that AIDS could be transmitted by an infectious agent carried by blood products.[1234] By now, too, it was becoming more and more apparent that this was actually the case, though certainty was still lacking: it was reported that a baby in San Francisco had developed symptoms of AIDS after receiving transfusions. One of those transfusions had been given by a donor who was subsequently diagnosed with AIDS.[1235]
A viral cause was further implicated on 7 January 1983, when the MMWR noted that it had, since June 1981, received reports of 43 females who had developed pneumocystis pneumonia or other opportunistic infections typical of AIDS. Some had no risk factor other than to be the steady partner of a man with AIDS or at high risk of it. If accurately reported, the cause was highly likely to be viral, transmissible by sex as well as blood, and similar in these respects to Hepatitis B.[1236]
On the same day Alpha issued a press release which said that: “The evidence suggests, although it does not absolutely prove, that a virus or other disease agent was transmitted to [haemophilia patients with AIDS] in the Factor VIII concentrate, derived from pooled human plasma”.[1237]
Further information emerged about the nature of the risk. Dr Craske told 21 haemophilia directors at a meeting in the Excelsior Hotel at Heathrow on 24 January 1983[1238] that:
The Lancet [1241] and New Scientist [1242] concurred that the prime suspect was a blood-borne virus.
Other countries in Europe started taking precautions: for instance, Dutch physicians treating haemophilia patients agreed to use only cryoprecipitate in children under four and suggested that all other patients should consider cryoprecipitate as the treatment of choice, followed by locally produced (smaller pool) Factor 8 and Factor 9 concentrates. The Dutch Association of Haemophilia Patients advised members that it was highly likely that Americans with haemophilia had been infected by using factor concentrates.[1243]
When the CDC reported in March that blood products or blood appeared responsible for AIDS among haemophilia patients requiring clotting factor replacement it also noted that the first signs of AIDS might take two to three years to emerge after exposure to a possible transmissible agent. It added that there was a fatality rate of more than 60% for those first diagnosed over one year previously.[1244]
Reviewing the position as it was in early 1983 leads to these two observations.
The US was the epicentre of the AIDS epidemic in the Western world. The earliest recorded case identified in the UK was in December 1981, two years after the first symptomatic case of AIDS was believed to have occurred in the US – but the person concerned had regularly travelled to the US. An outbreak in the UK was thus separated not only by geographical distance but also by time from that in the US: for those who chose to be alert to it, there was an “early warning” of what might yet be in the UK, coupled with a knowledge that AIDS had come to its shores. After all, Terrence Higgins had died of AIDS in July 1982, and a Trust in his honour had already been set up by his friends.[1245]
During 1982, concern had risen in the US that the epidemic had many features which were reminiscent of the previous epidemic of Hepatitis B, which in part had been spread by blood and blood products as well as by sex. Because it was now being reported to the CDC as arising in Haitian patients and intravenous drug abusers, who were regarded as less likely to use amyl nitrites or to have anal intercourse[1246] than male homosexuals, the CDC considered that this indicated that the cause was probably an infectious agent, transmissible by blood.[1247] This view was increasingly shared by European epidemiologists.[1248] More significantly still, commercial producers of blood products recognised that whatever the true cause might be they could not exclude the possibility that it was indeed an infectious agent transmitted by blood products. They started to consider the sources of the plasma, which they bought, to exclude riskier donations. Alpha issued a press statement on 7 January 1983 advising that there was a real risk that those who took its products might as a result develop the symptoms of AIDS.[1249]
The FDA decided against this background, augmented as it was by further comment in both the popular and medical press in 1983 and by the growing epidemic, to press commercial producers to take steps to avoid the use of blood from high-risk groups when preparing factor concentrates. The pressure fell short of making a formal regulation (though it is often, erroneously, referred to as such). So, it became formally a recommendation, on 24 March 1983.[1250] The recommended steps included adopting standard procedures to quarantine, and dispose of, any products collected from donors known or suspected of having AIDS. They were to train personnel responsible for donor screening to recognise early signs of AIDS. Blood and plasma facilities were recommended to inform persons at increased risk of AIDS that they should stop donating. Those at increased risk were often referred to “the four Hs”(homosexual males, heroin addicts (IVDU users), Haitians and those with haemophilia). In short, people within the “four Hs” were much less likely to be sources of blood or plasma after 24 March 1983. All products made for distribution after that date were to be made from plasma collected after 24 March 1983 in accordance with these recommendations, and products made from donations collected earlier were supposed to be labelled to indicate this.[1251]
Dr Joseph Smith was the director of NIBSC, and chair of the CSM(B).[1252] By late March 1983, Dr Smith had been made aware of letters recently released by the FDA drawing attention to the recommendations. Having been alerted by these letters, Dr Smith wrote to Dr Leslie Keith Fowler, a senior medical officer in the Medicines Division of the DHSS, on 28 March 1983. He came straight to the point: his opening words were “I think it would be advisable to consider, at a meeting of the CSM(B), the problem of AIDS in relation to licensed blood products.” He added that it would be “extremely helpful to secure the advice of Professor Arthur Bloom” and also the latest information on surveillance in the UK from the CDSC. Dr Smith drew attention in his letter to the fact that the US was taking steps to avoid the use of blood from high-risk groups. He asked if Dr Fowler could prepare a brief paper on which the discussion might be based “together possibly with a note that Spence Galbraith’s unit might be prevailed upon to prepare.”[1253]
In the event, only two documents were placed before the CSM(B) when it finally met on 13 July 1983:[1254] a paper from Dr Fowler and an annotated agenda prepared by Dr Smith that formed the basis for discussion. No paper from Dr Spence Galbraith or his unit was circulated and there is no evidence of Dr Galbraith being asked to prepare any such paper. Dr Galbraith had written, on 9 May 1983 to Dr Field of the DHSS setting out his view that the importation of concentrates should cease. The broader significance of that letter is considered elsewhere in this Report[1255] but for present purposes the key fact is that the letter was not provided to the CSM(B).
The second document prepared for the meeting of CSM(B) was a suggested “agenda”for the discussion on AIDS and blood products.[1256] This was prepared by Dr Smith and dated 28 June 1983. The agenda started with the assumption that “participants will be familiar with the problem and with at least a proportion of the many publications.” Headings for the discussion and a suggested first speaker were proposed. Somewhat unusually for an agenda, “brief possible conclusions”were also indicated, although Dr Smith added “doubtless these would be changed radically.”[1257] From the agenda and its suggested conclusions, it appears that even before the meeting of the CSM(B) took place, Dr Smith’s view (or, if the suggested conclusions were based on discussions with others, the views of those others),[1258] was that the very issue under consideration could not be recommended: the suggested conclusion was “Impracticable on grounds of supply”.[1259]
Dr Fowler’s paper – on which he was not invited to speak, though it presumably was read by all attendees – took as a starting point that immune deficiencies were not new, and whilst accepting that AIDS was clearly a transmissible condition queried whether it had a single causative agent,[1260] and appeared to think it questionable that factor concentrates posed any additional risk to people with haemophilia. He asked in it whether haemophilic AIDS might be a function of the concentrate itself, but then said: “one cannot ignore other views and hope the problem will go away.” He identified four potential responses: improving donor selection; using cryoprecipitate to minimise exposure to multiple donors; using labelling and stop orders to prevent dumping of US concentrates manufactured before the FDA recommendation; and potentially heat treatment in the future.[1261]
Dr Smith regarded Dr Fowler’s paper as representing that division’s evaluation of the cause of the AIDS problem.[1262] This is almost certainly an inaccurate evaluation since Dr Walford was clear that the general and accepted view within the medical stream of the civil servants of the DHSS was that the likeliest cause of AIDS was an infective agent.[1263]
The CSM(B) met on 13 July 1983.[1264] This was a special meeting of the CSM(B) rather than one of its routine scheduled meetings. The meeting was attended by nine members of the CSM(B) itself.[1265] The invited experts were Professor Bloom (UKHCDO chairman), Dr Craske (PHLS virologist), Dr Galbraith (director of CDSC), Dr Harold Gunson (CMO’s adviser on blood transfusion) and Dr Phillip Mortimer (PHLS virologist). Also present were Dr Holgate (medical assessor), Dr Purves (pharmaceutical assessor), Mr Morgan (secretary) and others from NIBSC and the DHSS, including Dr Walford.
The meeting began with a reminder from Dr Smith that the material those attending received was confidential and should not be disclosed outside the meeting. The minutes were succinct: Dr Smith told the Archer Inquiry that that was the practice in the Medicines Division.[1266] The upshot of the meeting was that it did not decide to take any action in response to the risks from imported factor concentrates.
The discussions that took place were not recorded in the minutes. Instead, the meeting’s conclusions were set out. They are not identical to, but are for the most part similar to, the suggested conclusions in Dr Smith’s annotated agenda.[1267]
The first issue to be discussed was the cause of AIDS, on which Dr Mortimer was to speak first. The conclusion was that “The cause of AIDS is unknown, but an infectious aetiology seems likely.” Although Dr Smith told both the Archer Inquiry and this Inquiry that he was almost certain by the end of 1982 that a new virus was the explanation, this was watered down between the possible conclusion in his annotated agenda and the minutes, perhaps influenced by Professor Bloom’s and Dr Fowler’s views.
Dr Galbraith was then to discuss epidemiology. From annotations to a copy of the agenda, this may have included a briefing on the numbers to date infected.[1268] The conclusion, though, is not consistent with Dr Galbraith’s earlier advice and looks more like Professor Bloom’s characterisation of the risk:
“Patients who repeatedly receive blood clotting-factor concentrates appear to be at risk, but the evidence so far available suggests that this risk is small. The risk appears to be greatest in the case of products derived from the blood of homosexuals and IV [intravenous] drug abusers resident in areas of high incidence (eg, New York and California), and in those who repeatedly receive concentrates in high dosage. Balanced against the risks of AIDS (and of other infections transmitted by blood products) are the benefits of their use; in the case of haemophilia they are life-saving.”[1269]
It is difficult to square this view of risk with, for instance, the views expressed by Dr Craske in the paper he wrote the previous autumn in which he drew attention to the fact both that there was a substantial delay in symptoms emerging and that mortality after first symptoms was high (around 50%).[1270] Nor does it appear that the Committee was informed of a letter Dr Evatt had sent to Professor Bloom on 7 March 1983, in which he described the AIDS epidemic as evolving at “a frightening pace … The incidence rate has been increasing in hemophiliacs and the epidemic curve paralays [sic] that of the total epidemic curve.”[1271]
The second problem is the belief that factor concentrates were life-saving. This is true in part, but was not the unique preserve of commercial concentrates: it was true also of NHS factor concentrate and cryoprecipitate. Moreover, the phrase over-inflates the benefits of factor concentrates, which were used mostly in non-life-threatening circumstances. It is easy to see how this over-simplistic belief, that people with haemophilia would die without imported factor concentrates, would skew the outcome of the deliberation.
Continuing with the meeting, the annotated agenda suggested that Drs Gunson, Craske, Schild and Fowler would be invited to speak about screening tests and future heat treatment but the main focus of the discussion was next.
Professor Bloom was invited to address the question of whether to withdraw (all) factor concentrates on grounds of safety. The conclusion had no subtleties:
“The possibility was considered of withdrawing clotting factor concentrates from the market and replacing them with cryoprecipitate. It was concluded that this is not feasible in the UK on grounds of supply.”[1272]
As for withdrawing US products,[1273] the CSM(B) concluded:
“this is not at present feasible on grounds of supply. Moreover, the perceived level of risk does not at present justify serious consideration of such a solution. Efforts are however being made to secure UK independence of foreign suppliers of clotting factor concentrates. This should reduce markedly, although not eliminate, the risks to recipients of these products, and the Sub-Committee strongly supports this aim. The Sub-Committee was also informed that the UK Haemophilia Centre Directors have adopted a policy for use of US Factor VIII in order to minimise risks as far as possible.”[1274]
Dr Walford in her statement[1275] said that she did not know the factual basis for the conclusion that the replacement of concentrates with cryoprecipitate was not feasible, but observed that Dr Richard Lane was at the meeting as a member of the CSM(B). This conclusion is consistent with reports which he had given to a CBLA meeting on 27 April 1983.
It is plausible that this is the case. Dr Lane had produced a report for the CBLA, dated 22 April 1983.[1276] This said that the potential of BPL to manufacture small pool freeze-dried cryoprecipitate in significant amounts as an alternative had been ruled out on logistic production considerations. His objection to the production of single-unit wet cryoprecipitate (which would be in regional transfusion centres) was that it would “seriously reduce the efficiency of the current plasma procurement programme to satisfy BPL targets for factor VIII concentrate.”
However, the production problems identified by Dr Lane were concerned with BPL’s ability to produce freeze-dried cryoprecipitate. They had nothing to do with the ability of regional transfusion centres to produce single-unit wet cryoprecipitate. The overwhelming evidence given to the Inquiry from directors of regional transfusion centres was that they would have been able to revert to the production of cryoprecipitate without great difficulty.[1277] Dr Lane’s objection was not one of feasibility, or logistics, so far as this was concerned: it was, rather, that it would reduce the amount of plasma available to BPL. Understandably, given his position as director of BPL, Dr Lane’s focus was on the impact on BPL and its activities.
As a result, it seems likely that the CSM(B)’s decision was based in part on a mistaken belief that cryoprecipitate could not be produced in large quantities.
Moreover, the position in respect of continued importation appears to have been based on a complete misunderstanding (at least that of its chair) of the position regarding self-sufficiency. Dr Smith thought it was going to be achieved imminently. He told the Inquiry that he had “the clear impression” that the UK’s self-sufficiency was expected to be achieved within a period of months (he thought about two further months).[1278] Indeed, he recalled asking the DHSS (probably Miss Zoe Spencer) after a couple of months about progress, and that she had remained positive about progress whilst telling him that self-sufficiency had not yet been achieved.[1279] This repeated his evidence to the Archer Inquiry which was that, from the discussions at the meeting, he had gained the clear impression that UK self-sufficiency was expected soon.[1280]
A view that self-sufficiency was going to be imminently achieved must inevitably have skewed the decision-making. Indeed, in Dr Smith’s written evidence, he described the Committee as having gained “some comfort”[1281]from this view of the position.
As for the Sub-Committee being informed that the UK haemophilia centre directors had adopted a policy in order to minimise risks as far as possible, the errors in this conclusion are demonstrated by questions and answers during the course of Dr Walford’s evidence:[1282]
“Q. ... This particular paragraph is all about risk, isn’t it?
A. Yes.
Q. It talks about the ‘level of risk not at present’ justifying withdrawing US product.
A. Yes.
Q. Then the next three sentences deal with risk, and they throw into the equation to assess what the risk actually is, the sense of when and if we become self-sufficient in making our own concentrate, then the risks of US concentrate will, by definition, fall away: we have our own risks, but we won’t have the USA’s risks.
A. Yes.
Q. The second part is that there has been a change of policy or a policy which ensures that the risk is kept as low as possible. In terms of the first of those two points, the context was that of what was possibly a transmissible agent that was thought to be the most likely cause -- you yourself thought it was the most likely cause?
A. Yes.
Q. – which, if it was something which had a long incubation period which, was understood at the time, might take a while to manifest itself in the way that epidemics do.
A. Yes.
Q. So the sense that in a year or two or three or four’s time there might be sufficient production domestically really had nothing to say about that risk, did it?
A. No, the risk as they were defining it was what they perceived as the risk at present time, yes.
Q. And the future production of self-sufficiency, enough quantities, unless it was very, very imminent –
A. Yes.
Q. – would have nothing to say on it?
A. No, it does appear to be another non sequitur.
Q. So it’s – yes, it’s another non sequitur.
A. Yes.
Q. The last looks like misinformation, the sense that there’s been a change when there hasn’t been a change.
A. Yes.
Q. Because the general message being sent out from – as I understand your view of – and at the moment it may well become my own view, of what is said in the letter of 24 June, is that the UKHCDO weak recommendations really were: business as usual.
A. Or slight improvement on business as usual, if you like, emphasising how best practice –
Q. It gives a nudge.
A. Best practice.”
Dr Walford there recognised there had been at least two “non-sequiturs” in the reasoning.
The CSM(B) reached three further conclusions about factor products. First, that it was advisable that factor products for use in the UK should be derived from plasma collected after the FDA recommendation as soon as that became feasible. Second, that manufacturers were working on viral inactivation[1283] and when licence applications were received, it would be important to examine not only improvements in safety but also clinical effectiveness. Third, that manufacturers should be stopped from making claims about the safety of heat-treated products when safety and effectiveness had not been established by the Licensing Authority.[1284]
The short answer, it appears, is none, at least insofar as Dr Smith can recall. He told the Archer Inquiry that he had only seen Dr Galbraith’s letter – which he described as a “very good letter” – recently, and that as far as he could remember it did not come to the CSM.[1286] In his statement to this Inquiry, he stated that neither he nor, he thought, members of the CSM(B) knew that Dr Galbraith had written to the DHSS, and that Dr Galbraith made no mention of it at the meeting.[1287] The contemporaneous documentation (summarised above) suggests that Dr Smith is right and that the Galbraith letter and paper did not reach the CSM(B).
Professor Christopher Bartlett gave written[1288] and oral[1289] evidence to the Archer Inquiry, effectively on behalf of and at the request of Dr Galbraith whose health did not enable him to give evidence himself. In 1983, Professor Bartlett had been a consultant epidemiologist to the CDSC, reporting to Dr Galbraith, and became the Director of CDSC in 1988 when Dr Galbraith retired. His written statement, referring to Dr Galbraith’s letter and paper of the 9 May 1983, explained that Dr Galbraith had sought his opinion on the final drafts and that he fully concurred with the conclusions and advice he had expressed. In his oral evidence it would appear that Professor Bartlett understood that Dr Galbraith repeated his advice orally to the CSM(B).[1290] Professor Bartlett commented further in his oral evidence that although there were, by May 1983, only a small proportion of recipients of Factor 8 concentrate who had developed AIDS “the risk may not have been small” and added that “I think this last piece of evidence about the risk is one where other experts at the time disagreed; they felt the risk was small. So there was a difference of opinion at that time and that came out in the meeting of the Sub Committee of Biologicals.”[1291]
Professor Bartlett had understood that the CSM(B) meeting was convened in response to Dr Galbraith’s letter.[1292] However, in the light of Dr Smith’s letter of 28 March 1983 that seems unlikely, for the letter predates Dr Galbraith’s contribution. Further, the fact that Dr Galbraith’s letter and paper do not appear to have been circulated to members of the CSM(B) or to other invited experts tends to confirm this.
Professor Bartlett recounts that he spoke to Dr Galbraith the day before he gave evidence to the Archer Inquiry and conveyed that Dr Galbraith’s reaction to the CSM(B) conclusions was one of being “completely bowled over.” Professor Bartlett reported his own reaction as being “dismayed at the time.”[1293]
Professor Stephen Palmer, who took up a position as CDSC’s first medical consultant epidemiologist in Wales in May 1983, has explained in his statement that in mid 1983 Dr Galbraith was unwell and not able to be present at CDSC.[1294] Dr Galbraith’s colleague would record on 5 September 1983 that he had been off sick with severe arthritis for the previous six weeks.[1295] This might, possibly, explain why Dr Galbraith’s views as expressed in strong terms in his paper to the DHSS do not appear to have been similarly expressed to the CSM(B).
Finally, it should be noted that both the Archer Inquiry and the Penrose Inquiry seemed to have proceeded on the (inaccurate) basis that Dr Galbraith’s statement had been considered and rejected by the CSM(B).[1296]
On 23 June 1983, the Council of Europe recommended the governments of member states “to take all necessary steps and measures with respect to the Acquired Immune Deficiency Syndrome and in particular: to avoid wherever possible the use of coagulation factor products prepared from large plasma pools; this is especially important for those countries where self-sufficiency in the production of such products has not yet been achieved.”[1297]
There is no evidence that this was drawn to the attention of the CSM(B). There is no evidence that it formed part of any discussion on 13 July, or later when the CSM itself decided to endorse the recommendation of the CSM(B).
Professor Richard Tedder is a medical virologist and physician, and a member of the Royal College of Physicians. His early training was in zoology. In a talk he gave in Cardiff in 1984, he is recorded as expressing the view that “in veterinary medicine, products from one country would not get through incoming Customs of another country in the way that … concentrates have come into the human market for haemophiliacs in the UK”.[1298] In his written statement he added:
“Personally, I would have recalled, prevented or very strictly controlled the use of imported commercial blood products, especially those from the USA, which were known to have a significant risk over and above the expected. If the same was to occur with a British product, then clearly recall would be appropriate. At the Middlesex, we would only have used such products if it was the only option to avoid serious harm to a patient. That was David Dane’s teaching.”[1299]
In evidence, he amplified that the use of prisoners for donated blood particularly in the US meant that the producer of the product could not “know their donor”, which Professor Tedder regarded as a cardinal principle.[1300] The decision of the CSM(B) does not seem to have been one which that virologist, speaking soon after the event, would himself have taken.
At its meeting on 21-22 July 1983 the CSM endorsed the recommendations of its Biologicals Sub-Committee. There appears to have been little by way of discussion, if any.[1301]
Professor Sir Michael Rawlins was a member of the CSM and was present at the meeting. He confirmed that it would be normal for the CSM not to have the papers that had been considered by the CSM(B), because the experts in the subject sat on the Sub-Committee rather than the full committee. He would, however, have expected the CSM(B) to examine and interrogate rigorously the evidence about the factor concentrates when reaching its decision. He expressed surprise that the CSM(B) did not keep the issue under review so as to look at it again actively after July 1983. He considered that Dr Galbraith’s letter and paper should at the very least have been provided to the CSM(B).[1302]
Although Sir Joseph Smith, in his written statement to the Inquiry, described the remit of the CSM and CSM(B) in relation to advice on the response to AIDS as relating mainly to dealing with applications for product licences or variations to them in respect to blood products, he also observed that there were occasions when the CSM(B) or the CSM considered broader issues relating to the safety of blood products in the context of AIDS. This led to advice, recommendations or “remarks” being conveyed to the Medicines Division of the DHSS for consideration by the Licensing Authority.[1303]
He thought that the CSM(B)’s meeting of 13 July 1983 was the most obvious example of this.
However, the Licensing Authority itself – the ministers – were not informed of the discussion of 13 July. Lord Glenarthur, who at the time had ministerial responsibility for policy relating to blood and blood products, was “completely unaware” of the CSM(B)’s meeting and deliberations.[1304] Lord Kenneth Clarke, who at the time was Minister of State for Health, did not think he was aware of the CSM(B)’s existence. He was, however, a “little surprised” that the issue was not drawn to the attention of Lord Glenarthur. [1305]
If the decision at this meeting had been as Dr Galbraith had proposed in May and as the Council of Europe had recommended in June, the consequence would almost certainly have been that many lives would have been spared, and many others saved from the desperation of infection by HIV when it was untreatable – and, for that matter also from the great difficulties caused by infection with what became known as Hepatitis C and to a large extent Hepatitis B.[1306]
In retrospect, the decision was almost certainly wrong. Whether it is now legitimate to see the decision as flawed at the time it was made demands further analysis.
The CSM and CSM(B) has as their principal focus the safety of the public, and in that light whether medicines were safe to import for use. By the time they met, there was a well-established risk that factor concentrates, especially from the US, were unsafe so far as hepatitis was concerned, and it was known that this was a serious disease with significant long-term consequences.[1307]
There was now also a very real risk that use of the same products as gave rise to a significant risk of hepatitis could also cause AIDS. The fact that the Sub-Committee appreciated that there was indeed a risk of AIDS,[1308] and that this risk was higher in the case of imported concentrates made in the US from large pools of purchased plasma than it was for concentrates and other products made from smaller pools from unpaid donors in the UK, is underlined by the reference[1309] to the clinicians adopting a policy towards the use of US Factor 8 which would minimise risks. This is a reference to a policy adopted by the UKHCDO for use by its members.[1310] In short, the Sub-Committee recognised that cryoprecipitate was safe[1311] (otherwise it could not have been given preferentially to those considered the most vulnerable). Though there were risks from using cryoprecipitate – if made in small batches, there might be a risk of bacterial contamination, and there was a greater risk of causing inhibitors because cryoprecipitate would contain more proteins than simply the clotting factor protein of interest – these were outbalanced by a greater risk of viral infection or[1312] AIDS arising from the use of large pool concentrates commercially manufactured.
The real choice was not between stopping importation, and requiring patients with haemophilia to go without treatment, or continuing it and exposing them to the risks of contracting AIDS and non-A non-B Hepatitis as a necessary adjunct to the advantages factor concentrates brought. It was a choice of therapy. Underpinning the Sub-Committee’s reasoning was an acceptance that cryoprecipitate was generally safer than concentrate.
The critical issue, therefore, in evaluating whether the decision was justified is not one primarily of safety, but whether the decision to continue the importation of factor concentrate “on the ground of supply” was reasonable. If sufficient supplies of cryoprecipitate to meet the continuing need for people with haemophilia to treat significant bleeding could be assured,[1313] the logic of the meeting’s reasoning should have led to recognition that a safer course would have been to suspend the importation of factor concentrates, and to consider carefully whether concentrates made from domestic, volunteer sources of plasma (“NHS concentrates”) should continue to be used to the extent they were.[1314]
The balance which the Sub-Committee said it was drawing was between the risks of AIDS and other infections being transmitted by clotting concentrates and the risks of ceasing to use them. It said that “in the case of haemophilia they are life-saving”.[1315] But as has just been pointed out, so too was the use of cryoprecipitate, and cryoprecipitate was safer. This language used in the minutes appears aimed to persuade rather than to convey a balanced picture.
In saying also that the evidence suggested that “the risk [of AIDS] was small”[1316] it is unclear what approach the Sub-Committee was taking to risk. The magnitude of risk is a combination of the likelihood of it eventuating, coupled with its severity if it does. A small incidence of a fatal outcome is of high magnitude, and all the more so where any disease leading to death is incurable. In 1983 AIDS could not be treated. To say the risk was small was most probably to refer to an estimate of its likely incidence: the incidence would have to be very small indeed to be of a low enough magnitude to justify a decision which would expose some patients to inevitable death. The Sub-Committee must have thought there was only a very small chance that the infectious agent they thought probable would actually cause an infection, or it could not properly have decided as it did. It is, however, difficult to see a proper basis for this.
Professor Bloom had apparently earlier assessed the size of the risk by reference to the number of cases of AIDS which had developed in the UK and Europe amongst people with haemophilia.[1317] Given the way he expressed himself in this letter to the Haemophilia Society about risks, he was committed to a view both that this was how to evaluate risk and that the risk was very small indeed. It is to be inferred that his contribution to the discussion at the Sub-Committee would have echoed this position. He was an influential figure, later to be described by a pharmaceutical company’s UK marketing manager as an “opinion former”.[1318]
Yet, a memo of 13 July 1983 from Dr Peter Foster to John Watt referred to the assertion (by others, but reflecting Professor Bloom’s expressed view) that the risk of contracting AIDS was one in one million. Dr Foster considered that this understated the risk by a factor of 100.[1319] Even this, revised by a factor of 100, does not display the caution necessary when dealing with a new viral infection.
Risk is to be assessed not by past experience of what has happened, but by an holistic assessment of what can be seen potentially as happening in the future, taking all the evidence into account. A reasonable worst case scenario should be the guide. Since it had been noted[1320] that it might take six months to two years for the first symptoms of AIDS to emerge (and some time after that for it to be confirmed as a case of the syndrome), since Dr Fowler had observed that the apparent long latency period meant that the seeds had been sown for disease in the future, and Dr Evatt had confirmed that 50% of people with haemophilia in a study in the state of Georgia already had T-cell abnormalities and 13% were markedly abnormal,[1321] it is clear there was contemporaneously at least one reasonable view of what scenario might follow. Dr Evatt’s figures suggested that 13 in 100 people with haemophilia looked to be on the threshold of AIDS, and the 50% figure and the epidemic history of the disease showed that the figure of 13 in 100 was likely to increase.[1322]
Dr Evatt had told Professor Bloom in March, in a clinically factual letter, that “the incidence rate has been increasing in haemophiliacs, and the epidemic curve paralays [sic] that of the total epidemic curve.”[1323] That curve showed that from small numbers initially the total figures had reached 1,150 cases in the US by March, 40% of which had come in the previous four months, each month showing an increasing rate of incidence. The implication was chilling. Yet there is no evidence that Dr Evatt’s letter was mentioned at all to the Sub-Committee.
Moreover, Professor Bloom’s approach was a scientifically inept way to evaluate the risk given that it was known that AIDS had a latency period following infection. It focused on the wrong figure. The number of reported cases was bound to be only a fraction of the numbers of those already infected but not yet symptomatic. Once it was postulated that the cause was a virus transmitted by blood or blood products, the appropriate question was not one which focused on the number of infections which had already become apparent, but one which focused on the risk that the plasma pool from which a batch was made had been contaminated.[1324] If even only one contaminated donation had been made to the pool, there was no scientific basis for assuming that its effect would be diluted by the other donations.[1325]
To assess the risk, first the chances of there being one (or more) contaminated donations to a pool needed to be assessed; that needed to be multiplied by the number of donors to the pool; and the risk to people with haemophilia who had concentrates from multiple similar batches then had to be assessed in the light of the knowledge that they had as many times that risk as they had had batches. A risk assessed in this way was an order of magnitude greater than that which was assessed simply by reference to how many confirmed[1326] cases had already been reported. Focus needed to be on what was potentially in the pipeline, not what had already been seen to come out of the tap.
Professor Bloom’s approach, as expressed in his letter to the Haemophilia Society, and the concise nature of the minutes of that Sub-Committee (which is apt to disguise almost as much as it reveals), suggest that his misdirected views[1327] as to the nature of the risk and the way it should lead to inaction may well have carried the day. If, as seems likely, the Sub-Committee was also aware that the Haemophilia Society was firm that it did not wish there to be a ban on the importation of US factor concentrate,[1328] this too must have had some influence. The members of the Sub-Committee may not have taken on board the fact that the Society’s view was in truth not a wholly independent view, but rather reflected the advice which it had sought from Professor Bloom,[1329] and he had given. If a view is expressed by one person to another it is seen as the view of just that one person. If, however, that other then relies on the view and expresses it to a third person, that third person may well conclude that two authoritative sources separately support the view, since that is how it will appear. And so views may spread, and gain acceptance, purely on the basis of apparent numerical support rather than merit.
Too cavalier a view was taken of the risks. Whilst there may have been still uncertainty about the precise scale of the risks, the reality of the risks was not properly appreciated. Dr Smith’s proposed conclusion as to whether an infectious agent was a cause was watered down, possibly because of the doubts expressed by Dr Fowler in what Dr Smith incorrectly took to be the authoritative view of the DHSS, coupled with Professor Bloom’s personal approach to risk. The analysis of risk was flawed. This is demonstrated within the minutes themselves by the approach the Sub-Committee took to further reliance on the purchase of commercial product from the US. In the corresponding minute, in apparent explanation why the Sub-Committee thought the level of risk did not justify withdrawing US preparations from the UK, the view is expressed that the efforts being made to secure independence of foreign suppliers of concentrates “should reduce markedly, although not eliminate, the risks to recipients of these products”.[1330] This must have assumed that a long-term solution could be an answer to a challenge likely to materialise, if at all, within the short term. It simply was no answer to such a risk.
A risk of infection is just that – a risk. But if the event which was risked was actually to happen – especially where it is realistic to suppose it might, as was plainly there to be seen on 13 July 1983 so far as AIDS was concerned – the nature of the supposed risk must be clearly kept in mind in determining what may reduce it. The nature of the risk of AIDS, which it was well justified to fear for the reasons given above, was not of a slowly evolving, gradual increase in risk. It was of the rapid escalation which Dr Evatt’s figures implied. Its progression was likely to be epidemic. There would be no reason to feel sure that the UK would not copy the US in this. Where there is a long incubation period after first infection before symptoms become apparent, an increase in the appearance of those symptoms will evolve only after the period is over, but then do so at an epidemic rate – with the unsettling knowledge that it is now too late to avoid those infections which have increasingly, in the meantime, been incurred. Dr Evatt’s figures show, in short, that there was no time for long-term solutions if indeed the cause was a virus.
Dr Smith mistakenly understood – he thinks now from what Dr Lane and the DHSS representatives were saying – that self-sufficiency was expected soon, and would be achieved “within a period of months”.[1331] Indeed after only a couple of months had passed he asked the DHSS if it had by then been achieved. However, there could have been no realistic hope that “efforts … to secure independence of foreign suppliers”[1332] (“self-sufficiency” in other words) could be achieved in the immediate future. Dr Owen told Parliament in 1975 that the Government would fund national self-sufficiency in blood and blood products. By the time the Committee on Safety in Medicine met in July 1983, eight to nine years had passed. Yet England and Wales had failed to achieve what he had promised would occur. No explanation as to why this was had been advanced to Parliament. The redevelopment of BPL was underway by July 1983 but was a long-term project. At the earliest it might be able to increase production of concentrate derived from voluntary unremunerated donors in the UK, which had been made from smaller pools, sometime in 1986.
It would seem therefore that a central figure on the Committee was labouring under a misconception. It was one which was highly material. If it had been right, then after a couple of months or so there would have been no need to continue to import foreign concentrates; the supply issues would have been solved. It is right to note that this (mistaken) view is not, as such, recorded in the (economically worded) minutes.[1333]
As it stands in the minutes, the reasoning is poor. It is an unacceptably casual approach to regard a long-term solution as an answer to a risk of immediate harm, however slowly signs of that harm might begin to emerge. The development of self-sufficiency might provide an alternative source of supply to that provided by importing products, but it could not be an answer to the risk of imported commercial concentrates causing AIDS: that risk would long since have either materialised or been shown to be a misplaced worry.
The appropriate response to what appears on the horizon as a threatening hurricane is to batten down the hatches, and if need be evacuate the coast, rather than leave such steps till later, even though the hurricane may change course and the risk evaporate. Letting it make landfall is leaving it too late.
In summary:
Accordingly, I have concluded that the decision was on any view flawed in the way in which it was taken and in the reasoning that was advanced. There is no doubt – not only in retrospect – that it was also wrong. It was not universally accepted at the time.[1336] Accepting there are dangers of views reached in hindsight, it seems clear that if paramount consideration were to be given to patient safety it should have resulted in a stay on further imports of commercial concentrate, coupled with an increase in local supplies of cryoprecipitate, whilst reserving NHS concentrates for those occasions when their use was truly life-saving, appropriate to provide cover for elective surgery, or used for patients only after careful consideration between clinician and patient as to the balance of risk and remedy.[1337]
It is not asking too much of the Sub-Committee, and relying too much on retrospectivity, to have reached this conclusion. I am fortified in this by a telling exchange between Counsel to the Inquiry and a member of the CSM (but not of the Sub-Committee) which on 22 July accepted the decision of the CSM(B) to make no recommendation about the continued importation of commercial factor concentrates. That member, Professor Sir Michael Rawlins, commented in oral evidence to this Inquiry: “Well, I think if we’d known then what we know about AIDS, that it’s caused by a virus … because at that point it was suspected it was an infectious agent. If we’d known it was caused by a virus, and if we’d known how frequently pool donors in the US … had the virus, then I think we would have done something different. At least I hope we would have done.”[1338] This was the evidence of someone who knew the difficulties and demands of regulation inside out: he plainly did not think it too much to have expected the CSM(B), and in turn the CSM, to have reached a different conclusion if those two matters had been understood.
The first of these – the idea that the cause was a virus – was already regarded as approaching certainty: it was clearly put in Dr Galbraith’s letter (which Professor Sir Michael Rawlins said he would have expected to be put before the CSM(B)), and the second – how frequently pools might contain contaminated donations – was also as good as stated by Dr Galbraith when he spoke of intravenous drug users and male homosexuals being frequent donors. If this second point had not been fully appreciated before the meeting of 19 July 1983 in the US at which the representative of the Pharmaceutical Manufacturers’ Association, Dr Michael Rodell, spoke, it was after that so dramatically clear that it could not be ignored:[1339] that, on average, persons who were paid for their plasma had it collected 40 to 60 times per year. Dr Rodell’s public presentation suggested that at that rate, and given the pool sizes used in the US, as few as four infected persons could contaminate the entire world supply of Factor 8 concentrate (his analysis was confined to concentrates made from US plasma).[1340]
The logical corollary of the FDA’s formal recommendation to pharmaceutical companies of 24 March 1983 that they should not fractionate plasma collected from “the four Hs”was that products produced from “pre-March plasma” should not be supplied, and those already in the supply chain should be withdrawn, on the grounds that supplying them would give rise to an increased risk of transmitting AIDS. Matters in the UK came to a head in early May.
In early May, as recounted above, there was press speculation about whether the Government might decide to ban further imports of commercial concentrates. On 9 May Dr Galbraith wrote his letter advising just this. Coincidentally Travenol wrote on the same day to Dr Walford advising her that “well before”the FDA’s 24 March recommendation, steps had been taken by Hyland to introduce donor screening procedures designed to eliminate high-risk donors.[1341] On the other hand, on the same date the Haemophilia Society planned a meeting with the junior minister, Geoffrey Finsberg, to seek his assurance that there would be no immediate ban on the importation of US blood products.[1342] There were thus voices pushing in the opposite direction to Dr Galbraith and the media.
Professor Bloom was alert to the risk that fractionators in the US and elsewhere who used US-sourced plasma might have stocks of concentrate prepared from plasma collected before March 24, and wrote to Armour to express the worry that if such material was difficult to sell in the US it might be preferentially exported. He sought reassurances from Armour that this would not happen with their products.[1343]
Dr Walford[1344] took the similar view that there were likely to be “large stocks”of Factor 8 concentrates in the US prepared before the 24 March guidelines came into force. She considered it possible that concentrates made from the “safer” plasma might be retained for use in the US while these older stocks were dumped on export markets such as the UK. She asked if there was any way – perhaps by means of new labelling requirements – to prevent this.[1345] Dr Ronald Oliver[1346] responded by suggesting a meeting of officials to coordinate “our activities” so that “we safeguard our own supply position, and if possible obtain Factor VIII from the safest available sources.” He said “Ideally[1347] I suppose we would like to see any imported Factor VIII which is derived from American material to be manufactured after 24 March 1983.”[1348]
It was agreed (by Dr Fowler) that there was a serious possibility that US manufacturers “may try to ‘dump’ pre 24 March 1983 material on the UK market.” He thought, however, that pharmaceutical companies probably had “large supplies of Factor VIII in store waiting for batch clearance by NIBSC and it is very unlikely that material was made solely from post 24 March 1983 plasma.” He nonetheless suggested that “stop orders” might be used; and saw no reason why stating the date of the collection of the source plasma on the labels attached to the products should not be a requirement if it were thought desirable.[1349]
When the question whether new legal restrictions could be introduced to prevent “dumping”was discussed in a DHSS meeting on 3 June 1983, Zoe Spencer[1350] said this would “present significant practical difficulties” and suggested that informal discussions with the companies concerned were more likely to lead to successful control.[1351] Pharmaceutical companies were to be asked to confirm that all future supplies of coagulation factor concentrates to be sold in the UK would be manufactured in accordance with the FDA “Directive”.[1352]
Each firm contacted gave the assurance at the end of June 1983 that “future saleswill comply with FDA guidelines”. However, two (Miles[1353] and Immuno) indicated that Factor 8 concentrates manufactured from plasma collected since March 1983 would not be available until August and September, respectively.[1354]
There remained uncertainty within the DHSS as to the expression “future sales.” It seemed vague. It spoke of sales rather than supplies. Dr Oliver’s minute noted that “in some instances we are still left with the backlog of uncertain plasma or of Factor VIII.”[1355]
About this time,[1356] an information sheet about AIDS prepared within the DHSS was passed to Ministers – Lord Glenarthur and John Patten.[1357] It was said that “The Department’s Medicines and Supply Divisions are endeavouring to ensure that there will be no “dumping” of high-risk plasma products on the UK market and are seeking various assurances from the manufacturers in relation to the quality of their products.”[1358]
Accordingly, when Lord Glenarthur’s office asked for a “fairly full draft letter” to respond to a parliamentary question asked by Baroness Masham, the draft response from the DHSS on 26 July 1983[1359] included the note for his consideration that “we have confirmed with American manufacturers that future supplies of Factor VIII for this country will be manufactured only from plasma collected in accordance with US Food and Drug Administration Regulations introduced in March this year. These were designed to exclude from plasma donation, donors from high risk groups.” This draft – using the word “supplies” rather than “sales”[1360] – was in accordance with the only recommendation which the CSM(B) had made on 13 July.
However, matters then took a rather different turn. This was in the light of developments in the US. On 19 July 1983, the Blood Products Advisory Committee of the FDA considered what to do about products which did not comply with the recommendations it had made to pharmaceutical companies back in March. Since the logical position was that public safety was served by these being observed – or, put the other way round, was at risk if they were not – it might be thought that the FDA would recommend, or require[1361] that product manufactured from plasma obtained before 24 March should be recalled. It did not do so. Instead, the Advisory Committee concluded that:
“a balance must be struck between theoretical risk of the product to recipients against the need for an uninterrupted supply of a life-sustaining therapy … it would be undesirable[1362] to distribute and use a lot of product which incorporated plasma from a donor with a definite diagnosis of AIDS. However, signs and symptoms suggestive of AIDS … would not be persuasive enough to dictate a recall of product … The consensus of the Committee was that the action to be taken for each incident of inclusion of plasma from a donor who might have AIDS into a product pool should be decided on a case-by-case basis.”[1363]
The FDA accepted this advice, deciding that the working policy of the Office of Biologics would be to evaluate the desirability of a recall on a case-by-case basis whenever a donor was found to have AIDS or strongly suspected to have AIDS, taking into account its judgement on the accuracy of the diagnosis, the timing of the occurrence of symptoms in relation to the time of donation, and the impact of a recall based on this.[1364]
It may seem surprising, now, to UK eyes that the FDA had thus not gone so far as to prohibit the continuing distribution of products made from pools to which someone who had AIDS, and had been confirmed to have AIDS, had contributed. It was later to be criticised authoritatively in the US for having failed to do so.[1365]
The result of the FDA meeting was reported by Dr Fowler in a memo of 28 July 1983.[1366]
On 2 August 1983 Mr Charles Wrigglesworth sent an internal memo to Dr Walford, attaching a minute of the US meeting. It asked for Dr Walford’s views on whether further action, if any, was now required in relation to the stocks of pre-March 1983 material; he suggested there was a conflict between the result of the FDA meeting and the recommendation of the CSM(B) of 13 July.[1367]
Dr Fowler was shown a copy of the minute, and took issue with the idea there was a conflict. He argued that there was none:
“Although the first sentence of CSM(B) recommendation (5) states the ideal situation, that only those products made from ‘post-March 1983’ plasma should be used in the UK, it goes on to explain why such a step is impractical because of the effect it would have on essential supplies. Although it is not specifically stated that ‘pre-March 83’ material should be used until adequate supplies of ‘post-March 83’ material are available, this is clearly implied in the full text as being the only practical approach to this difficult problem. The CSM(B) and FDA would thus seem to be in accord on this matter.”[1368]
Dr Walford’s response on 3 August posed a practical question: in effect, was the product to be supplied to the UK (or at least a substantial part of it) just as safe as it would be if it had been made from plasma collected after March 1983 because (as three US companies had asserted) measures at least as good as those requested by the FDA had already been put in place by them well before that date? If so, then the UK “need have no qualms”. However, she too did not feel there was a conflict, because the CSM(B) she thought had “carefully worded [the] recommendation” so as to express the view that “assured supply of material must take precedence over [the] implementation [of its recommendation].”[1369]
Armour were quickly alert to the decision by a “small majority” at a DHSS meeting that included Professor Bloom that the DHSS would permit the use within the UK of factor concentrates produced from pre-March plasma – an internal memo from the UK representative to the parent company suggested it was “vitally important”that Armour sell the product as quickly as possible.[1370]
It transpired before the end of August that the DHSS only had details of precautions introduced by one pharmaceutical company prior to the FDA recommendations in March: it had not pursued information from the others. Mr Wrigglesworth noted that some of the “old” stock was in the UK and that some was still in the US but destined for the UK market. Nonetheless he queried whether any further action was required, given that a US Congressional hearing had accepted the outcome of the FDA meeting.[1371]
The position was thus no longer that there would be “no dumping”. Lord Glenarthur advised the Haemophilia Society: “Although future supplies of Factor VIII both for export and for use in America will be manufactured from plasma collected in accordance with these Regulations [a reference to the FDA recommendations of March], there is still a quantity of stock, some already in the UK and more in America awaiting shipment here, which has been made from “pre-March” plasma. The FDA has recently decided not to ban the use of similar stocks intended for the USA market because to do so would cause a crisis of supply. The same considerations apply here.”[1372]
He expressed this view to Clive Jenkins, general secretary of the Association of Scientific Technical and Managerial Staffs (“ASTMS”), in a letter[1373] which nonetheless began by saying “there is no conclusive evidence that AIDS is transmitted through blood products. Nevertheless we are taking all practicable measures to reduce any possible risks to recipients of blood and blood products”. There is plainly a tension between what he was saying in the letter would happen – that stock manufactured from plasma considered in the US to be a less safe source material would be allowed freely into the UK – and the passage which is highlighted.[1374] Moreover, it was being contemplated that, to accompany a leaflet which was under preparation by the DHSS to advise high-risk groups against donation in the UK it should be said: “Meanwhile, as a safety precaution, the US Food and Drug Administration have introduced special requirements for plasma collection which are designed to exclude … plasma donation donors from high-risk groups.”[1375]
Nothing such as “but products already manufactured from such donors will continue to be imported, distributed and used in the UK for a while” was suggested as a qualification. This should have been made clear in the draft press statement.[1376]
In respect of this letter, Lord Glenarthur was asked in evidence about the draft of the letter prepared for him by civil servants. One exchange (of many[1377]) is particularly revealing:
“Q. I’m just asking about, as it were, the draftsman, thinking it appropriate to put in, in your mouth -- and I know you looked at the letter and approved it, but you did so partially on trust -- saying, ‘We’re doing everything we possibly can’ and then saying, ‘Well, actually, we’re not in this respect because we’re having to accept ‘dodgier stuff’ because there’s no alternative’.
A. Yes, that’s correct.”[1378]
There was a marked change in the approach of those responsible for regulating the importation of blood products between the end of March 1983 and the end of August. Within five months the approach had changed from, in effect, “There shall be no dumping here” to “There shall be no restriction on dumping here.”
The reason for not wanting dumping was the worry that pre-March products would pose a greater risk of AIDS to the patient receiving them than post-March products. It is obvious that the recommendations of the FDA that firms should not accept donations of plasma from those in groups at high risk of AIDS compared to others were designed to reduce the risk of AIDS as far as practicable by aiming to make the sources of plasma safer.
It is thus equally obvious that to impose no restriction on the continued import of products made from such plasma sources put the British public at some additional risk.
Why, then, was there a U-turn? The reasons for it given by Dr Walford and Dr Fowler[1379] relate to a textual interpretation of Dr Smith’s draft on the minutes of the CSM(B) but there is no record of his having been asked if, when he recommended that the use of pre-March plasma be avoided, he was actually countenancing that its supply should continue for as long as there were stockpiles of previously manufactured products.[1380] If he had been asked, as he should have been, there might have been a clearer answer. From what he has subsequently said – that he expected self-sufficiency within a few months – it is difficult to think he would have said this, for there would then be no need to use commercial products, whenever produced.
Their grounds were simply that supply would be insufficient without reliance on the riskier product. The Inquiry has found no convincing evidence that this was the case;[1381] nor that there was detailed consideration of how much “post-March” plasma was available to augment the mix of NHS concentrate and cryoprecipitate which was available for treatment; nor any step “in between” which could have led to discussions between clinician and patient, such as obliging pharmaceutical companies to label, clearly, the date of the collection of the source plasma.[1382] It was however noted that (when looking at August stock levels) that all of Miles’ pre-March 1983 stock and around 70% of the Alpha and Armour stock had been “collected in accordance with companies’ special precautions”.[1383]
Even if the importation of all commercial blood products should not have been suspended for a period, the decision to allow continued importation of pre-March 1983 plasma products is difficult to justify on the evidence available to the Inquiry.
There are two troubling aspects of the chronology of events set out above. The first is this. If the FDA decided not to ban products to which those with AIDS might have contributed, it seems to have been thought that that justified a similar response in the UK. It did not. Further, if any close attention had been paid to what was said at what was a public session in the US on 19 July 1983, the magnitude of the problem would have become apparent. Dr Rodell, a vice president (regulatory and technical affairs) of Armour, said that, on average, persons who were paid for their plasma had it collected 40 to 60 times per year.[1384] His presentation suggested that at that rate, and given the pool sizes used in the US, as few as four infected persons could contaminate the entire world supply of Factor 8 concentrate (his analysis was confined to concentrates made from US plasma).[1385]
This may sound, now, like an elegant plea to ban the products, or at least to ensure the strictest of precautions in manufacture, and measures such as reducing reliance upon regular paid donors and reducing pool sizes.
The context is different. He was arguing the pharmaceutical company position against recall of any infected batch, not simply giving an estimate which would undercut the entire commercial industry. His point was that if a donor was subsequently found to have AIDS, and the product was recalled, the likelihood was that his donations “could easily be represented in as many as 50 plasma pools in one year … 25 to 250 million AHF activity units could be affected, all in various stages of pooling, production and distribution.”[1386]
The comment was made that given the pharmaceutical manufacturers’ estimate of 800 million AHF activity units produced annually by the fractionation industry, the potential for serious disruption of AHF supply described by Dr Rodell “seems quite real”. In other words the need to continue supplying a product trumped any question of whether it was safe or (in effect) a poison.
Quite simply, the presentation suggested that the methods of production used relied on pools which were so big that the products could not be recalled – the system was in effect too big to allow it to fail.
Though it is clear that Lord Glenarthur had been made aware that stocks of product made from pre-March plasma would not be banned in the UK, on supply grounds, and said he considered the decision justified,[1387] it is unclear that he was alerted to the basis of the decision in the US for not requiring recall of products to which a person with signs of AIDS had contributed. A decision to expose those British citizens who might be prescribed blood products to the kind of risk implied by that decision justified specific ministerial consideration. There is evidence that the DHSS knew of the decision by the US authorities (it was, after all, a basis for their accepting pre-March plasma products after having first decided they should not do so).[1388] It is unclear whether the DHSS was told of the detail of the public discussion which had led to it.[1389] On the one hand it would be surprising if an approach as disturbing as that suggested by Dr Rodell was not picked up on: it should have been, given the alarming implications and Dr Fowler seems to have known enough of the discussion to have regarded it as “well aired”. But on the other there is no contemporaneous internal documentation of which the Inquiry is aware which specifically mentions it.[1390] The DHSS as a whole may have fallen short in this, though on the available evidence the Minister himself is not to blame. He could, and should, have been told of the point (if it had been realised within the DHSS), but could not reasonably be expected to discover it for himself.
The second troubling aspect is that although the increased risk posed by “pre-March” plasma products was appreciated, and was now to be taken on supply grounds, nothing was done to try to reduce this risk or help clinicians and patients to identify the additional risk to which they might be exposed. The possibility of imposing a requirement to state the date of collection of the source plasma was contemplated by the DHSS[1391] but this remained only a suggestion. It did not result in the DHSS doing anything. Whether this was because of the “practical difficulties” referred to by Zoe Spencer[1392] or otherwise is unclear. If the DHSS was not going to take action to prevent the importation of pre 24 March products, the least it could do was to take steps to mitigate the additional risk which it was permitting by:
Although Lord Glenarthur wrote letters about “pre-March plasma products” to both the Haemophilia Society and Mr Jenkins of ASTMS, there is no evidence that information about the additional risks were circulated more widely.
It is impracticable for a regulatory body constantly to review all its previous decisions, and whether acting in accordance with them remains appropriate. However, some decisions call out for active review. In particular, where a decision is taken against a background of uncertainty, and events are moving fast, such review is appropriate.
The CSM(B) recognised that its view of risk at the meeting of 13 July 1983 might well evolve. It recognised that knowledge of the cause of AIDS was yet to be firmly established. The issue was not necessarily one of banning the import of commercial concentrates for all time, but rather suspending imports until the balance of risk and advantage became clearer. The members were bound to be aware that what was an epidemic in the US might well become one in Europe, calling for further measures which might involve the variation or revocation of licences. It should have known that its decision was controversial. Its task was not simply to take a decision and move on, without reviewing whether the decision remained appropriate. The decision should have been kept under active review.
The Inquiry has sought to find evidence that there was any such review. Professor Sir Michael Rawlins expressed his surprise there did not appear to have been any.[1394]
The Inquiry has kept looking. Nothing has been found to suggest there was any active review. I conclude it is likely there was none. There should have been.
Is there any evidence of a different (more precautionary) approach being taken to the risk of hepatitis where caused by other products during the 1970s and early 1980s which might shed light on whether the decision-making in respect of Factor 8 products was lacking or not?
There is some.
Thus, in the same year as it declined to recommend the suspension of the importation of products which might carry the cause of AIDS – 1983 – the CSM(B) declined to recommend a licence for a blood product (Immuno’s “Tisseel Kit”) on various grounds, which included that there was inadequate evidence on the hazard of the transmission of hepatitis to the patient:
“Although the use of selective 100 donor pools, as proposed by the Company, would reduce the risks of transmitted infections, there can be no assurance that infecting agents such as Non-A, Non-B hepatitis will be excluded.”[1395]
The approach of regarding it as too great a risk to permit importation of a product because a risk of infection could not be excluded is a very different approach to one which looked instead for evidence that a product actually did cause a serious disease, as was the approach where factor concentrates were being considered.
In another case (this time, in relation to a class of enzyme) the CSM declined to recommend a licence because: “(2) there was a need to consider whether there were alternative treatments for these conditions, (3) there were serious potential adverse effects (particularly hepatitis)”.[1396] The CSM noted that inadequate evidence had been given in relation to safety in respect of the transmission of infection, especially non-A non-B Hepatitis.
These two examples stand out because they show that the CSM had refused to recommend products for licences where there was a risk of hepatitis, and actively looked for evidence as to whether there were alternative treatments.[1397] This contrasts with its approach when considering the potential suspension of the importation of factor concentrates (where there was an acknowledged risk of hepatitis as well as a risk of an infective agent which caused AIDS) and the availability of alternative treatments (where there was a treatment acknowledged to be safer, cryoprecipitate, and no evidence that there was any adequate investigation of its availability).
Towards the end of the 1970s the risks of hepatitis[1398] being transmitted by blood products began to take greater prominence for commercial companies. What seems to have focussed attention in particular amongst the US pharmaceutical companies was knowledge that Behringwerke had developed a product intended to eliminate the risk of hepatitis. It began clinical trials of this product in 1978.[1399] Hyland/Travenol learned of this in February 1979.[1400] In May 1979, they heard that the clinical trials of the Behringwerke product were almost complete, and the results seemed promising.[1401] It prompted them into action. Not only Hyland, but Cutter,[1402] Alpha and Armour all appear to have made a determined effort to inactivate their own products. More about this is said in the chapter on Viral Inactivation.
Three companies developed a heat-treated product and had sufficiently successfully conducted clinical trials by 1982[1403] to apply in that year to the FDA for a licence. This was followed by a fourth company making applications in 1983.[1404]
In March 1983 the FDA granted a licence for Hemofil-T; in January 1984 it then licensed the Armour product and the Cutter pasteurisation product, followed by Cutter’s dry heat product in February 1984.[1405]
Applications followed to the Licensing Authority in the UK in 1983 in respect of Hemofil-T and Behringwerke’s product “Haemate P”. In 1984 they were followed by an application from Armour seeking a licence for heat-treated Factorate.[1406]
Both the application in respect of Hemofil and that in respect of Factorate were refused.[1407]
So far as Hemofil-T was concerned the CSM(B) said it was unable to recommend a product licence. The grounds included that “justification should be provided for the inclusion and choice of the heat treatment step.” The CSM(B) remarked that “Promotional letters making unjustified claims on improved safety margins in respect of infection and AIDS were seen by the Sub-Committee and strongly deprecated.”[1408]
The pharmaceutical assessor[1409] noted that there was anecdotal evidence that the heat treatment step had been “included to minimise the chance of transmission of AIDS: but, this assumes AIDS is a viral mediated infection. There is no evidence to confirm this.”[1410]
The medical assessor[1411] observed “The company have applied to vary their product licence for a conventional FVIII concentrate, by the addition to the manufacturing process of a heat treatment step. No reason is given for this, but it may be assumed that they have a reason because the proposed treatment destroys about 20% of the coagulant activity yield.” However, he then suggested that the reason was to be found in promotional letters sent by the company to regional transfusion directors and specialists in haemophilia. These letters promoted heat-treated Hemofil as being less likely to transmit viral infection, “with particular reference to hepatitis B, non-A non-B hepatitis and possibly AIDS.”[1412]
Given the references – to the “unjustified claims … in respect of infection and AIDS”, the “anecdotal evidence” and the promotional letters – a reason for including a heat treatment step in the process seems clear, even if not formally articulated by the manufacturer. Yet the application was rejected.[1413]
It was another year before Hyland/Travenol reapplied for a licence for the same product. By then it had been invited to apply using an abridged application process. In the meantime Hemofil-T had been licensed for sale in West Germany, Canada, Spain, Sweden, Belgium, and Ireland as well as the US and a licence to import it had been granted in the Netherlands.[1414]
The only other application to the UK Licensing Authority in 1983 was made by Behringwerke. A licence was granted, subject to a number of conditions. One was to provide satisfactory information on the heat treatment process; another not to make claims that transmission of Hepatitis B and non-A non-B Hepatitis had been “excluded”; and a third that there should be no reference to AIDS except to warn that blood products may transmit the syndrome.[1415] Of interest in the medical assessment is the view by the assessor, Dr Fowler, that “All anti-haemophilic factor (“AHF”) preparations can cause hepatitis, and most haemophiliacs will sooner or later get hepatitis. Some will die of it. Clearly anything that improves this situation would be desirable but it is important to distinguish which form of hepatitis poses the greatest threat.” He went on to identify the “greatest threat” as being non-A non-B Hepatitis which “is thought to account for ninety percent of all hepatitis due to blood and blood products and to be more likely than HB [Hepatitis B] to cause chronic liver disease.” He concluded that it was probable that Hepatitis B would be less likely with the heat-treated product than with comparable untreated products.[1416]
Although the licence was granted (in February 1985, though the recommendation had been to accept it with conditions in March 1984) the product was not introduced onto the UK market before 1987 for commercial reasons.[1417]
The third application was from Armour. It was declined in July 1984 on the grounds of safety, quality and efficacy.[1418]
Thus far the Licensing Authority had rejected applications to license heat-treated factor concentrates (with the exception of Behringwerke).
The situation changed on 26 October 1984. On that date, the CDC published in the MMWR series a report on their study conducted on a heat-treated product produced by Cutter. It recorded that the preliminary evidence of the effects of heat treatment was that it reduced the potential for transmission of the AIDS virus in blood clotting factor concentrate products. It suggested that the use of non-heat-treated concentrates should be limited thereafter.[1419]
Things moved quickly. Within a month Dr Smith, chair of the CSM(B), reported that heat treatment appeared to abolish detectable infectivity of the AIDS virus.[1420] As a result, the CSM requested[1421] that the Licensing Authority invite the companies concerned to make early applications for variations to their licences to permit the distribution and sale in the UK of Factor 8 products made by processes including a dry heat-treating step.[1422]
Four days later the Licensing Authority wrote to pharmaceutical companies encouraging them to use a dry heat treatment process, and to make early (abridged) application for a new product licence for concentrates manufactured by using it.[1423]
A summary of the way heat-treated products had been dealt with by the regulator since the first application was set out in an internal Cutter memo of 30 November 1984. It read:
“AIDS has finally come to the United Kingdom with a force that has caused a virtual panic in the Department of Health. For one year this department has blocked every application for registration of heat-treated factor VIII products [apart from Behringwerke, albeit with conditions, though it did not enter the market] and now in the space of one week they are in a panic responding to the newspaper demands for action concerning the AIDS risk to hemophiliacs. The action by the Department of Health comes after the announcement in the Sunday Mail that 2 hemophiliacs have died from AIDS.”[1424]
The summary then set out five headlines from 25 November, and one from 20 November, from The Mail, The Times, The News of the World and The Observer, before continuing: “Following these headlines the Department of Health has advised Cutter that every action will be taken to grant us registration by early December.”
The summary is both concise and correct so far as evidence available to the Inquiry goes. (Though the Inquiry has no confirmatory evidence of the “early December”date having been given, it has none to the contrary).
For reasons which are unclear, despite apparently telling Cutter that a licence would be approved in December, a licence was not granted until February 1985. In February 1985, but not before, the heat-treated products of Baxter, Alpha, Armour, Cutter and Immuno were all licensed.[1425] Quite why it took this time given the urgency of the invitation remains unknown. However, it did not stop clinicians taking advantage of the products (technically on a named patient basis).
It was not until March 1986, amid concerns that the use of Factorate could still give rise to infections despite heat treatment, that the DHSS collected data on the ability of the products to inactivate HIV.[1426]
It is for an applicant for a licence to set out their case for being licensed. It is not for a Licensing Authority to make that case for them. If, therefore, there was good reason for introducing a heat treatment step into the process, it was in the first place for Hyland/Travenol to state it. However, by 1983 the CSM(B) had already determined (at its meeting of 13 July 1983 considered above) that the cause of AIDS was probably viral. There was an obvious reason, known to the Committee, why a manufacturer would wish to include a heat-treated step which resulted in a lower yield of Factor 8 activity per litre of plasma. The pharmaceutical assessor quoted anecdotal evidence that the step was intended to minimise the chance of transmission of AIDS. The medical comment noted that no reason was given, but then went on to describe the reason as being that heat treatment made the product less likely to transmit viral infection, in particular the hepatitis viruses and possibly AIDS. In itself the decision was justifiable, and not unreasonable given a lack of detail of the methods being used to kill viruses and the uncertainties of their success.[1427] However, given the material available to the Committee it would have been a simple matter[1428] for the Committee to write and ask Hyland, prior to final consideration whether to accept or refuse the application, why the heat treatment step had been introduced.
Nonetheless, the medical assessor was also concerned that the introduction of the heat-treated step involved the loss of 20% of coagulant activity. This meant that some of the Factor 8 would be degraded, and might then have a “toxic potential”.[1429] There was a general concern that a new process might bring with it new risks to the patients receiving the product. Taken in isolation this would be a real risk.
The decision not to recommend a licence was reached in a wider context of which account could have been taken. It was made in September 1983. This was only two months after the decision had been taken by the CSM(B) on 13 July, endorsed by the CSM later that month, not to recommend suspension of the importation of factor concentrates. That should have been kept under close review. As part of the discussion before the CSM(B) there had been positive reference to the likelihood of blood products being heated to protect against AIDS, assuming AIDS to be virally caused: here was an application in respect of just such a product, it might have been thought. It was also already known by September that on “grounds of supply” untreated products coming from the US made from “pre-March plasma” were to be permitted to enter the UK market, contrary to earlier assurances that they would be excluded because they were more likely to risk AIDS. It was also clear that the number of AIDS cases amongst people in the UK who did not have haemophilia was continuing to grow exponentially. Finally, the reality of the risk of transmission of the cause of AIDS to people with haemophilia by blood products had been highlighted by the death of the first person with haemophilia in the UK. He had most probably died in consequence of receiving commercial factor concentrates.
As Professor Sir Michael Rawlins observed, safety often involves a balancing exercise. Here it was the balance between the possible, but unknown, adverse effects of heat treatment against the highly likely, though not yet certain, fact that blood products transmitted a fatal disease. The balance did not fall against Behringwerke’s product, despite the fact that the yield was far less than that claimed for Hemofil-T, so the drawing of this balance does not appear consistent even prior to the events of autumn 1984.[1430] However, once those events occurred – the endorsement by the CDC of the effectiveness of heat treatment, and adverse press comment – the balance was held not only to favour licensing but effectively to fast-track it (despite all the reservations which had led to Hyland’s application failing a year earlier).
There is an apparent inconsistency between the approach taken in late 1984 to that taken in late 1983: the explanation is, however, the impact of growing information about the viral cause of AIDS, growing concern about its effects on society transmission, and a growing need to stop further progression in its tracks: coupled with an appreciation after October 1984 that (dry) heat treatment was likely to be effective.
When the approach of rejecting the applications to market heat-treated products in the early 1980s (on grounds of safety) is compared with the approach in the 1970s to licensing products which were both known to transmit hepatitis, and thought likely to do so to a greater extent than domestic coagulant therapies, there is however an irony. Hemofil and Kryobulin were first licensed in 1973 despite being less safe than products already in use. The heat-treated versions were rejected on grounds of safety, despite being aimed at reducing the risks of transmitting disease.
Finally, there is no explanation why, when Cutter was assured (it appears) that the aim was to have its product available by December 1984, licences should have waited until February, at least in the cases of Hyland (for Hemofil) and Cutter (for Koate) who applied in September and November of 1984, respectively. It is not unreasonable for applications made by Alpha and Armour in January 1985 not to have been granted before February,[1431] and I am not prepared to say that it was unreasonable that there should be delay in the grant of a licence for the Kryobulin TIM 2 product in respect of which Immuno made an application in December 1984.[1432] If, however, the applications to resubmit a licence were an invitation to push at what was effectively an open door, then, given that the decisions on them had consequences for safety at least the first two could have been taken faster.
The Medicines Commission was responsible for directing the British Pharmacopoeia Commission which published the British Pharmacopoeia.[1433] This sets out, product by product, the standards for human medicines and formulated products.
In a publication in July 1977, entitled The Control of Medicines in the United Kingdom, it is said that “A central theme in the British approach to the regulation of the marketing of medicinal products is a conviction that controls before marketing are not sufficient. However extensive the precautionary animal work, some effects may not be detectable until a large number of patients have received the drug … Great importance is attached to the monitoring of possible adverse reactions to medicinal products.”[1434]
For that purpose, the publication noted that the CSM maintained a Register of Adverse Reactions to which confidential reports about individual patients were made on a voluntary basis by members of the professions, usually on a specially designed “Yellow Card” issued to all doctors and dentists. Other sources – the Registrar General, the pharmaceutical industry, coroners – also contributed. 80 doctors were engaged part-time to investigate reports of individual reactions at the request of the CSM; summaries of the information obtained were provided routinely to those who reported adverse reactions, and “are available for certain classes of authorised person who may enquire about them”.[1435] No information was released which would identify a patient without written permission. This “Yellow Card scheme” has become very well known, which is part of its general success in alerting the authorities, the medical profession generally, and patients to potential problems.
Other means of communicating with the professions (and later the public) were through leaflets as to adverse reactions; to provide “Dear Dr” letters from the chair of the CSM; produce leaflets on “Current Problems”; and publish articles in medical journals.[1436]
The Yellow Card scheme[1437] has limited relevance to the risks of hepatitis amongst people with haemophilia, since the risk was already known to practitioners, and it is more likely to be used for reactions which are closely linked in time to the causative injection or transfusion. Chronic hepatitis, for instance, may first show itself with relatively unspecific symptoms, easily attributed to other causes and by the time the problems are becoming understood as serious, and the patient’s condition worsening, are not likely to trigger a Yellow Card since so long will have passed between the effect now manifesting itself and its cause several months or (more probably) years earlier. Nonetheless, so far as acute hepatitis[1438] is concerned it might suggest that certain products appeared to produce more infection than others. Similarly, AIDS symptoms were likely to arise some time after the injection/transfusion which caused them to develop, and it might not be easy for either patient or clinician immediately to have spotted that there was a possible relationship between the two which would justify an adverse reaction report. In those cases where the patients themselves suspected that there may be a link, the Yellow Card scheme was of little use to them between 1970 and 1995 because reporting was limited to medical practitioners during that period.[1439] Between 1970 and 1995 there were 144 Yellow Card reports relating to blood products,[1440] 63 of which occurred between 1977 and 1981. Approximately half did not relate to reactions involving the blood and lymphatic system, the liver, or “infections and infestations”.[1441] None related to HIV or AIDS.
There was an established process of investigating reports of serious adverse reactions to see if there is a link between effect and postulated cause, and whether to notify the professions of it.[1442]
After hearing from Professor Sir Michael Rawlins, the Inquiry sought evidence of the information (if any) which was disseminated regarding the risks of factor products. The reply on behalf of the Medicines and Healthcare products Regulatory Agency (“MHRA”) states that no record exists of any communication between 1970 and 2000 in respect of the risks of factor products.[1443] There was some (limited) evidence that hepatitis was reported through the Yellow Card scheme after the use of factor products. However, there is no evidence (despite the efforts of the MHRA to trawl through potential sources) that the full investigative process which might then have followed, to understand and if necessary report the risks, did so. This was despite the fact that on the evidence hepatitis is a serious condition when it occurs. I am bound to conclude that there was no such investigation.
In conclusion, the CSM had as one of its functions the job of communicating particular risks of medicinal products to professionals. However, it made none in respect of the risks of hepatitis or AIDS from blood products, though there was ample material which might have caused it to do so or to investigate further. There is one qualification to this. The British Pharmacopoeia did contain references to named commercial factor concentrates risking hepatitis if they were administered. However, in the years that most mattered in protection of the public (1983-1985) nothing appeared about the risks that AIDS might result from their use.[1444]
So far as regulation of factor concentrates is concerned, the system failed the British public. The failures were in how the system was operated, rather than being inherent in the system itself. They were compounded by a lack of openness in the critical period of interest to the Inquiry in respect of blood products: that was almost certainly because the committees involved understood this to be required by statute. A more open approach would have gone a long way to ensuring that those who were to receive products knew clearly of the risks to their health. The central failure however was not to prioritise safety.
This chapter examines the long-standing government policy of self-sufficiency in blood products. It assesses the various factors which contributed to the failure to achieve self-sufficiency for England and Wales earlier, including the lack of forward planning, the delay in redeveloping BPL and the failure to arrange for plasma from England and Wales to be processed in Scotland.
1962 “make and mend” extension to BPL.
1965 Ministry of Health and SHHD agree to build PFC, which will fractionate plasma from northern regions in England.
1967 Dr Biggs calls for the “organisation, apparatus and buildings” to enable greater product of domestic concentrates.
January 1973 Dr Maycock urges DHSS to “have constantly in mind the need to develop our own sources in the UK transfusion services.”
20 March 1973 first meeting of Expert Group on Treatment of Haemophilia sets initial aim of 250,000 donations to be used for factor concentrate.
January 1974 MRC working party endorses range from 547,540-720,000 donations.
24 December 1974 DHSS writes to regional administrators that achieving self-sufficiency is “of the greatest importance”.
22 January 1975 Dr Owen states the government’s commitment to self-sufficiency and announces allocation of additional finance.
January 1976 Dr Bidwell estimates need for between 970,920 - 1,213,650 donations; similar estimate advanced by Dr Biggs to Expert Group in May 1976.
August 1977 Dr Lane unwilling to enter into long term agreement to have plasma fractionated in Scotland.
December 1977 Report of Working Group on Trends in Demand for Blood Products concludes that major government investment is required.
December 1978 Roland Moyle tells Parliament self-sufficiency not yet achieved.
April 1979 Medicines Inspectorate inspects BPL and produces damning report in July
December 1980 ministers instruct officials to begin planning for new BPL.
October 1981 90% of the blood products used in Scotland are manufactured at PFC.
11 November 1982 Treasury approves redevelopment of BPL (completed in 1987).
Dr Ethel Bidwell director, PFL (1967 - 1981)
Dr Rosemary Biggs director of Oxford Haemophilia Centre (1970 - 1977)
Thomas Dutton joint secretary of the Central Committee for the NBTS
Dr Richard Lane director, BPL (1978 -1990)
Dr William d’A Maycock consultant advisor on blood transfusion to CMO and director, BPL (until 1978)
Roland Moyle Minister of State for Health (1976 - 1979)
Dr David Owen Minister of State for Health (1974 -1976)
Dr Gerard Vaughan Minister of State for Health (1979 - 1982)
Dr Sheila Waiter joint secretary of the Central Committee for the NBTS
John Watt director, PFC (1967 - 1983)
BPL Blood Products Laboratory (Elstree)
PFC Protein Fractionation Centre (Edinburgh)
PFL Plasma Fractionation Laboratory (Oxford)
The starting point is that, in overview, product made in the UK from UK-donor sources was safer [1445] than product made commercially from plasma purchased from donors. If the UK had become self-sufficient in the production of factor concentrates, NHS treatment using them would have been safer. The likelihood is that significantly lower numbers of infections with HIV would have followed. The likelihood is also that there would have been fewer infections with Hepatitis B and non-A non-B Hepatitis (Hepatitis C as we now know it).[1446] The sad fact is that despite the policy of governments ever since the end of 1974 being to achieve self-sufficiency in the production of blood products to treat haemophilia throughout the UK, this was not achieved in England and Wales until after 1990, although it was substantially achieved in Scotland at a much earlier stage. This chapter examines the causes of this, looking at each of the factors set out below in turn, except for finance which is threaded throughout the narrative.
The story this chapter tells is one of missed opportunities: a fractured and uncoordinated response to problems; a failure to plan in time for anticipated need; a disinclination to accept changes to methods of collecting and using blood; as well as an overenthusiasm amongst treating haemophilia clinicians for a newly developed treatment without significant regard to the risk, coupled with an apparent acceptance that much of that risk was inevitable. It is a story, too, which focuses on manufacturing products on a large scale in facilities which (save in Scotland from 1975/76 onwards, and in England from 1986/87) had never been designed for that purpose. Pervading it is a sense that patient safety took second place to cost, at times, and “efficiency” of production, at other times.
It is difficult to avoid the conclusion that Dr Robert Cumming, who was Dr William d’A Maycock’s Scottish counterpart overseeing the fractionation plant in Edinburgh,[1447] had it right when in 1975 (having retired) he wrote a paper on The Voluntary Blood Donor: “It is the author’s opinion that those inadequacies which exist in modern developed countries are entirely the fault of the organisation of the Service ... One of the important features of a successful voluntary blood donor system is forward planning.”[1448] He seems to have been clear-sighted about demand and how to meet it.[1449]
After the National Health Service (“NHS”) began operating on 5 July 1948 the supply of blood was almost entirely from domestic sources, but the supply of blood products to patients can be traced through two separate chains: domestic and commercial.
The domestic supply has origins that can be traced back to the start of the Second World War, and to arrangements (described in the chapter on Blood and Transfusion) which were inherited when the NHS first began. Commercial supply involved blood products (mainly clotting factor concentrates) being imported for use for those who required them.
The two chains remained largely distinct, though they could overlap in some respects. Principal differences between the two were:
Until the mid 1960s there was no easily available or easily usable means of remedying a shortage of clotting factor in a person’s bloodstream. Cohn fractionation offered a way of separating blood into its constituent parts, and opened the possibility of using that part which was responsible for helping blood to clot without the far greater volume of blood from which it was separated.[1457]
Early attempts to adapt the methods of Dr Edwin Cohn to producing large quantities of clotting factor concentrates were hampered by technical difficulties, until the mid 1950s when these were overcome by researchers working independently in England, Sweden, France and Scotland.[1458] A product information sheet for the Scottish achievement dated 27 April 1954 recorded that it had ten times as much Factor 8 activity as fresh frozen plasma (“FFP”), and that “A similar fraction is prepared by ether fractionation (Kekwick).”[1459] This was a reference to Dr Ralph Kekwick and Dr Peter Wolf’s work at the Lister Institute (at the Blood Products Laboratory (“BPL”), in Elstree).[1460] It was freeze dried. Their product was supplied in small quantities to Lewisham and Hammersmith hospitals in London and to the Radcliffe in Oxford. By 1959, 75 patients had been treated.[1461] The UK had thus become an international leader in the field as early as 1957, and at that stage technologically ahead of the US.
There were three blood product manufacturing units in the UK: in Elstree, which became BPL; in Oxford, the Plasma Fractionation Laboratory (“PFL”); and in central Edinburgh (eventually in Liberton, a suburb), the Protein Fractionation Centre (“PFC”).
BPL was a post-war 1954 building. It had been planned initially as a civil defence project to prepare freeze-dried ultraviolet light irradiated large pool plasma. In the course of planning, this goal was abandoned in order to return to freeze-dried ten-donor small pool plasma.[1462] Fractionation of plasma was not a primary objective. As planned, the building had no space to accommodate this. When he retired as the director of BPL in 1978, Dr Maycock described how it had been extended in a “make and mend operation” in 1962.[1463] It was not until 1965 that planning for a 1972 extension, which then followed, contemplated accommodating the fractionation of plasma on any scale. This was a necessary step in producing clotting factor concentrates, though the main reason for the expansion at the time was to produce more immunoglobulin to prevent rubella in pregnancy, following an outbreak.[1464] There was also a slowly rising demand for albumin.[1465]
Dr Maycock described how even then the production facilities were not designed for the task nor large enough. He thought it generally took at least four to five years from the planning stage for a production facility to come on stream.[1466] Given his view, which he expressed with some force in the final report of BPL (for which he was responsible as its director), it is probable that he would have expressed it to the Chief Medical Officer (“CMO”)[1467] of the day. He is likely to have pressed the Government to provide for suitable production facilities, rather than the one he ran, which was not designed for the task, nor large enough. There are signs that he did so throughout the early 1970s, especially when – as will be seen below – he allied himself to calls for self-sufficiency, greater provision of plasma to achieve it, increased production, and for collaboration with Scotland to achieve this on a UK-wide basis.
Whilst the production unit in England was “make and mend”[1468] when extended in 1962, the Scottish Home and Health Department (“SHHD”), faced with a growing demand for a range of blood products,[1469] drew up plans to build a completely new unit in Edinburgh processing 1,500, and if necessary up to 3,000, litres[1470] of plasma per week, to produce antihaemophilic globulin (“AHG”)[1471] as well as other fractions required for therapy. It was also to have research and development facilities.[1472] In 1965 the Ministry of Health made a formal agreement with the SHHD that the new unit in Edinburgh would fractionate plasma for the NHS using plasma collected by four English regions – Newcastle, Leeds, Manchester and Liverpool.[1473] This history, and the way in which through Westminster the necessary finance was made available, suggests a forward-looking interest was taken at that time to updating and renewing production facilities so as, between them, to serve the UK as a whole.[1474] It proved lacking after this.
The planning for the Edinburgh unit is all the more striking a provision for the future because it happened before a means of producing cryoprecipitate for therapeutic use was developed.[1475] Estimates of future annual needs for haemophilia therapy were already being predicted by a Working Party on AHG,[1476] which favoured a central laboratory for preparation of AHG.[1477] This demonstrates that there was developing use of AHG prior to the discovery of a way of using cryoprecipitate therapeutically, reported in the next year by Dr Judith Pool. It explains why, when new premises at Liberton were planned for PFC in Scotland, it was decided that it should be capable of producing AHG in quantity.[1478]
Antihaemophilic fraction (“AHF”)[1479] was by 1965 produced as a freeze-dried product, to be reconstituted with water, one unit giving 6-8 hours of Factor 8 activity (at least in Scotland). It was then made from six donations (approximately equivalent to just over one litre of freshly prepared plasma to which an anticoagulant had been added).[1480]
Cryoprecipitate[1481] could by contrast be easily prepared. It did not need a central production unit to make it. It was far richer by volume in Factor 8 than plasma had been, and thus could be administered in smaller, more concentrated doses. It was a game changer. By April 1967 it was being said in The British Medical Journal (based on a paper presented in September 1966) that cryoprecipitate was an “extremely valuable therapeutic material” and that from “many points of view it is the therapeutic material of choice.”[1482] Dr Peter Jones said in a publication in The Lancet on the same day that cryoprecipitate was now “the method of choice in treating bleeding episodes” and that “concentrated human AHF should be reserved for patients in whom haemostasis presents particular difficulty.”[1483]
Blood product usage now focussed upon cryoprecipitate: and thus, so did production. For nearly ten years cryoprecipitate was the major therapeutic material used for “on demand” treatment of bleeds. Centralised production facilities were largely unnecessary to provide it, since it could be made locally[1484] with relative ease. AHF was used in small quantities, in circumstances where clinicians felt the volumes of cryoprecipitate required to ensure a reasonable level of clotting would be too great, or where the use of cryoprecipitate[1485] had provoked an immune reaction.
During 1967 a haemophilia centre was established at the Churchill Hospital in Oxford. This was in succession to a coagulation research laboratory which had been operated by the Medical Research Council (“MRC”). The Centre had three elements to it: a clinical section, a coagulation research laboratory, and a plasma fractionation laboratory.[1486] The Lister Institute, which already administered the Blood Products Laboratory at Elstree, agreed to administer this Plasma Fractionation Laboratory as well, “because of the similarity of the work of the two organizations and the benefits which would accrue from their close association. The work of PFL was to be concerned with the separation and purification of coagulation factors for clinical use.” It thus became a third production facility of importance for people with haemophilia in the UK, alongside BPL and PFC (Liberton). It became operational in mid 1968.[1487] It was always much smaller than Elstree or Liberton. Much of its work involved the production of Factor 9 concentrates. In broad terms, the UK was then self-sufficient in meeting Factor 9 needs, and remained so until products sourced from British donor plasma ceased being used because of the threat of vCJD[1488]
The AHF as first produced by PFL and BPL was not ideal for home therapy since it was “poorly soluble, of low potency and specific activity.”[1489] Home therapy was thus pursued only to a limited extent at this stage: it was feasible with cryoprecipitate, but not as convenient.[1490]
There was a change in the method of preparation of AHF after 1970, first at PFL, and later at BPL.[1491] Thus far, AHF had been manufactured from liquid plasma. The base material had not been frozen. It thus had usually to be sourced from local donors, and used fresh. A change from the Blömback to the Newman method of preparation involved a change to the use of frozen plasma, from which cryoprecipitate could be obtained so as to form the basis for the further concentration of the Factor 8 it contained.[1492] This opened up more possibilities of larger-scale production.
It became apparent during 1967 to Dr Rosemary Biggs, who was at the Oxford Haemophilia Centre, that pharmaceutical companies in the US were planning to produce large quantities of freeze-dried concentrated AHF. She regarded concentrates as of prime importance. In a letter of considerable foresight to the CMO, she said: “I have estimated, on the basis of our practice,[1493] that a minimum quantity of these concentrates required at present is the product from about 50,000 donors a year. When all of the patients come for treatment more would be needed. The supply of plasma, as starting material for fractionation would, I think, be no problem since the use of the red cells can be organised.”[1494]
She estimated that product from more than one million donors a year would be processed on a commercial basis in the US, adding:
“When this material comes on to the market we shall be obliged to buy it at a very high cost for our patients unless the English shortage can be remedied.
In this country we have pioneered this treatment, we have the personnel who know how to make the products, we could easily have enough plasma to serve as starting material. It would seem to me a great pity if we cannot make our own material in this country for lack of the organisation, apparatus and buildings in which to work. The purchase of the finished products in the United States will undoubtedly be very costly … a large amount will be made by commerical [sic] enterprise and on sale. On present prices a course of anti-haemophilic treatment for one emergency purchased from the United States, would cost $1,500 to $5,000. Surely it would be less costly to us to do everything to expedite the manufacture of these fractions in England and in particular to accelerate as much as possible the new fractionation buildings at Elstree and in Edinburgh.”[1495]
As to “new fractionation buildings” in Edinburgh, at this point the plant was still at the design stage, and was being purpose built for large-scale fractionation. It could not be expected to be on stream for a while.[1496] By the new fractionation building in Elstree, Dr Biggs presumably had in mind a further extension to the then BPL, which was completed in 1972.[1497] The estimates for Factor 8 concentrates and albumin concentrate on which the plan for the extended facilities were based were, in Dr Maycock’s view, “totally inadequate.”[1498] The limited size of the site imposed constraints; and yet Dr Maycock complained that “reductions in floor space were nevertheless imposed by the Department [of Health].”[1499]
In short, an adequate state-of-the-art facility was planned for Scotland, and a “make do and mend” solution for England, at a time when little space might have been needed to produce AHF – unless, that is, there were going to be rapid improvements in the quality of AHF, its solubility, its ease of production, and the ability to scale it up for production in large quantities. Developments in all those respects were, however, certainly foreseeable. And in the near future.
By 1967, as Dr Biggs’ letter shows, the message that more space for production might well be essential was slowly becoming clear, albeit after the initial plans for both the “extension” at BPL and the new building of PFC had been determined.
The force of her message was demonstrated particularly after 1969 when a pharmaceutical company, Immuno started to market Kryobulin.[1500] This was first used in the UK in 1970.[1501] Its distribution within the UK was not, as yet, licensed. However it could be used by clinicians on a named patient basis.[1502] (It was not until December 1972 that an application for a licence to distribute Kryobulin in the UK was made). A rival US product – Hemofil – was also used on a named patient basis. Their efficiency in use, easier solubility, and (plainly) the fact that they were the result of large-scale production, might have indicated that the UK would need to follow suit if those products were not to dominate the market.
Dr Maycock appears to have foreseen a need for more substantial production facilities to be provided. So too did Dr Biggs. At this stage, in the late 1960s to the turn of the 1970s, public money was more freely available than it was later to be. An opportunity was missed.
Nonetheless, as the chapter on Regulation of Commercial Factor Concentrates reports, by 1973, the year in which both products were licensed, 80% of treatment was by cryoprecipitate, with the balance being made up of factor concentrates, largely of NHS manufacture. Between 1974 and 1975, for the first time, the use of commercial concentrate exceeded the use of NHS concentrate so far as the consumption of concentrates was concerned: but two thirds of the total product used for factor replacement was still cryoprecipitate. The two commercial products licensed in early 1973 thus did not immediately form a major plank of replacement therapies.[1503]
In summary of the story thus far, before Hemofil and Kryobulin were licensed in 1973 there was a mixture of inadequate, out of date, and struggling manufacturing facilities in the UK, aiming to cope with the manufacture of a new product for which they had not been designed. There was bound, inevitably, to be a passage of some time before new, effective facilities could be made available (at PFC Liberton in Scotland), intended to provide for roughly half the needs of mainland UK,[1504] which could match the rapid developments in, and the acceptability in use of, concentrates provided by commercial fractionators in Europe and the US, and which could fulfil the desire of some leading clinicians[1505] to facilitate home treatment for people with severe haemophilia. But there had been a failure to recognise that BPL would either need very considerable extension, for which there seemed to be little if any space, or complete redevelopment, if necessary on a site elsewhere than Elstree.
It was this licensing, and its consequences, that led to further calls for self-sufficiency.
A simple definition of self-sufficiency in blood products is producing from a country’s own resources enough factor concentrate to meet clinical need without having to import any.[1506] This is the broad definition adopted for the purposes of this chapter.
It may seem simple. However, even expressed this simply, it is not. Clinical need is not easy to identify objectively. Who is to judge? In the treatment room, one doctor may think that a condition is best treated by a conservative approach, whereas another clinician might think that surgery is required. If the first were asked “does the patient need surgery?” their answer would be “no”. Depending upon the degree of confidence of the second, their answer might be “of course they do”. It might, however, be “I think it is probably safer/better to have surgery, even though it is not essential.” These are three very different responses to what represents the patient’s clinical need.[1507]
If one asks the same question of the hospital administrator seeking to save costs in one area so that the money might be spent in another to make the most of limited resources, they might answer by expressing doubts that the patient needed surgery. At the time of principal concern to the Inquiry, there were regional health authorities. If asked what the patient needed, what would their view be? They might see their task as being to prioritise the “needs” of each patient as best they could. This would involve a balance with other groups of patients who might seem more deserving to that authority than those groups did to other regional authorities. It might have the result that in one region a patient would be seen to have certain “needs” for more extensive treatment, whereas in another region they would not “need” it.
In short, “need” involves questions of perspective. The individual patient’s perspective may well be different from that of his treating clinician, and in turn from the administrative bodies. What patients think they need (always of critical importance) may reflect very different considerations again, both individually and as a group.
In the context of organising the supply of blood and blood products the “needs” of the population as a whole had to be determined. By reference to what standard? Here, views differed.[1508] It was seen by some that people with haemophilia needed to be able to live a “normal sedentary lifestyle.”[1509] Others had further ambitions: that having the condition of haemophilia should not inhibit anyone having as active a lifestyle as they wished. The World Health Organization (“WHO”) defines health as not simply the absence of disease, but a state of complete physical, mental and social wellbeing. At the other end of the spectrum, it could be considered that “the need” of patients was relief from life-threatening bleeds.
“Demand” tends to be equated in common parlance with “need”. But it is not the same, though demand for a product may over a period of time[1510] evolve into the product being seen as “necessary”, or (to use another word) “needed”. Dr Terence Snape pointed out in his evidence that prescribing choices in England and Wales (ie the choices that would be reflected in demand) were being formed between 1973 and 1978 “when imported commercial factor VIII was opportunistically filling the gap left by BPL’s failure to supply” and commented that therefore “it may be no surprise that clinicians … would continue to exercise that choice well into 1982/3”.[1511] In short, the convenience in treatment which Factor 8 concentrate offered, which led to its increasing use for home treatment, and the plentiful supply of concentrates from the US to fuel this, led to an increased demand for further supply, and made it more likely that factor concentrates were seen as necessary, not merely as highly desirable. It became, in his view, a case of supply creating demand, which then in turn created a need for increased supply.[1512]
This view, expressed in evidence by Dr Snape, was echoed in closing submissions to the Inquiry, arguing that the fact of licensing importation of foreign concentrate itself led to a demand for it to be available.[1513] The submissions were to the effect that if no licence had been granted there would have been a greater emphasis on producing more easily usable factor concentrate from the UK’s own resources: there would have been a greater urgency in pushing ahead with developing state-of-the-art production facilities.
If the regulator (ie the Licensing Authority) had rejected the applications made to it in 1972 for the licensing of Kryobulin and Hemofil M such that their licensed distribution would not have been permitted in 1973, it would have been on the basis that they posed too great a risk of transmitting hepatitis. This may then have led to a greater emphasis by those commercial companies on research into viral inactivation. It seems likely that, whether or not such steps were taken by those who wished to enter the market to compete against an apparently safer domestic product, greater impetus would have been given to developing a modern production facility in the UK.
The facts are that freeze-dried concentrates – whether commercial or domestic in origin – became seen as generally necessary by the end of the 1970s, when they had begun the decade by seeming desirable for the convenient advantages they offered for particular cases. The fact was also that cryoprecipitate prevented the worst of serious bleeds, could be used at home, though with some difficulty, and was responsible in itself for a significant improvement in life expectancy. It met the needs for treatment. The Achilles heel of cryoprecipitate was the difficulty in organising effective home treatment. It was by no means impossible – indeed, the number of centres which used cryoprecipitate for home treatment at one stage was in double figures – but it was not as easy nor as convenient as using concentrates. Home treatment would avoid the need to come to a hospital in pain, and then have to wait for a treatment which in total would take about half a day and which might need to be repeated if it was not effective within the half-life of Factor 8, usually about 12 hours.
The supply of cryoprecipitate was such that no cryoprecipitate needed to be imported. The need for such therapy, and the demand for it, was capable of being satisfied from the system of voluntary non-remunerated blood donation in the UK. There were sufficient donations to meet the need for all but a very small number of blood transfusions.[1514] So there was always self-sufficiency in blood.[1515] And the near unanimous evidence of the transfusion directors from whom the Inquiry heard is that there would have been no difficulty in making sufficient cryoprecipitate had more been needed. None would need to be imported. “Self-sufficiency” thus relates to the supply of fractionated blood products only – and principally to Factor 8 concentrates, since there was generally a sufficiency of Factor 9 concentrates to meet needs.
The supply of concentrates depended upon a number of factors. These were:
All of these, in turn, depended upon the policies adopted by the government and the way and extent to which they were put into effect.
The policies were not in doubt after 1974. It was, and on the face of it remained, the policy of successive governments to achieve self-sufficiency in the near future, and to cease dependence on expensive (and less safe) imports of concentrates. However, that goal was not achieved. Self-sufficiency was not achieved until after 1990. The “near future” as planned in 1974/1975 had become the distant future. Such a failure calls out for explanation.
In August 1967, Dr Biggs had emphasised, to the Ministry of Health, the need for the supply of Factors 8 and 9.[1519]
The following year the plans for the new PFC building at Liberton had been changed to allow for more AHG to be produced than originally intended.[1520] Work had begun on erecting the new building for fractionation at Liberton in 1971.
In July 1972 Dr Charles Rizza at the haemophilia centre at Oxford asked the hospital’s director of pharmaceutical services to purchase Immuno Factor 8 concentrate at an estimated cost of about £15,000 a year. The purchase was needed because of Oxford’s pre-eminence as a treatment centre, with about half the patients coming from other regions. The purpose of providing the material was to increase the “safety margin for the treatment of urgent cases” and it would permit a shortening of the waiting list for “non-urgent operations.”[1521]
In October 1972 the haemophilia centre directors from England and Wales met in Oxford. The general sense from the minutes of their meeting is that the contributors felt there was a general undersupply of concentrate, and that supply was also variable across the country.[1522] The supply constraints were not however so severe as to preclude Dr Maycock and Dr Bidwell saying they could supply enough freeze-dried concentrate from NHS sources to facilitate a trial of prophylaxis at Treloar’s school which the centre wished to mount.[1523] The idea of using a copious amount of NHS concentrate for this purpose did however lead to a discussion of whether this would unfairly prejudice supplies of concentrate elsewhere. Home treatment of people with haemophilia was discussed, but it was noted that some centres could not provide it because they did not have sufficient concentrate to do so.[1524] The chair, Professor Edward Blackburn, therefore wrote to the CMO asking for an expert committee to be set up to consider the supply of therapeutic materials to treat haemophilia and allied disorders. He commented that: “The great shortage of materials is limiting the treatment that can be performed, particularly the introduction of Home Treatment.” He emphasised that the directors felt there was “an urgent need to increase supplies of Factor VIII Concentrate”, adding: “Many feel that if a British preparation cannot be made available very shortly, the commercial preparations should be bought.”[1525]
In January 1973 Dr Maycock urged the Department of Health and Social Security (“DHSS”) to “have constantly in mind the need to develop our own sources in the UK transfusion services.”[1526] This was a plea for the Government to expand the capability of the UK to produce its own product. Though implicit in this letter, two weeks later he added his voice to that of Professor Blackburn to say expressly that the UK supply of AHG was inadequate.[1527] The CMO alerted the Permanent Secretary at the DHSS to the likelihood of increasingly heavy expenditure on commercial preparations which were being licensed, and which, “when … available [we] can hardly refrain from using”, resulting in a response suggesting a need to consider how far the home supply could be increased, leading to a lower cost.[1528]
Within a fortnight Hemofil was licensed for use in the UK. There is no indication, however, that the concerns expressed about shortfalls of supply between the haemophilia centre directors, Dr Maycock, and the DHSS had any influence on that decision.
At this stage, apart from a clear view that the supply of NHS-made concentrates was insufficient, it was not clear to what extent an increase was needed. That was to be addressed by an expert group set up in part for the purpose.
The Expert Group on the Treatment of Haemophilia met for the first time on 20 March 1973. To determine how much factor concentrate should be produced by the NHS to be sufficient to meet all reasonable clinical demand the meeting needed to know how many people there were with haemophilia in the UK; how many required regular treatment; what the average amount required for treatment was; and what was likely to be required in future. None of these parameters was clear. There was no national register of people with haemophilia. Nor was there any accepted unit of measurement: “donor units” was used, although experience with cryoprecipitate showed that the amount of Factors 8 or 9 in the plasma of a donor could vary considerably, and even from time to time for the same donor.[1529]
Dr Biggs produced a paper in an attempt to deal with these problems. She estimated there to be 1,754 to 3,000 people with severe haemophilia in the UK.[1530] At the time, they were already receiving an aggregate total of 300,000 donor units; but needed between 400,000 to 700,000 per year, from cryoprecipitate and concentrate combined. Though over ten years “an attempt should be made to provide all of the necessary material” in the form of factor concentrate, an initial aim should be to supply concentrate made from 250,000 donations for use in home treatment, with the balance being cryoprecipitate.[1531] Having considered her paper, the meeting “generally agreed” with her lower figure – that 400,000 donations per annum were required – but if strenuous efforts were made to clear waiting lists for surgery, or if home treatment or prophylaxis were to take off, more would be needed.[1532]
Importantly, for what follows, the expert group also thought:
The supply of plasma for cryoprecipitate and for sending it to make concentrate at that stage was 300,000 donations in a year.[1534] What was proposed was therefore a significant increase. The production capacity, after the current expansion of BPL had been completed, was said to be 135 litres per week (and thus around 350,000 donations per year).[1535]
The activity of Factor 8 was not then measured in international units: that standard measurement was proposed in 1970 but was not in general use until around 1973.[1536] Accordingly, many of the early estimates mentioned in evidence need to be converted according to an assumed rate. Comparing these standards (donor units, litres, and international units) with the activity to be gained from a single-donor cryoprecipitate creates further difficulty, because that single unit may be rich in Factor 8, or may be poor. In clinical use, a clinician will wish on the whole to ensure that an appropriate amount of activity is transmitted by an infusion, and thus prescription of packs of single-donor cryoprecipitate would be on the “high” side to allow for the difficulty of precisely determining activity, whilst aiming for a sufficient effect.[1537]
In March 1973 it had been thought that some 300,000 donor units were needed for that year’s treatment, and the Expert Group then meeting had estimated 400,000 would be needed for the future, both involving a mix of concentrate and cryoprecipitate. It had been considered that from within the 400,000 some 275,000 donations would be required to make factor concentrate if reliance on the use of imported concentrates were to be avoided.[1538]
Dr Biggs pressed her case for the higher figures she had quoted earlier through the MRC’s Blood Transfusion Research Committee Working Party on the Cryoprecipitate Method of Preparing AHF Concentrates.[1539] She foresaw a future when little or no cryoprecipitate would be used. Her paper noted that by January 1974 the supply of treatment for Factor 8 and Factor 9 replacement derived from approximately 300,000 blood donations per year, most of this was provided in the form of cryoprecipitate. On the basis of calculations, made by looking at what was being supplied to pupils at Treloar’s,[1540] it worked out that the amount of material required to treat all patients with haemophilia in Great Britain adequately would be between 547,540 to 750,000 blood donations per year. The conclusion was that that amount needed to be “fractionated annually to produce freeze-dried Factor 8 concentrates.”[1541] The group’s report was later published in the British Journal of Haematology.[1542]
There was a dissentient voice. Dr Christopher Bowley, regional transfusion director in Sheffield, attempted to get his fellow regional transfusion directors to persuade haemophilia directors to change course.[1543] He thought that Dr Biggs was suggesting too great an increase in the amount of donations which would be used for fractionation.[1544] He made the point that she was basing her paper on the practice of the Oxford Haemophilia Centre which used “a very great deal more material (per case) than anybody else”. He said he had spoken with a number of senior haematologists and “they all thought, [that] given an adequate supply of good quality cryo[precipitate] and just a small supply of super concentrate for the major surgery or the patient with inhibitors, they would be very happy.” He added: “Bearing in mind that Factor VIII is inevitably wasted at all stages of preparing and using concentrate, it may well be that money and effort should be channelled towards more and better cryo.”[1545] He had some support from Dr John Wallace, regional transfusion director in Glasgow and West of Scotland. He too thought that “Adequate amounts of a good quality cryoprecipitate would probably cover most clinical indications for factor VIII therapy.”[1546]
Both of their papers were discussed at a meeting of regional transfusion directors and haemophilia centre directors, and the minutes record that: “It was felt that once the new fractionation laboratories in Edinburgh and at the Lister Institute[1547] were in full production they should be able to meet the needs of the country provided sufficient plasma was available.”[1548]
Despite this report, no central funding was provided.[1549] Dr Biggs then went public with her concerns about funding. Having given notice to Dr Sheila Waiter at the DHSS of her intention to write to The Lancet, she wrote that the reason for the shortage of Factor 8 was the expense of Factor 8 concentrate.[1550] At this stage, much of the Hemofil and Kryobulin, which was available through central contract with the DHSS for regional health authorities to purchase at a predetermined rate had simply not been bought. This seemed to her to be the consequence of the amount of money needed to buy it even at the preferential rates secured by collective purchase.[1551] Dr Biggs concluded by noting “the ridiculous impasse of large available stocks of therapeutic materials locked up in stores because no-one would buy them and, on the other hand, patients in dire need of this same material.”[1552]
This led to a parliamentary question and response by Dr (later Lord) David Owen, who had become Minister of State for Health.[1553] The response did not challenge Dr Biggs’ central points: that concentrates were the optimum treatment; that commercial product was available but, despite that, UK domestic production should increase; and that home treatment was desirable as a goal.[1554]
At this stage, the Expert Group had set a goal of 250,000 donations to be used for Factor 8 concentrate (March 1973); this had been increased to 275,000 by regional transfusion directors following the Joint Steering Committee (June and July 1973);[1555] and the MRC Blood Transfusion Working Party had then endorsed a range from 547,540 to 720,000 donations (including cryoprecipitate) (January 1974). The figures were escalating. But even the goal of 275,000 donations for Factor 8 production had not been met a year after it had been given.[1556]
Dr Maycock had already seen dangers lurking for the voluntary non-remunerated blood donor system upon which the transfusion system in the UK was based, if the need to import commercial products to address what had been seen as a short-term need became a permanent demand. He recognised a need for blood transfusion services to be “self-supporting”;[1557] but this was seen by more than him alone. The SHHD considered that the “present dependence on commercial supplies of anti-haemophilic globulin concentrate and PPF [plasma protein fraction] posed a threat to the unpaid voluntary donor system” and meetings had been held between their representatives and those of the DHSS at which:
“the following principles had been reaffirmed:-
Though the facilities at BPL were cramped into too small a space, and its production capabilities were limited, Edinburgh was beginning to produce factor concentrates, and Dr Maycock was still of the view that overall UK production facilities were more than adequate to meet the demand for fractionated product.[1559] The DHSS, and he, therefore understood that it was the supply of plasma for fractionation which needed to increase if the shortfall in meeting anticipated demand was to be met from within the NHS.[1560]
The amount of plasma available to send to BPL for fractionation could be increased by arranging for a greater number of donations of whole blood; but it could also be increased by ensuring that no part of any donation was wasted. Where a patient’s need was for the replacement of red blood cells, traditionally whole blood had been transfused to meet it. Yet more than half of any donation of whole blood consisted of plasma, which such a patient did not need. Red blood cells could be separated from whole blood, to leave plasma – and since it was that plasma which contained Factors 8, 9 and other proteins of therapeutic value, and could be sent for fractionation, to separate red blood cells out in this way was to make use of the whole of a whole blood donation.[1561] Efforts were thus made by Dr Maycock and his colleagues to persuade clinicians to use less whole blood and more packs of concentrated red blood cells. Whereas in Scotland the service had by 1974 managed to use some 30-40% of donations in this way, efforts at persuasion were met with little success in England, which achieved less than 10%.[1562]
Whether the solution to the problem of increasing the supply of plasma lay in more donations, better use of present donations, or a happy combination of the two,[1563] it came at a cost. Under the system of finance then adopted in the NHS, each regional health authority managed its own budget. The DHSS considered (for good reason) that a large contributory factor to the lack of supply was an unwillingness on the part of regional health authorities to spend money on sourcing and providing materials to a body (BPL) over which they had no direct control. Neither BPL nor the National Blood Transfusion Service (“NBTS”) could direct them to do so; the DHSS would not direct them to do so; and the system of funding had thus far not permitted it. The regions had other demands on their finances which they saw as more pressing.
Pressure on the Government to act was exerted by clinicians, by the medical press, by NBTS, and by the advisory bodies which had been set up.[1564] The expense of having to purchase more and more concentrates from commercial enterprises, on a continuing basis, could harm not only the public finances, but possibly public health, and might put at risk the voluntary donor system itself. The Government was aware, too, that sacrificing national control over a valuable therapeutic supply, and rendering the UK vulnerable to a shortage of supply from third-party providers outside the control of the UK, could add to these difficulties. Accordingly, a policy began formulating within the DHSS that self-sufficiency should be achieved.
Between October 1974 and the end of the year, the policy evolved internally. On Christmas Eve 1974 a letter to regional administrative officers set it out. The DHSS recognised that there was an immediate need to provide AHG concentrate, equivalent (now) to some 275,000 blood donor units. It was because of this need, the cost of commercial alternatives, and the potential threat to the voluntary donor system if commercial firms considered it worth their while to establish panels of paid donors in the UK to obtain their own supplies, that the DHSS regarded it “as of the greatest importance[1565]… that the NHS should become self-sufficient as soon as practicable in the production of PPF and other blood products.”[1566] Since supply of raw material in the form of plasma depended on the number of blood donations collected, and the extent to which clinicians were prepared to use blood in the form of concentrated red cells – ie not using whole blood, but only the red cell portion of it, leaving the balance (plasma) to be sent for fractionation – they were to be encouraged to do this. The reluctance of regional health authorities to fund a greater supply of plasma to the central production facilities was to be met by an exceptional step: the bill would be paid by the DHSS centrally. However, in deference to the principle of regional control over expenditure, this would not be by expenditure directly from the centre but by making funds available to the regions which would be earmarked for the purpose of increased plasma production.[1567]
On 22 January 1975 the self-sufficiency policy which had been devised during the previous three months was made public by Dr Owen. In answer to a written parliamentary question he said: “I believe it is vitally important that the National Health Service should become self-sufficient as soon as practicable in the production of Factor VIII including AHG concentrate. This will stop us being dependent on imports and make the best-known treatment more readily available to people suffering from haemophilia. I have, therefore, authorised the allocation of special finance to boost our own production with the objective of becoming self-sufficient over the next few years.”[1568]
In his evidence to the Inquiry, Lord Owen made it clear that a major motivating factor, as far as he was concerned, was to ensure the safety of the patient. He had in mind the dangers of hepatitis, and the increased risks of this posed by the pool sizes used by commercial companies.[1569]
On 25 and 26 February 1975 he again pointed in Parliament to the £500,000 of special financing which was “to increase the existing production of Factor VIII”.[1570]
Yet again in Parliament, on 7 July 1975 Dr Owen described the Government’s policy as “to make the NHS self-sufficient in the production of Factor VIII as soon as practicable”.[1571]
The implementation of the policy was overseen by a policy official, Donald Jackson, in the DHSS.[1572] On 11 July 1975 he recorded that he had set targets which would produce plasma (for concentrate production) from 337,000 blood donations. “This is some 20% more than the total of 275,000 recommended by the Expert Group on Haemophilia but that figure must be regarded as the minimum.”[1573]
This led to an interesting insight into the extent to which ministers were kept abreast of knowledge within their departments. The Haemophilia Society met Dr Owen in December 1975, and attempted to point out that the DHSS was pursuing the wrong planning target. It was too low, given that Dr Biggs’ paper adopted by the MRC Working Party in January 1974 as a basis for future planning had suggested over 500,000. Dr Owen did not recognise Dr Biggs’ paper for the working party when the Society referred to it and he asked to see a copy. He told them he would look at the MRC study and would write to the Society giving the basis for the Department’s target.[1574]
The DHSS targets were expected to be met in 1977. Estimates of need shifted upward in the interim. In January 1976 Dr Bidwell, director of the PFL, wrote a confidential paper based upon her understanding of the number of patients with haemophilia and on “internal data from PFL and RTD (75) 26”.[1575] She made assumptions as to yield,[1576] and as to the appropriate figures produced by conversion from international units to plasma volume to weight in kilograms to number of donations. On the basis of these she calculated that the need would be for between 970,920 and 1,213,650 donations to be devoted to plasma supply (or 36-45 million international units).[1577]
If she was right, then the target which had been set, and which was to be met 18 months later, was, as she noted, already an aspiration to produce only around a third of what was needed.[1578]
When the Expert Group on the Treatment of Haemophilia and Allied Conditions next met (in May 1976) Dr Biggs advanced an estimate similar to that of Dr Bidwell. It was that the total requirement would be 40 million units of Factor 8 in all forms (both concentrate and cryoprecipitate) based on a population of people with haemophilia of approximately 3,000. This estimate did however, depend upon the accuracy of her assumptions about the amount of plasma that would be obtained from each donation.[1579]
The expected supply from the NHS was in the region of 31-34 million international units, provided that the rate of production of cryoprecipitate was maintained even as the production of freeze-dried concentrate increased. This left a shortfall of some 6-9 million from Dr Biggs’ estimate. In the end the Expert Group agreed not to fix a new specific target but to review it again when the original target figure had been attained.[1580]
The discussion in the Expert Group – in particular its belief that “with the extension of home treatment joint surgery etc the current target may represent no more than ⅓ to ½ of the amount of Factor VIII which may be required in 5 years time or less” – was reported to the Central Committee of the National Blood Transfusion Service. It was also reported that“The Department [of Health] is considering the implications of the new advice.”[1581]
At the Central Committee’s meeting on 22 June 1976, the chairman proposed a review of the clinical use of blood and blood products, including an examination of the overall use of blood and blood fractions, and “whether optimal use was being made of the raw material – donated blood”, no doubt being of a mind that if less were to be used to give transfusions, more plasma would be available from the same number of donations, and self-sufficiency could be achieved more easily.[1582]
The review was to be carried out in late 1976 by Thomas Dutton and Dr Waiter, both civil servants in the DHSS, who were joint secretaries of the Central Committee for the NBTS. In the course of preparing it, it became apparent that there were difficulties in obtaining sufficient information, but they referred the Committee to a paper one of them (almost certainly Thomas Dutton) had prepared earlier, as background to the problems the Committee was facing.[1583] This was itself a thoughtful review, covering a wide range of issues. For the purpose of this chapter, it is necessary only to say as follows. It commented that it was difficult to obtain a reliable estimate of the amount of any product which would be required in the foreseeable future, since in many instances the pattern of treatment which had developed might well have resulted from current shortages which might, in time, be overcome. It considered that clinicians were uncertain about their requirements, and this uncertainty created major problems for the blood service and the central blood laboratories, noting that “The clinicians now believe that they will require 3 times the amount of Factor VIII originally forecast” because the greater use of Factor 8 concentrates had opened up new treatment possibilities, such as home treatment and rehabilitative surgery. This fluidity in treatment and demand meant that “Self-sufficiency in blood products is clearly not a static situation which once achieved will require only infrequent modification. In its fullest sense it would mean attempting to keep up with developments in the world industry in blood products which shows few signs of reducing its activities despite WHO resolutions about the undesirability of relying on paid blood donors.” It noted that the health departments had decided to set up a small expert group to consider likely future trends in demand.[1584] The small expert group to which this was referring was the Working Group on Trends in Demand for Blood Products, which was established in January 1977.
On 13 January 1977, before the first meeting of the Trends Working Group, Dr Waiter attended a meeting of haemophilia centre directors. Professor Blackburn said that reference centre directors understood that the blood services could supply enough plasma to produce 40 million units of factor concentrate per year, which they regarded as a minimum requirement. However, they considered that there was a “hold-up in the expansion of fractionation in the U.K.”[1585] Dr Waiter responded that the DHSS had understood that the capacity at Liberton, Elstree and Oxford was adequate.[1586] With the stated capacity of those centres, a target of 50 million international units could be met. The maximum capacity of each of the three production facilities was examined – 14-15 million international units for Elstree and Oxford[1587] combined, and (said Dr Iain Macdonald from SHHD) 60 million international units at PFC, though to achieve this would need some £25,000 for new equipment and extra running costs, which would include payment to staff to operate a 24-hour shift system of working.[1588]
The Trends Working Group had its first meeting in February[1589] and reported in December 1977.[1590] It considered not only the production and supply of factor concentrates, but of all forms of therapeutic blood products. It calculated that over a 10-year period the amount of Factor 8 used by the UK would reach a level which equated to 60 million international units per year – but the amount of albumin required by the UK meant that the plasma used for that would enable 74 million international units of Factor 8 per year to be produced.[1591] It envisaged that there would be a complete transfer from cryoprecipitate to fractionated freeze-dried concentrate but that “Considerable further investment in collecting, testing, processing and premises”would be needed to meet the proposed targets: it was thought that the“present UK capability is less than half what we regard as essential. Additional major investment is, therefore, also needed for this.”[1592]
The estimate for the next ten-year period used by the Trends Working Group to assess the needs of the UK population for factor replacements measured in international units usefully equates to 1,000 international units per 1,000 population: such that a population of, say, 56 million as it became in the 1980s would require approximately 56 million units,[1593] one of 60 million would need approximately 60 million units and so on. Thus as the population increased so too some increase in the quantity of fractionated product would be necessary. This explains why there were higher estimates for the requirements in ten years’ time than the amount thought optimum in 1977.[1594]
The minimum goal which had been set by the DHSS of 340,000 donations was met by mid 1977. Roland Moyle, who had by now succeeded Dr Owen as Minister of Health, reported this to Parliament the following year.
He reported that (by then) both BPL and PFL were working to full capacity, though that capacity was being increased.[1595] Between them, they produced approximately 15 million international units of Factor 8 concentrate per annum. About the same amount of cryoprecipitate was produced by NBTS each year. Production in England was thus some 30 million international units. Total usage of Factor 8 was reported to be approximately 45 million international units per annum. That suggested a shortfall of 15 million international units.[1596]
How the shortfall would be made good from domestic production (it was plainly being met by the purchasing of commercial concentrate for the time being) was addressed only by saying that the regions were “being asked to provide more fresh frozen plasma to the central processing laboratories where the National Health Service concentrate is produced.”[1597] Quite what it was hoped to achieve if they did so, since both BPL and PFL were said to be working at full capacity, is unclear. In December 1978 Roland Moyle recognised that the commitment to self-sufficiency had “not yet” been met.[1598]
This came after further estimates of demand/need.
First, the estimates which had been reported by the Trends Working Group in late 1977 were largely thought to be reliable estimates for future need by the Standing Medical Advisory Committee in 1978.[1599]
This was no surprise to the DHSS. In a memo sent to medical and administrative civil servants, as well as Dr Maycock and Dr Richard Lane, Thomas Dutton observed that the report “essentially it says no more about Factor VIII requirements than some experts have been saying for years and which has now come to be generally accepted”.[1600] It was assumed in his memo that there would be general acceptance of the need to provide blood products on the scale envisaged by the Trends Working Group. He noted that a Blood Components Production Programme for the next ten years needed to be drawn up: the Central Committee for the NBTS and its Sub-Committee on the Central Laboratories was “on the basis of past experience not adequate for this task, even if their roles were changed from advisory to managing committees.” He continued:
“The production programme will require ‘managing’ in every sense (although it may be advisable to avoid the term and refer to ‘coordinating’) by people who are closely involved, and who are responsible for the outcome. They must be able to achieve results in a situation where success depends on the ability to persuade Health Authorities to co-operate, which in some instances may mean giving up activities [which have] hitherto been regarded as part and parcel of their function.”[1601]
His conclusion was that to meet the requirements foreseen by the Trends Working Group:
“economically and without a great deal of frustration, expensive duplication and uncertainty will require a major effort in co-ordination in a highly technical field. The constitution of the NHS and the understandable desire of Regional Authorities for autonomy are natural obstacles to sustained co-operation of the kind that will be required and it is proposed that the 10 year Blood Components Production Programme should be co-ordinated by a managing committee expressly set up for the purpose. In view of the inter-dependence of England & Wales and Scotland in blood products, particularly the need to be able to fall back on other plant if there is a local breakdown or contamination, it is proposed that the Blood Products Production Programme should be drawn up on a UK basis … The essence seems to be that without a measure of co-operation which has hitherto been unnecessary, there is little likelihood of achieving the targets set by the Trends Working Party, far less of achieving them at the minimum cost to the NHS and that for this purpose the setting up of a national machinery for co-ordination is unavoidable.”[1602]
These words echo the themes explored in the paper which he and Dr Waiter as joint secretaries had sent to the Central Committee of the NBTS: the problems caused by the regional structure and funding of the NHS; the consequent reluctance to provide plasma to BPL for fractionation; and the absence of any power to require plasma to be provided.
At the end of 1978, the Minister of State for Health, Roland Moyle, told Parliament “that self-sufficiency has not yet been achieved, and my Department is therefore reviewing production in relation to present demands and resources.”[1603] The review which followed considered various options, which included handing the whole fractionation process to the commercial industry as well as increasing the capacity at UK facilities. The latter was thought more viable.[1604]
The next year there was again an upward shift in estimates of future needs, though slighter on this occasion than it had been in the past: current demand for Factor 8 was probably in the region of 60 million international units, but if clinical freedom continued, it was possible that the eventual requirements might well approach the 100 million international units per annum mark.[1605]
Those figures helped to inform planning of the capacity of a redeveloped BPL (of which more is written later). Although it was recognised that estimates for five years’ time were highly speculative, it was obvious that the new production facility then being contemplated required some attempt at meeting them. Dr Lane considered in 1979 that a redeveloped BPL could be commissioned to increase production capacity to 90 million international units between 1985 and 1990, as an intermediate stage,[1606] and then to scale up production to 120 million units for the years that followed.[1607]
By 1982, planning was eventually under way for a new building to constitute BPL at Elstree. The approval given by the Treasury in November 1982 for the reconstructed BPL was for a plant capable of fractionating 400,000 kilograms per annum.[1608] The overall plasma supply target was however likely to be somewhat higher, to include plasma used to produce cryoprecipitate, which still retained a useful therapeutic function, albeit that it was foreseen to have less of a primary role in treating bleeding disorders.
A plasma supply target of 435,000 kilograms, including this element for cryoprecipitate production, was broadly maintained thereafter, and although estimates thereafter continued to increase, there was a growing consensus that demand for Factor 8 would increase to the region of 100 million international units, perhaps a little over. The increases in estimated needs were now gradual compared to those that came before.[1609]
It follows from this chronological account that the therapies thought desirable for the treatment of people with bleeding disorders during the 1970s required larger and larger amounts of factor concentrate. The causes of this are most likely to have been the availability of commercial concentrate in substantial quantities from 1973 onwards, the use of which created a greater demand for still more to be supplied. A significant driver was the demand for home therapy, which was most conveniently satisfied by freeze-dried factor concentrate which could be kept in domestic refrigerators and reconstituted as needed; but it was not the only issue. The increased lifespan of people with bleeding disorders following the success of cryoprecipitate treatment since 1966 meant more patients required treatment, and the more active lifestyles encouraged by the availability of treatment may have led to a further need for it. Some clinicians aspired to develop prophylaxis, which used a considerably greater amount of material; but this was not widespread. Operations requiring factor concentrate cover became more common. Sadly, though, the figures used as a basis for Dr Owen’s central expenditure of £500,000 to enable the regions to produce more plasma were based on estimates that were outdated even before the policy was announced. This was realised in the DHSS. It was thought by 1977 that there was a need for a blood products production programme to ensure an effective and coordinated approach to achieving self-sufficiency. There never was one. Self-sufficiency remained an important – but elusive – goal.
It is difficult to avoid a conclusion that as a matter of fact, too little was done too late. The need may initially have been focussed on the provision of more plasma to be made available from the regions to a greater extent than on expanded production facilities, but it was always about both.[1610] This was known to the DHSS. The opportunity was missed.
The extent to which Factor 8 replacement therapies (fresh frozen plasma, cryoprecipitate, NHS factor concentrates and commercial concentrates) were consumed in the UK year by year between 1969 and 1990 is best portrayed by a chart, as shown at Figure 1 below. Factor 9 is not shown since for most of the period of central interest the UK was self-sufficient in it.

Figure 1 is drawn from haemophilia centre directors’ statistics. The Inquiry is satisfied that these represent the best available and most complete source. Nonetheless, the data has limitations. The figures are based upon the information which was given by the centres. That was incomplete. Not every centre made returns, and some made them for some years, and some never. The nature of the returns had the appearance of having been hastily compiled in many cases, rather than the appearance of care being taken to cross-check. Further, product was consumed in vials or bottles which usually contained 250 international units. However, some bottles were larger. Not all of their contents might have been used. But the full contents will still count as “usage”. The usage of cryoprecipitate is particularly imprecise because it will have been prepared locally. Different laboratories in different regions will have achieved different levels of yield, making the estimates of the number of international units of Factor 8 provided to a patient imprecise. The consumption frequently appeared as “bottles”, from which a calculation of the number of international units contained was made based on an assumption as to the average number of units each bottle contained. Finally, since international units were only adopted as a recognised standard in 1973/4, the figures which are shown will have been calculated by the UK Haemophilia Centre Directors’ Organisation making a number of assumptions.

Figure 2 shows part only of the same chart as in Figure 1, in order to focus attention on three matters.
First, it was not until mid 1976 that cryoprecipitate ceased to be the main source for Factor 8 replacement: at the start of the year just over half the total consumption came from that source. The chart does not show a headlong rush, across the board, by clinicians to embrace factor concentrates. Given that the use of concentrates was especially prevalent in home treatment, it may be inferred that cryoprecipitate remained the main product used for much hospital treatment until later in the 1970s. It follows that when, in 1983, consideration was being given to whether a ban on the importation of imported concentrates might lead to there being no product capable of preventing serious bleeding, recent experience should have led to the realisation that cryoprecipitate was an acceptable alternative.[1613]
Second, it shows the dramatic effect of Dr Owen’s initiative in increasing the supply of plasma to BPL, but that instead of the effect of this being to reduce reliance on imported concentrates, the consumption of those also increased in volume at very much the same rate as did that of NHS product. Figure 1 shows that between 1974 and 1988 more commercial concentrate was consumed in the UK than NHS concentrate. Even by 1990 self-sufficiency had not yet been achieved in England and Wales, though it was effectively achieved just after that.
Third, it shows a spike in the intake of Factor 8 from factor concentrates and cryoprecipitate combined in the 1977 figure. It is not clear what was the cause of this: readers should however be aware that it might simply be an artefact of the figures, which otherwise show a steady increase in the uptake from the start of the 1970s until 1990.

On the basis of these figures,[1615] despite the uncertainties of the data, it can be seen that the estimates of the MRC Working Party were generally in excess of what was actually used until the early 1980s, though the initial DHSS planning targets were not. The problem in achieving self-sufficiency was not, therefore, a failure sufficiently to estimate what would be needed: it was a failure to plan and produce it, partly because of lack of sufficient plasma, but mainly because the central production facilities were inadequate.[1616]
Plasma for fractionation was of two kinds: recovered plasma and time-expired plasma. Recovered plasma was plasma which was separated, either manually or by machine, from a whole blood donation. It was recovered and immediately frozen and is thus identified as “fresh frozen plasma”. Time-expired plasma is plasma which is recovered from a donation which has been kept for so long that the red blood cells have ceased to be effective for treating a patient. Over time, the quality and acceptability of donated red blood cells diminishes. The same is true of some of the proteins contained in plasma. Thus Factor 8 loses activity over a short period of time: in the body, it has a half-life of around 12 hours. Accordingly, if it is to be harvested from blood, the blood has to be fresh. Otherwise the plasma component of the donation will not form a useful base from which to extract Factor 8 or Factor 9. However, albumin and immunoglobulins take longer to deteriorate. Time-expired plasma remains useful for making those products.
This leaves two matters relevant to understanding the supply of plasma. First, blood was collected regionally. If a region were then to recover plasma from whole blood to send to BPL or PFC, it would first have to be separated from the red blood cell component of blood. Facilities to make that separation had to be available, whether the separation was to be manual or by machine. Alternatively, plasmapheresis might be organised. This involves a donor giving only their plasma and not their red blood cells as well. Plasmapheresis was generally achieved by machine. Blood was taken from the donor and passed through a machine designed to separate the plasma from the red blood cells. The red blood cells would then be returned to the donor. Since plasma takes a couple of weeks or so to replenish itself within the body, whereas red blood cells take very much longer, it is possible without significant harm to the donor for a donor to give as many as 26 donations of plasma in a year by plasmapheresis. Donors who provide whole blood, and who do not have their red blood cells returned to them, may safely give blood no more than four times a year (if male) and three times a year (if female).[1617]
The second aspect of importance is to note that to focus upon the amount of plasma “received for fractionation” by the fractionating plants is not the same as asking how much plasma was “received for the production of Factor 8 and Factor 9”. Time-expired plasma, for instance, would be received for fractionation because it remained a valuable source of albumin and immunoglobulins, the quality and utility of which did not diminish quickly over time, but would not be usable for making factor concentrates because little or no clotting factor activity would remain once “time” had expired.
It is for these reasons that the figures for plasma supply have concentrated upon the supply of fresh frozen plasma. Most came as recovered plasma; a little came from plasmapheresis.[1618] None came as time-expired.[1619]
The chart below shows the supply of fresh frozen plasma to BPL each year.

Much of the information available to the Inquiry relates to the position in England and Wales. However, the policy until early 1978 (as to the change that then took place, more is written later) was to see the UK as one unit in terms of production of factor concentrates for use within the UK. That meant aggregating the production capabilities of both the Scottish and English production facilities. If, therefore, fresh frozen plasma was supplied to BPL and PFL in excess of their current capacities to process it, the Edinburgh facility would have been available to process it, providing always that it had not been supplied with a surfeit of fresh frozen plasma from within Scotland itself.
The story, broadly, of the period from 1967-72 is that there was little concentrate in circulation, and its use was limited. Nonetheless, there was a slowly growing demand for it, and a sense that the UK needed to increase its own production if commercial concentrates were not to dominate the market before long. There was a growing gap between the amount of fresh frozen plasma being sent from the regions to BPL for fractionation and the demand for finished product. Usage of commercial concentrate was low, until 1974-75, but it had by then become available generally rather than under the named patient exemption. In 1973, as can be seen, most treatment needs for people with haemophilia were met by cryoprecipitate. At least 80% of the usage was by this means. Cryoprecipitate was made regionally. Standards varied. But in general, no shortage of cryoprecipitate for treatment was thought to exist. A push for self-sufficiency began in 1973, when the convenience of factor concentrate for home treatment led to suddenly increasing demand.
There were three essential problems with increasing the supply of plasma to the central production facilities, over and above the question of financing it. The first was the way in which the National Blood Transfusion Service was organised. As the chapter on Organisation of the Blood Services discusses, and as Drs Harold Gunson and Helen Dodsworth were to observe in 1996: “A problem which BPL has had to contend with throughout its history is that it has never been in control of its plasma supply, with the exception of 1975 when the DHSS financed an increase. The only argument which could be used with the RTCs [regional transfusion centres] was persuasion.”[1621]
This became the subject of an editorial in The British Medical Journal in 1974.[1622] It argued that the blood services were ill-equipped to do the job as a modern transfusion service, suggesting that the “shortage” of blood and therefore plasma, allowing entry to the UK of the products of pharmaceutical companies was not a real shortage, but a consequence of poor administration, organisation and underfunding, and that there was urgent need for a national policy for the procurement and distribution of voluntarily donated blood.
Importantly, this was not simply a matter of comment from the medical press. It was recognised at an early stage by those civil servants most closely involved with advising ministers about blood supply. In a review in 1976 of the requirement for blood products and their availability, Thomas Dutton[1623] echoed some of the themes The British Medical Journal had highlighted by identifying that:
“The customary method of financing the NBTS is not conducive to the development of such a partnership and it was probably this more than any other single factor which led to the delay in mounting the AHG (Factor VIII) Concentrate production programme.”[1624]
This document, discussed above, is significant. It spoke not only of the problems of the way in which the blood service was organised, and the problems that regionalising autonomy had created in organising a national production service which depended upon the regions spending their money for these central purposes at the expense of some of their local priorities, but of the delaythis had caused in achieving sufficient production of factor concentrates.[1625]
A second factor, as Thomas Dutton and Dr Waiter pointed out, was the way in which blood supply was financed. This was through the regions, each of which in England was allocated its own finances. Although a clinician could approach a regional or hospital treasurer to obtain funding to purchase factor concentrates, regions were persuaded only with difficulty to spend money on producing plasma, freezing it, and supplying it to a body outside the region and its control (BPL).
Obtaining blood from donors was a matter for each region. It came with some cost. Separating plasma from that blood in order to transfer to a body which was effectively a third party involved staff, equipment, premises, and gave rise to some more cost. The regions could not be sure of any return on this expense for the benefit of the patients for whom they were responsible. Accordingly, persuading them to produce more for a benefit which was uncertain was always likely to be difficult. There was no compulsion upon them to do it.
It was not until Dr Lane secured the introduction of a return of factor concentrates to the regions in proportion to the amount of fresh frozen plasma they had supplied to BPL (“the pro rata scheme”) that there was much change.[1626] It was recognised that there were some centres which had a special need for the supply of concentrate, such as was necessary at Treloar’s. Allowance was therefore made in this scheme to accommodate them. After adjustments to the pro rata principle, to deal with special cases such as Treloar’s, the DHSS introduced the scheme with effect from 1 April 1981.[1627] It was successful in helping to ensure a greater supply of plasma from the regions to the central processing units in England and Wales.[1628]
By 1989, however, the increase of plasma supplies and factor concentrate production following the redevelopment of BPL coming into full production meant that some regions which sent large quantities to BPL might receive more Factor 8 than they could use, whilst others that were not “plasma rich” would be left in need. The original rationale for the system, encouraging regions rapidly to increase the quantity and quality of plasma supply to BPL at a time when demand for finished NHS product exceeded its supply, no longer applied. So, in 1989, a revised system of cross-charging was introduced following trials.[1629]
A third problem was the persistence of treating doctors using whole blood rather than red blood cells.[1630] Not only that, but many clinicians overused transfusions. Doctors had for several years been encouraged to transfuse to patients only that component of blood which they really required – in most cases, this would be the red blood cell component – and to transfuse no more than was strictly necessary.[1631] Ever since the Second World War, doctors involved in facilitating transfusion had been at pains to encourage a parsimonious approach to administering blood.[1632] These pleas initially fell on deaf ears. Clinicians tended to use techniques, including administering transfusions, with which they were familiar, in ways and in amounts with which they were familiar, rather than taking any active steps to change what had become their clinical habits.
It was difficult for those supplying blood to do much to change their practice. This was because in the first 40 years of the history of the NHS a huge respect was paid to the clinical judgement of practitioners treating their patients as they individually saw fit. This approach – “clinical freedom” – dictated that in the great majority of cases the guiding rule was that other doctors and in particular, administrators, would not significantly interfere in the treatment being provided.[1633] Medical treatment was thus individualised not only to the patient, but also by reference to the particular treating doctor and their habits. Unless a doctor wished, therefore, or could be gently persuaded, to take a different approach, it was not felt that anyone else had any right to interfere. The consequence of taking this approach, patient by patient on an individual basis, when it came to transfusion was that the collective interest of other patients was little considered. That collective interest lay in those blood components which were not going to be of any real use to the immediate patient being diverted for the benefit of those others, rather than uselessly put into the veins of the immediate patient who (almost by definition) did not need them. Persuasion, accompanied by some education, was the only tool, and it was not very successful.[1634]
Other steps were taken to improve the amount of plasma, and its quality, coming for fractionation to BPL.
In the very early 1970s, some regions were still using glass bottles with which to convey frozen plasma to BPL. Plastic bags were much more suitable. They were easier to freeze. They were easier to thaw. And they were easier to handle. First, there was a change from glass to plastic; and then a change in the size of bag used. This latter was important, but needs some explanation.
The system that operated was to use five-litre packs of plasma. It became apparent by mid 1977 that the system of using such packs was not compatible with good manufacturing practice, unless the “pooling” of the plasma donations before filling the packs took place in aseptic units.[1635] Such units would be expensive to develop. By contrast, single-donor plastic packs which formed a “closed” system for separating and handling plasma became seen as preferable. A further advantage in the use of single plasma packs was not only that open processing at regional transfusion centres would become minimal, reducing the need for redevelopment and capital expenditure to provide clean and sterile areas, but that such packs could more effectively be tested by RIA[1636] than five-litre packs. They were also suited to rapid thawing, which improved the yield of Factor 8 by as much as 60%.[1637] The change to single plasma packs did necessitate changes to storage facilities and production methods, but they lent themselves readily to the process of splitting open the bag (indeed, bags were designed specifically for the purpose in a wedge shape so that the contents could be more easily pooled in the process of manufacturing concentrate).
Trials using single plasma packs began in late 1980.[1638] The change to single plasma packs proved efficient in saving time and resources at regional transfusion centres.[1639] Although there is no direct evidence that a change from five-litre to single-donor packs of frozen plasma for fractionation increased the quantities of plasma coming to BPL, the combined effects of a pro rata scheme and the widespread use of single plasma packs were probably responsible for an increase in the amount of fresh frozen plasma received at BPL in 1981/82. It was the first time in five years, according to Dr Lane, thatthe input of plasma for fractionation had increased.[1640] It had increased by over a quarter. Not only, it seems, did the use of single plasma packs improve the quantity of the plasma received, but also its quality. The faster the plasma was frozen, the more the activity of the Factor 8 within it that was preserved. The yield from plasma collected in this way was thus always likely to be higher, and there was less risk of contamination.
In the early 1970s, Scotland was well ahead of England in ensuring that as much blood as possible could be administered to patients without unnecessary plasma. This meant ensuring that they were “packed” red blood cells (sometimes called red cell concentrates). Until the mid 1960s, clinicians almost invariably used whole blood to replace red cells and to restore blood volume in patients.
A booklet entitled “Notes on Transfusion” was issued by the DHSS, SHHD and the Welsh Office in 1973.[1641] It began by saying that “Transfusion therapy should be undertaken only after careful assessment of the patient’s clinical condition to determine the nature and quantity of fluid to be transfused and the rate of administration. The patient may require whole blood, concentrated red cells or other blood components or one of the special plasma fractions” It then went on, in bold, to say:
“A transfusion should never be given without a definite indication; not only is this in the patient’s interest, since an element of risk is associated with every transfusion, but supplies of blood are not unlimited and with the ever growing demand for blood it is imperative that it should not be used unnecessarily.
The use of transfusion to correct moderate or slight degrees of anaemia that could be overcome as effectively, if more slowly, by other means, seems unjustifiable unless some cogent reason for speed of recovery exists. In some instances failure to institute simpler and safer but equally effective treatment earlier leads to the quite unnecessary use of blood transfusion.”[1642]
Similar calls were made throughout the 1970s.
Some clinicians were reluctant to use concentrated red blood cells because they had greater viscosity,[1643] were slower to transfuse, and often had to be pre-diluted with saline. Some concerns were raised that over-insistence on the use of concentrated red cells would lead to clinicians using plasma protein fraction in addition, to provide a product that flowed more easily, thus limiting the amount of additional plasma that might be released for fractionation.[1644]
In order to prevent red blood cells being too viscous to be administered easily, in turn leading to clinicians not wishing to use that as a component on its own, some of the plasma that might otherwise have been separated from them was kept together with those cells. This also provided the red blood cells with the nutrients they required to survive.
Although some 55% of blood is composed of plasma, the use of some of the plasma in this way to carry and support the red cells, meant that generally only 180ml of plasma could be removed from each donation.[1645] So far as viscosity was the problem, a fluid like saline could be used to provide greater fluidity. However, this would leave the red blood cells deteriorating, since they were unsupported by the nutrients they might otherwise have obtained from plasma, and defeat the purpose.
Accordingly, scientists searched for a solution they could add to packed red blood cells which might both counter the viscosity of the concentrated red cells and also provide those red cells with a source of energy. The optimal additive solution was discovered to be a mixture of saline, adenine, glucose and mannitol: “SAG-M” as it more conveniently became known.[1646] Its introduction permitted more of the plasma in a donation of whole blood to be separated out, for that could be replaced with SAG-M. This enabled approximately one and a half times as much plasma to be recovered from a donation as had been previously separated out, whilst doing more to preserve the longevity of the red blood cells at the same time.
SAG-M was probably introduced in September 1982.[1647] At the time it was anticipated that its use combined with the greater use of red cell concentrates instead of whole blood would enable around 75% of the plasma required for self-sufficiency to be obtained from the donations of whole blood then being made.[1648] At the regional transfusion directors’ meeting in January 1983[1649] it was recommended that SAG-M be introduced as soon as possible, and it was to be expected that it would yield a considerable increase in plasma which might be available to BPL for fractionation.[1650]
Apart from increasing donations of plasma (as to which the evidence before the Inquiry was that regional transfusion directors saw little difficulty in ensuring an increase), coupled with less use of whole blood, greater use of concentrated red blood cells and the use of SAG-M would secure close to the amount of plasma which BPL on its own could handle. Dr Lane recorded that it was in the last quarter of 1984 that plasma supplies to BPL increased as a result of SAG-M.[1651]
A further way of increasing the amount of plasma available for fractionation was to recruit more donors specifically for plasmapheresis.
Plasmapheresis first began in the United Kingdom in early 1967.[1652] It is a process in which blood is removed from the body, plasma is separated from it, either manually or by machine, and the remaining part of the donation (red blood cells and platelets) returned to the donor on the same occasion. By December 1969 it was being suggested at a meeting of regional transfusion directors that perhaps plasmapheresis should be practised more widely and rather more intensively than was currently being done.[1653] By March 1973 Dr Maycock was suggesting that extended use of plasmapheresis might be the most economical way of obtaining the plasma required for fractionation,[1654] and the Expert Group on the Treatment of Haemophilia at its meeting of 20 March 1973 suggested that increasing collection of plasma by plasmapheresis should be considered.[1655] It was also a safer base material from which to manufacture concentrates, because donations obtained by plasmapheresis were larger in volume than those recovered from donations of whole blood. The amount of plasma from one donation of whole blood was 40% of that from a donor of plasma by plasmapheresis.[1656]
The argument was not all one way in favour of plasmapheresis. Regional transfusion directors showed some resistance.[1657] The Joint Steering Committee thought that the use of plasmapheresis might be difficult to justify as a means to meet targets because it inevitably exposed donors to risk.[1658] By January 1975 the Central Committee for the NBTS expressed the view that increased plasma supplies could be achieved either by increasing concentrated red cell use or by plasmapheresis: however, ultimately it was decided not to ask donors to subject themselves to frequent plasmapheresis.[1659] This was echoed by Scottish National Blood Transfusion Service (“SNBTS”) directors, who in a meeting in June 1975 also decided not to proceed with plasmapheresis: it would be premature to do so.[1660] When the Haemophilia Society told Dr Owen about the achievements of Dr Tom Cleghorn’s plasmapheresis unit at Edgware in December 1975, a civil servant at the meeting recorded that he “explained that there were professional differences of opinion about this process.”[1661]
A fear, which inhibited the use of machine plasmapheresis, was that cardiac arrest might occur. Accordingly, a cardiac arrest team had to be available when this was practised. This made it impractical to use machine plasmapheresis for voluntary donors on a wide scale.[1662]
Over a few years, the landscape changed. Dr Angela Robinson[1663] became an enthusiast for plasmapheresis, and set up a pilot unit in Yorkshire in 1980.[1664] At the same time, Dr Gunson (now consultant adviser to the Chief Medical Officer on blood transfusion) expressed the view that plasmapheresis should be addressed further.[1665]
At this point it was clear that, in the US, pharmaceutical companies acquired their plasma almost entirely from plasmapheresis. A market in plasma had grown up. Plasma brokers obtained their plasma either from third parties who used plasmapheresis or by using plasmapheresis themselves. In the UK there had been reluctance to engage in it, despite the considerable increase in supply to which it might lead, because of fears for the safety of the donor. Machine plasmapheresis was looked upon sceptically. There were, however, mixed feelings. It was recognised how useful plasmapheresis might be in the UK, provided that it could be performed with reasonable safety.
Further movement came. In England, in 1981, Dr Gunson tabled a paper concluding that the number of plasmapheresis facilities should be increased. The Advisory Committee of the NBTS agreed to set up a Working Party, and liaise with Scotland. It was considered vital at least to consider plasmapheresis.[1666]
It was at this stage in the story (in 1982) that the availability of a new machine, the Haemonetics v50, became a turning point in the UK. A pilot study by Dr Robinson’s team showed that use of it enabled plasmapheresis more efficiently, and more safely.[1667] The plan in Scotland was now to increase the use of plasmapheresis,[1668] and no longer just to consider doing so.
Though there remained concern that the growth of plasmapheresis might deter donors[1669] and whether plasmapheresis could become an “economic proposition”,[1670] plasmapheresis slowly began to gain ground: and manual plasmapheresis to fall out of favour compared to machine plasmapheresis.[1671] Nonetheless, the routine recovery of plasma from whole blood donations, especially increased by separation of red blood cells and the use of SAG-M plasma, were still thought to be the methods of choice, with plasmapheresis making up for the deficit.[1672]
By mid 1984, studies in Scotland comparing machine and manual plasmapheresis and looking at optimal additive solution found that the cohort of plasma donors was highly motivated, there was a unanimously favourable response to machine plasmapheresis, the quality of plasma obtained was good and the costs comparable with manual plasmapheresis.[1673]
Plasmapheresis continued to grow – albeit unevenly – as a source of plasma. Thus, in 1986/87 it gave rise to just over 10% of the plasma sent to BPL.[1674] By 1989, 73% of plasma sent for fractionation came from the use of SAG-M (in plasma wedge packs), 13% from plasmapheresis and 9% from time expired blood.[1675]
Finally, the possibility of small pool freeze-dried cryoprecipitate was considered.[1676] It was thought that this might yield more Factor 8 units per litre than concentrate, because of the proportion of units inevitably sacrificed during the production of the latter, and be a safer proposition than concentrate because the pool from which it was made would consist of some 10 donors, rather than a pool contributed to by more than 1,000 donations, as was by now the case where factor concentrates were produced domestically.
Although a clinical trial was conducted in the West of Scotland, John Watt (director of PFC) saw that great practical difficulties might arise if freeze-dried cryoprecipitate were to be produced by PFC alongside Factor 8 concentrate. For these reasons, and additionally because the unit in the Law Hospital making it was closed down, such a product never gained traction in Scotland (or the UK more generally) as it had done in other parts of Europe.
Increasing the supply of plasma for fractionation could be achieved by:
Taken together, these measures would secure close to the amount of plasma which BPL on its own could handle when re-developed.
It could – and should – also have been achieved by organising the blood services so that instead of being regionalised they had a national directorate which exercised executive control. Since this would have had both a national perspective and the ability to require its regional centres to provide enough plasma to achieve centralised functions such as blood product production, this alone would have probably ensured sufficient supplies of plasma to meet the demands of fractionation. The change of structure was what regional transfusion directors, and Dr Maycock, had been calling for. It was what eventually happened – but this was more than a decade later and far too late.[1677]
Of the measures set out at (a) to (f) above, all save using single plasma packs and SAG-M were practices which could and should have been adopted in the early 1970s at the latest: the better use of blood had been recognised as important for some time before then, but both changing the culture of overuse of blood, and increasing the practice of using the red cell component of blood rather than whole blood, were not emphasised. This was probably because of a misplaced fear that clinicians might see efforts to do this as impinging on their clinical freedoms, whereas the purpose would actually have been to secure better and safer treatment for patients.
The measures of using single plasma packs and SAG-M were taken in good time, after persistence in finding the technical developments that facilitated them.
At the time that Dr David Owen told Parliament that he had authorised the expenditure of £500,000 to achieve self-sufficiency within two years, he understood that the estimates were such that 337,000 blood donations would need to be fractionated to satisfy them. He was given to understand that the production facilities were sufficient to produce what was needed (although this depended upon Scotland making a large contribution to total UK production, of which more later). Accordingly, the problem was seen as producing more plasma for fractionation and the DHSS allocated special finance to regional health authorities (“RHAs”) in 1975 in order to boost production of factor concentrate. Part of it was used centrally to provide additional equipment for BPL, and the rest was distributed to the regions for the specific purpose of increasing their supply of plasma to BPL.[1678]
After detailed discussions between the DHSS and the regional transfusion centres, the additional donations required to meet the self-sufficiency target were calculated. Five of the regions produced no fresh frozen plasma for factor concentrates at all.[1679] By contrast, Oxford and North East Thames were already producing large quantities.[1680]
The revised figures in the light of the discussions allowed for continuing use of cryoprecipitate, produced regionally. However, in some regions the effect of the proposed arrangements would be to halve the amount of cryoprecipitate which was then available.[1681] There was unease about this, not least because the demand for cryoprecipitate continued to grow throughout 1975 and 1976 in some regions.[1682]
As part of the allocation of the available funds to the regions, BPL also benefited. Arrangements were made to purchase additional laboratory equipment centrally; and for three Sharples centrifuges which were also to be provided for BPL.[1683]
By 1976/77, the special allocations appear to have become subsumed as a part of the standard regional allocations, revised “in the usual way” to take account of cost increases.[1684] Expenditure dedicated to self-sufficiency cannot thus be tracked as easily. Expenditure for 1976/77 was set at £433,000 before cost adjustments, including revenue allocations.[1685]
There were early signs that the programme was successful: in April 1976 Dr Maycock thought that the target of 340,000 donor units was likely to be reached earlier than set. By October 1976, 90% of the plasma target had been achieved.[1686] It was exceeded in July 1977 according to Roland Moyle in response to a parliamentary question.[1687]
The ability of the UK fractionation centres to convert the amount of factor concentrate available into factor concentrates for therapy was dependent upon the premises and facilities available, the yield, the system of production used, the availability of labour, and the distribution of production between the three production units.[1688]
Dr Lane became director designate in 1977, and director of BPL in 1978. He produced documents in a proof of evidence for the HIV litigation. These set out the amounts of concentrate produced and issued for “clinical use”.[1689] Dr Maycock, his predecessor, and Dr Lane, were both responsible for compiling annual reports. BPL’s perspective on its own production figures is set out in the chart below.

The production capacity of BPL was said in the documents discussed above to have been 14 million international units in 1975. The chart shows that little better than that was achieved (on BPL’s own figures) until 1980. The inadequacy of the premises was part of the reason for this. The premises at Elstree were owned by the Lister Institute until 1978. Production of factor concentrates and other blood fractions there was funded by the DHSS. However, the site was constrained. Dr Maycock said so, and strongly.[1691]
Dr Drummond Ellis was in charge of Factor 8 production at Elstree.[1692] In June 1976 he echoed the views which had been expressed by Dr Maycock and others in a minute, which examined whether production could increase to meet a target of 25 million international units per year. He said that: “Expansion to this level of production … would cause serious overcrowding of facilities, unless some additional building [is] work done … It should be noted that the existing AHF facility was not designed for the work being done and that it might be undesirable just to add extensions.”[1693]
Dr Lane was not yet involved in the management of BPL. However, from his later experience he commented that a limited expansion was possible without buildings being extended, but only as a stop-gap measure, and even this increase would require additional freezing and freeze drying capacity. There was very little further scope to manage this significant increase without additional expenditure.[1694]
The Trends Working Group, when it reported in 1977, concluded that considerable further investment in collecting, testing, processing and premises was required if self-sufficiency was to be achieved, and added “additional fractionation capacity is also needed, even allowing for some possible expansion of the Liberton plant’s output. The present UK capability is less than half of what we regard as essential. Additional major investment is, therefore, also needed for this.”[1695]
This built on a message that Dr Ellis had been conveying since January of that year. He had told the haemophilia centre directors that a figure of 14-15 million international units was the maximum capacity for Elstree with the present plant and building, and even that included a proportion made in Oxford. The figures which the Trends Working Group spoke of as needed would be at least double that. He was speaking purely of the English facilities: at that stage. SHHD suggested that Liberton had a capacity to make 60 million units of Factor 8 per year (ie four times the capacity of Elstree as it then was), although to do this would require some new capital equipment and money for extra running costs to include payment for staff to operate a 24 hour shift system of working.[1696]
In 1977, therefore, it was already clear (and had been for a while) that if the UK as a whole were to become self-sufficient then the Government would need to provide some further funds to Edinburgh to enable fuller use of the production capacities there, or to provide substantially improved, enlarged and updated production facilities for BPL, or most probably to provide some combination of both. It might have seemed that the first of these options would be easiest to achieve within a short time-scale – a point to which this Report will later return – though the third was likely to be the most practicable.
The chart above shows that the comment made by Roland Moyle to Parliament in June 1978 that BPL was already at its full capacity,[1697] was correct at the time.
Using some of the funding which had been provided by the half a million pound investment by Dr Owen, BPL’s fractionation facilities were extended slightly. Its report for the year ending July 1977 shows that the facilities had been extended to make it capable of producing 17.5 million international units. On its then site, that seems to have been the maximum achievable without further modification.
Dr Lane, in waiting as director of BPL, focussed on the view that BPL should be rebuilt. A large investment was required in order to adhere“to the Department of Health’s principle that the Health Service shall make all possible attempts to become self-sufficient.”[1698] He called for more centralised management of NBTS to coordinate plasma supply, but ultimately noted that BPL would reach its maximum accommodation by the year end, and described the present state of production as hazardous in any event due to the constraints of the laboratory conditions and workload.[1699]
In 1976 the Government had taken the decision that the premises used to produce factor concentrate in the UK should comply with the provisions of the Medicines Act 1968. They had been exempt from the rigour of these requirements by virtue of “Crown immunity”.[1700] A consequence was that by 1977, the point reached in this account, the Medicines Inspectorate were due soon to inspect the facilities at Elstree. Dr Maycock anticipated that the report would not be favourable.
To sum up thus far: by the mid 1970s, the premises in England which were designed as laboratories, and lacked the space, size, design and equipment to function as production plants, were being pressed into service to the limit of their capacity to produce blood products. This was to an extent which caused a potential danger to the public, or to those working at the facilities, because without significant modification or, ideally, replacement, production could not comply easily with then-current standards of good manufacturing process. There were potential risks to safety. Given that the Minister of State for Health had identified that the English plants had reached full capacity, the Trends Working Group had identified the extent of the shortfall, Dr Lane had expressed forceful views, and the imminence of what was expected to be a highly critical report from the Medicines Inspectorate, the fact that the inspection did not occur until April 1979 was little to the point: the writing on the wall about a continuation of production facilities in their then present form could hardly have been clearer.
A replacement on a site large enough to contain a replacement facility was plainly going to be necessary – it was already needed – and it was difficult to avoid the conclusion that planning should start without delay.
In December 1977, Dr Maycock produced a report in which he said that the
“‘stretched’ capacity of BPL will be reached about the turn of the year. The experience of the past year suggests that thereafter the laboratory will continue to work in an atmosphere of uncertainty about future development … The present method of operation will become more difficult if the scale of fractionation grows. What is needed is a programme in which each region would be responsible for carrying out a planned growth pattern within a centrally coordinated plan for the NBTS in England and Wales. Without this, or something like it, it will be difficult to plan for the future of BPL and PF Lab.
Planning the future of BPL should not wait until the problems of PFC have been resolved … It would at least dispel the feeling of uncertainty at BPL if DHSS were to say whether or not it intends to secure its investment … in PFC at the expense of developing its own fractionation potential in NBTS”[1701]
Dr Lane insisted on Dr Maycock including that last sentence. He was concerned that the belief in the DHSS as to the capacity of Edinburgh, encouraged by what he thought to be over-optimism at PFC, might result in starving BPL of the investment in redevelopment which he considered it needed.[1702]
By the end of 1976, and the start of 1977 it was apparent that the fractionation capacity in England would need significant expansion. First, though, BPL had to face the problems caused to its even continuing as it was, by the applications in March 1976 it had had to make for product and manufacturers licences, following the Minister’s decision that the NHS facilities should be treated in the same way as commercial pharmaceutical companies for the purposes of the Medicines Act.[1703]
To further complicate the picture, the Lister Institute ran BPL. It was struggling financially. In 1975 it sold premises it had occupied for several years in Chelsea. By 1978 it could no longer continue to run the Elstree enterprise, and had to sell the site it occupied there to the DHSS.
This was a reflection of what had become a time of high inflation and economic difficulty. Inflation had exceeded 20% in 1975; and GDP had declined in both 1973 and 1975. Unemployment had peaked in 1976 at 1.5 million.[1704] Public expenditure had increased markedly between 1972 and 1975, but the two succeeding years saw a sharp reversal in that trend, including the need for the Government to approach the International Monetary Fund for a loan. However, in turn, public expenditure reversed again in 1978-79.[1705]
In short, in 1977 money was exceptionally tight, but this did not mean that governmental policies already declared were not to be followed through. It nonetheless imposed constraints on the amounts of capital to be committed to them; however, one of the features of the arguments over self-sufficiency in the 1970s is that it was confidently expected that within a short time after completion of a capital project there would swiftly be a return of much or all of that capital. The savings from no longer importing very expensive products from abroad appeared substantial.
Dr Diana Walford expressed her view of the period in this way, from memory: “funding, at the time, was exceptionally constrained … ‘the elephant in the room’ for all discussions, including the redevelopment of BPL and production of additional plasma for national self-sufficiency, was that funding from the Department’s budget for centrally-funded services, such as BPL, was inadequate and capital funding was especially hard to obtain.”[1706] Thus, when it became apparent in October 1977 that any further plasma provided to BPL for fractionation would have to be dealt with in “unsatisfactory accommodation which the Medicines Inspectorate would be likely to condemn” it was decided to have a meeting to consider future production problems generally.[1707]
The DHSS thought it would be a useful occasion to take stock of the difficulties and to crystallise the possibilities for future planning. It was recognised that there was continuing pressure for more Factor 8 concentrate to be used, but BPL had reached the limit of its present production capacity. The implication of the recommendations of the Trends Working Group were that there would need to be a substantial expansion of production. Dr Lane proposed a solution. He suggested building new facilities outside the present building, re-equipping the existing shell for other associated purposes. However, for the reasons just explained, the DHSS felt that it was clear that:
“the current constraints on expenditure and the relationship existing between the Department and NHS field authorities were not conducive to the successful implementation of radical, expensive solutions to blood products production problems … Progress would most probably be achieved by concentrating on what needed to be done at BPL and a phased redevelopment solution, such as that put forward by Dr Lane, seemed to be worthy of further examination. The need to expand blood products production, provided this was done on the basis of low-cost, selective development, was now being accepted by the Department, and the importance of maintaining a separate production unit for England and Wales and of not being wholly reliant on the Scottish PFC at Liberton had recently been affirmed.”[1708]
Cost was now a major factor hindering the achievement of self-sufficiency. Though much has been made in closing submissions[1709] and some evidence has been given[1710] of the constrained financial position of the UK during the 1970s, the material available to the Inquiry suggests that the picture was more nuanced. There were “sharp increases in both public expenditure and borrowing which occurred in the years from 1972 to 1975. Public expenditure had been propelled to its highest-ever level both in absolute (real) terms and as a share of output … The succeeding years 1976/7 and 1977/8 saw a sharp reversal in this trend with very sharp falls in public expenditure, in turn reversed in 1978/9.”[1711]
It might appear from this that, given sufficient will[1712] and forward planning, there were periods during the 1970s when public money was available for capital expenditure without the financial position of the UK precluding it.[1713] It should also be borne in mind that, as was often suggested at the time, commercial concentrates were more expensive to produce than were their domestic equivalents. Successful investment in production infrastructure was thus likely to produce a continuing revenue saving.[1714]
It is difficult to avoid a conclusion that as a matter of fact, too little was done too late. The need may initially have been focussed on the provision of more plasma to be made available from the regions to a greater extent than on expanded production facilities, but it was always about both.[1715] This was known to the DHSS. The opportunity was missed.
The conclusion of the October 1977 meeting was that BPL should draw up a list of options for future developments keeping in mind the DHSS constraints.[1716] Accordingly, BPL produced a proposal designed to bridge the gap between the inadequate current plant and a new redeveloped BPL and double Factor 8 production over a four year period from 1978 to 1982. It was also intended to increase the pool size from 300 to 600 litres on grounds of efficiency.[1717] In his report on the year Dr Lane described the programme in this way:
“As its name implies, ‘Stop-Gap’ is a temporary measure to increase production, in order to go some way to meeting the recommendations of the Trends Working Party, while the future development of BPL and PF Lab is considered. The urgent need to start this deliberate planning cannot be overemphasised. Even if it were assumed that planning and building could be achieved in five years, the present BPL building would be 18 years old (in the sense that its planning and schedules of equipment were virtually completed in 1965, apart from subsequently imposed reductions) and is below the standards now regarded as necessary.”[1718]
The plan envisaged a programme of works reallocating space within the existing laboratory with some additional accommodation, upgrading certain equipment, modifying some fractionation techniques, introducing single donor bags for the supply of plasma to BPL and modest increases in staff and materials.
The plan was received positively at the DHSS. However, the proposals had to be reviewed and amended in the light of the cessation of the Lister Institute’s involvement in the running of BPL on 17 April 1978. Revised plans had to be submitted, in December 1978.
When she gave evidence, Dr Walford agreed that it was or should have been known to all those involved with BPL in the second half of the 1970s: (1) that the demand for blood products was rising; (2) that it was or should have been obvious that BPL was outdated and too small, and that significant investment was required in order to be able to meet the rising demand; and (3) that the Government had determined that BPL should meet standards equivalent to those expected of commercial plants, notwithstanding Crown immunity, but it was or should have been obvious that BPL would not meet those standards.[1719]
This had also been obvious to her predecessor, Dr Waiter.[1720] It had therefore been known to the DHSS for some years.
The Scientific and Technical Committee advising BPL made it very clear in March 1979 that there was an urgent need for planning substantial additional capacity: one member who was a biomedical engineer said “he had pointed out to the Department some 12 months ago that it was improvident to expect the major BPL plant to continue to function much longer without major breakdown.”[1721]
David Smart, who had particularly valuable experience in the pharmaceutical industry, was deputed to produce a report looking at options for BPL. He favoured complete redevelopment which should show a “rapid and growing return on the investment with all the capital expenditure paid back in the first 15 months of full-scale operation”.[1722] The view of Dr Walford was that “he was spot on.”[1723]
The Medicines Inspectorate began its long-awaited inspection of BPL in April 1979. It concluded that planning for essential improvements should begin immediately; called out for urgent action; and observed that the current position was not a recent situation.[1724]
It had not yet concluded its inspection when the Scientific and Technical Committee of the Central Blood Laboratories Authority (“CBLA”) met in June. The Committee was briefed that serious deficiencies had however been found in practically all aspects of the laboratory examined so far, for example in documentation, quality control, environmental control, availability of pharmaceutical advice and in the scheme for training staff. “Although it might be some time before the Inspectors report would be available it was apparent that changes were needed at BPL”. Disquiet was again expressed by the Scientific and Technical Committee that nothing had been done already to put the defects at BPL right.[1725] Urgent action was needed.
It was at this point that the Health Services Division of the DHSS[1726] became concerned that the costs of upgrading under the stop-gap proposals could result in a situation where the government would have to choose between upgrading on the one hand, and going ahead with the stop-gap on the other hand. The DHSS therefore said that no money would be available for either.[1727] This decision not to take a decision caused delay in achieving whichever option was eventually to be chosen.
Within a fortnight, the report was signed off. It was every bit as damning as had been predicted. The inspectors identified that BPL could not be readily adapted to large-scale manufacture; personnel had not had the opportunity to gain experience of modern large-scale production requirements in the pharmaceutical industry; production had outgrown the premises in which it was undertaken; and the laboratory was so short of space for cold storage, quarantine of raw materials, in-process materials and finished products, receipt and dispatch, packaging and warehousing generally that it was neither practical nor safe to increase throughput, even if the necessary production facilities had been available. “If this were a commercial operation we would have no hesitation in recommending that manufacture should cease until the facility was upgraded to a minimum acceptable level.” Notwithstanding that, its conclusion was that “as blood products are essential to the health and well-being of the nation and as alternative sources of supply are severely restricted, production at Elstree may continue provided that certain aspects of standards of production and control are improved immediately and that the planning of other essential improvements in these standards commences immediately with a view to very early implementation.”[1728]
On 7 September the Department’s Inspection Action Group concluded that the Inspectorate’s Report revealed that the production, control and other arrangements at BPL fell so short of the standards required of commercial establishments that had the BPL not enjoyed Crown privilege the Group would have felt bound to recommend immediate suspension of activities. It chose not to recommend this. It did so because it took the view that a) the NHS was heavily dependent on BPL’s blood products; b) existing production was understood to be barely adequate and a break in production was likely to interfere with essential supplies to patients; c) alternative supplies of all materials were not available; d) there was no guarantee that such alternative supplies of some products as were available were safer than those produced by BPL;[1729] and e) it was unaware of any weight of established evidence that BPL’s products had caused harm to patients.[1730]
In September 1979 there was another meeting of the Scientific and Technical Committee for the Central Blood Laboratories. The members did not support commercial development, and recommended that no time should be lost in planning a completely new NHS plant, even if it was felt that other possibilities had to be examined concurrently. David Smart’s estimate from his experience was that a new plant could be achieved in three years.[1731]
John Harley later wrote a memo which reflected his recollection of the Committee. He said that he had tried without success to discourage Professor Patrick Mollison (the chair of the Scientific and Technical Committee) from initiating planning because no decision had yet been taken to build a new fractionation plant at BPL and there was no budget even for the preparation of a development plan.[1732]
In December 1979 a submission was made to ministers on the future of BPL.[1733] They were asked to consider and agree: (a) that there should be a short-term upgrade to BPL, accepting that it would fall short of the full recommendations of the Medicines Inspectorate; (b) a decision in principle to rebuild BPL but without commitment to method or timing; and (c) further exploration of options for rebuilding within the NHS or in collaboration with industry.[1734] In January 1980 Dr Gerard Vaughan, current Minister of State for Health, agreed to the first and third of those proposals.[1735] There was thus no commitment even to a decision in principle to rebuild BPL.
In February 1980 Dr Lane was authorised to proceed with the stop-gap project. The DHSS anticipated that the sum of £750,000 would be available for the capital development of BPL in 1980/1981.[1736] Dr Lane’s view was that even relatively short-term redevelopment projects would cost more, and possibly as much as £2-2.5 million over two to three years.[1737]
In April 1980 ministers asked to see whether there might be scope for further savings in the stop-gap measures. They were concerned that there might be no justification to incur short-term costs on upgrading if BPL was to be rebuilt. The minister’s position was thus understood to be that expenditure should be limited to matters of necessity.[1738] Accordingly, in May 1980 Dr Lane sent a revised programme of works for BPL to John Harley at the DHSS. The proposal was named MARP01 to distinguish it from the previous stop-gap proposals.[1739] He was then asked at a meeting in June to put forward proposals on the basis that only £500,000 was available to spend on short-term developments at BPL.[1740]
Eventually, on 29 July 1980, Dr Vaughan approved a submission that had been put to him proposing expenditure of £1.3 million over two years. He rejected options involving lesser expenditure.[1741] It was not, however, until 2 February 1981 that Dr Lane was given formal authority to proceed to tender with MARP01: this was because the regional health authority which was the client for the purposes of the redevelopment work had insisted on considering the proposals and changes to those proposals before authorising the works.[1742]
Ministers decided to defer the eventual decision on whether to build a new laboratory within the NHS until other possibilities had been investigated.[1743] The investigation showed that “no British firm had the necessary expertise in the manufacture of blood products and only foreign firms had approached the Department, with a view to processing British plasma on the existing basis and, in addition, to processing and re-exporting plasma from overseas.”[1744] According to Dr Walford, by May the Deputy CMO, Dr Harris, was “exasperated”:
“Q: Because he thought ministers were taking the wrong course?
A: There was a clear course of action which was necessary at that time. It was barn-door obvious, and yet somehow or other, it wasn’t possible to make progress, and so what Dr Harris was doing there was actually saying ‘We must get on’; he was encouraging that the final submissions should go to ministers; and that … ministers should be encouraged to understand that at the end of the day they took responsibility if something went wrong.
Q: Is it right to understand we’re still talking about what should be done in the short-term here?
A: Absolutely in terms of keeping things going for the short-term, but there had to be a commitment to rebuild because without that clearly the entire edifice was not going to be fit for purpose.”[1745]
Long-term upgrading was considered in September 1980 by the Scientific and Technical Committee.[1746] It was reported to the Committee that officials had been instructed by ministers to investigate the possibility of collaborating with private industry. Initial discussions had taken place and a paper was due to be sent to ministers setting out the pros and cons of such an arrangement.[1747]
Worries were expressed about various aspects of this, including the fear that it would be “impossible to prevent the contamination of the UK material with imported hepatitis viruses.”[1748] A collaboration with Beecham was considered.
A submission went to ministers on 14 November 1980. In that document Peter Wormald of the DHSS said that it was important “we should reach a decision in principle now: that is we should either reject the commercial option or decide that we intend to implement it subject to satisfactory negotiations. A decision merely to continue negotiations, without commitment in principle, would prolong uncertainty, encourage continued argument and further damage morale at BPL. And it would not be fair to Beecham.”[1749]
This time, there was a decision. Dr Vaughan announced that there would be “no commercial management of Blood Products Laboratory: modernisation programme already underway.”[1750]
In December 1980, more than eighteen months after the Medicines Inspectorate report, and a number of years after it had become clear that a new fractionation plant was needed (whoever was to run it) ministers instructed officials to begin work on planning and designing a new BPL.[1751] Up to this point, Dr Walford in her evidence agreed with the view contemporaneously expressed by Dr Peter Dunnill.[1752] She said that “it had been a totally chaotic, protracted and difficult process, and needlessly so”. She remembered her frustration about “innumerable and repetitive meetings which generally ended without moving matters forward to any appreciable extent.”[1753]
Although planning and designing what might be a new BPL had been authorised, there had yet been no decision in principle to actually get on and build it. Indeed, by October, ten months further on, a minister asked the Policy Steering Group for the redevelopment of BPL to give consideration to the use of an existing factory which could be adapted at a relatively low cost to meet requirements.[1754] No such building could be found.[1755]
A lack of ministerial decision, ministerial uncertainty, and the absence of long-term management arrangements now complicated matters further.[1756] By March 1982 approval was sought for planning to proceed on the assumption that BPL would process all plasma for England and Wales since PFC did not have additional capacity without introducing three shifts.[1757]
In July 1982, the Policy Steering Group proposed a new laboratory be built at BPL at a cost of £21.1 million spread over the years 1982/83 to 1985/86.[1758] The Treasury then approved the redevelopment in principle, and agreed that the project should be “fast-tracked.”[1759] Final approval was given for redevelopment in the sum of £22.6 million on 11 November 1982.[1760]
Finally, on 1 December 1982, a special health authority was established to take responsibility for the management of BPL, PFL in Oxford and the Blood Reference Group Laboratory. This provided a management structure which had been thought lacking and was thought necessary for any redeveloped premises.[1761]
The first programme of works had been limited by financial constraints, identified broadly above. One of the aims of these stop-gap works had been to allow for production to be expanded: this was despite the Medicines Inspectorate recommending in their report that no expansion should take place until the concerns identified in that report had been addressed.[1762] Despite the decision to waive Crown immunity, some flexibility was permitted for NHS facilities. Although manufacturing licences were not mandated by statute for NHS manufacturing facilities, the policy was that they should nonetheless comply with the standards which the Medicines Division would require commercial firms to observe.[1763]
In a later report of 4 February 1986, Dr Lane said that the final cost of MARP01 was £2.8 million. He thought that a significant part of this inflated figure was “absorbed by repetitive design and interruptions in implementation” and by “simple procedural problems” such as, for instance, the role of North West Thames regional health authority as the nominal client, despite the project being funded centrally by the Treasury through the BPL budget.[1764]
Construction finally began in May 1983. The original completion date was to be July 1985.[1765] In a written parliamentary answer about this, Kenneth Clarke, the Minister of State for Health, stated that “the Government decided in 1982 that self-sufficiency in all blood products … should be achieved, and that the Blood Products Laboratory at Elstree should be rebuilt to provide the capacity to manufacture the blood product needs of the National Health Service in England and Wales.” It was then said to be on time for completion in January 1986.[1766]
Kenneth Clarke repeated this in February 1985: “We decided in 1982 that this country should become self-sufficient in blood products.”[1767] Lord Owen reacted to the opening words, since in his view (correctly) there had never been a time since his announcement of the policy of self-sufficiency when it had not been government policy to do so. He told this Inquiry that it was “extremely odd” and “as if the previous Labour Government programme had never existed.”[1768] This perhaps serves most to emphasise the fact that little seemed to have been achieved towards implementing that policy since 1977, such that it may have seemed to many to have “dropped off the radar”.
It was eventually finished at a cost of £60 million with an additional £7 million for essential extras in summer 1987. The estimated date for achieving self-sufficiency slipped from 1986 to 1989.[1769]
Documents from 1986 record ministers saying that the project had been “badly handled”[1770] and a “shambles”.[1771] Lord Norman Fowler told the Inquiry that the overspend on the project “reflects poorly on the Department”.[1772] His evidence, and the contemporaneous documents, suggest that what contributed to delays and expense included: underestimation of the initial project during the tender stage;[1773] the complexity of the plant and the build;[1774] the various re-designs which took place during the project, in part due to new technology, and in part due to the fast-track “design and build” approach; poor management by the CBLA; and a lack of close oversight by the DHSS.[1775] Nonetheless, Lord Fowler also pointed to some favourable features: the building was probably completed two to three years earlier than would have been the case with “conventional methods”;[1776] an incoming chief executive of the CBLA, who was not implicated in the project’s history, is reported to have told officials that on the basis of a lifetime’s experience in the pharmaceutical industry the building represented value for money.[1777] He noted that ministers invested money at a very considerable level, especially given the financial pressures on health spending: it was given priority at the expense of other pressing needs.[1778]
The principal reason why self-sufficiency was not achieved in England and Wales until after 1990 was that it was only then that BPL in its redeveloped form came fully on stream. It is highly likely that if this had been achieved significantly earlier there would have been less infection, in particular with HIV. Opportunities were missed. As early as 1967 Dr Rosemary Biggs had anticipated a need to ensure that the production of factor concentrates in the UK would be sufficient to avoid a need to purchase expensive commercial concentrates from abroad. She had identified the risk of insufficiency, and she was a leading clinician, at a leading treatment centre. Nor, as set out above, was she in any sense a lone voice. Scotland took note of the same risk, and broadly achieved self-sufficiency as a result. Although there was sufficient product in the rest of the UK (whether it was cryoprecipitate or concentrate, or both) for treatment without the need to import from abroad until around 1973, and arguably for a brief while thereafter, the writing on the wall was clear. A desire to promote home treatment, coupled with the increasing lifespan of people with haemophilia once cryoprecipitate began to be used after 1966, and evidence of a growing demand for concentrate from centres such as the Oxford Haemophilia Centre, showed that BPL was ever likely to be called upon to produce more. It needed to be put in a position to do so, both by sufficient supplies of plasma and adequate, safe, modern production facilities.
A number of factors hindered the achievement of this. There was no overall, nor any coherent, plan to provide factor replacement therapies to treat clotting disorders. The supply of plasma for fractionation was initially inadequate. This was largely because of the structure of the NBTS, which had no power to direct that supply, and because of the way that finance for that supply was regionally determined. However, it was the inability of BPL to process the quantities that would be necessary to meet the 1977 estimates, let alone the increased demands thereafter, which proved the main problem.
The production capabilities of BPL and PFL combined were insufficient largely because the premises were being pressed into service as production units when they were never designed for that purpose. There was no sufficient thought given by Government to meet the future needs of haemophilia therapy in England, Wales and Northern Ireland (although there was such forward planning in relation to Scotland); and nothing was done to meet the urgent need for revamping or replacing BPL which had been apparent throughout most of the 1970s. Though BPL was upgraded in 1972, Dr Maycock’s observations about BPL as it was speak of its inadequacy. It is plain from what he and others were saying in the first half of the 1970s that far better facilities needed to be provided at BPL, and this could not be done without a substantial redevelopment of some kind.
Civil servants in the DHSS were well aware of these matters. The paper written by Thomas Dutton in 1976 was insightful in identifying the problems of the previous few years. It described devising and effectively managing a balanced programme for the preparation and distribution of blood components including clotting factors as “probably the most urgent task facing the NBTS”. It spoke of a need to fractionate something approaching one million blood donations annually, substantially more than the amount which BPL was then capable of achieving, and the plasma to make which was not being made available by regional health authorities. It was plain from his paper that one difficulty was achieving the supply of sufficient plasma to BPL to enable it to fractionate sufficient Factor 8 concentrate; but it is also clear that it was recognised within the DHSS that the production facilities were unlikely to be adequate.[1779]
Dr Owen’s initiative resulted in a greater supply of plasma, and helped to assure that such a supply would be able to continue. However, the improvement in supply rapidly demonstrated the bottleneck in the system in England, Wales and Northern Ireland – the lack of facilities to produce sufficient Factor 8 concentrates domestically: by 1978 both BPL and PFL were recognised by the government to be “working at present full capacity”,[1780] and it must have been realised a year earlier, when the 1975 target of 340,000 donor units was met,[1781] how little headroom was left before hitting this ceiling.
There was no planning in time to meet this anticipated need. Dr Walford was correct when she said that Dr Lane was right to describe the difficulties in meeting the problems of the NBTS as having been “accentuated by the growth in requirement during the 1970s of plasma products, an exercise in production maintained without adequate planning, co-ordination or finance from the outset.”[1782] She agreed that there appeared to be no overarching plan in order to achieve self-sufficiency. Yet self-sufficiency was government policy from the end of 1974.
Regional health authorities were described by Dr Walford as “fiefdoms”;[1783] they decided how best to allocate their resources to the needs of their region as they perceived them. Minority needs, such as those of people with haemophilia, suffered by comparison with many of the other matters on which a health authority might wish to spend its money. The system gave little incentive to a regional health authority to collect plasma from within its region, freeze it quickly, and send it to BPL for fractionation. There was no guarantee of any return upon the expense incurred in doing so.
The decision was taken in 1974/75 that self-sufficiency was important. It was to be achieved. Peter Wormald, Under-Secretary in the DHSS, understood that the reasons for the policy were “that imported products were very expensive and in general were considered to carry much higher risk of cross-infections, particularly hepatitis”.[1784] It was important for these reasons, but also because the WHO had recommended it; in part because it was appreciated as a matter of principle that plasma sourced in a region in which some diseases were endemic would risk transmitting those diseases to the country to which it, and any product made from it, was exported.[1785] It was achieved (far) too late.
On the evidence, there was always likely to be sufficient cryoprecipitate capable of being produced to meet the demand for that form of haemophilia therapy. However, clinicians, and no doubt many patients too, wished for the added advantages which factor concentrates offered, particularly in terms of home therapy.[1786] Belief that factor concentrates were needed, rather than highly desirable, in part fuelled the drive to produce such concentrates domestically. The main problems essentially started first, before David Owen’s initiative took effect, with securing a sufficient supply of plasma, through a system which was uncoordinated; and which depended on the extent to which plasma could be recovered from donations made of whole blood. The more that blood could be separated into the components in which it was really needed, the more plasma was more likely to be available for fractionation. This however, depended upon a willingness amongst clinicians who used transfusion in their practice being prepared to accept concentrated red blood cells rather than whole blood. Blood was collected as whole blood, when there was room for some plasmapheresis. The provision of plasmapheresis in England was slow to be initiated. Much of the need to import factor concentrates (and the additional disease they brought with them), was an overenthusiasm amongst the treating clinician for the advantages of factor concentrate without paying enough regard to the downside risks of exposing patients to the viruses that they knew that those concentrates were likely to contain (hepatitis) and those they might have supposed to be there (unknown viruses which could do damage and which were more prevalent in the countries from which the product came). Clinicians accepted that the risk was inevitable, rather than seeking to reduce it. Categorising the risk in this way made the use of commercial products more acceptable.
The second major problem was that if plasma was supplied in the quantities needed for a sufficiency of concentrate, the production facilities needed to manufacture that sufficiency from that supply were simply lacking.
It is difficult to differ from the view expressed by Dr Walford that the process in deciding to develop BPL had been “totally chaotic, protracted and difficult” and “needlessly so”.[1787] The delay between April 1979, when the Medicines Inspectorate conducted their inspection and condemned the premises operated for BPL as unsuitable for a pharmaceutical company, and the middle of May 1983, when construction began, was just over four years. Dr Walford was right to describe the delays as “unconscionable”.[1788] The central problem that led to this delay was ministers being unable to make a decision, in part because of the consequential capital expense. But it was obvious that significant expense would be incurred whether or not the plant was operated by a British pharmaceutical company or BPL.[1789] Moreover, to look at April 1979 is to look at the wrong date as a starting point. It should have been no later than the end of 1976, when it was already known that the premises in which BPL operated were unsatisfactory, unsuitable, liable to be condemned by the Medicines Inspectorate, and simply could not produce enough products to meet the government’s, the profession’s and the patients’ requirements. The failure to make full use of the Scottish facility contributed significantly to the problems with supply.[1790]
On the available information, for periods during the 1970s the public finances were significantly stretched. However, planning for a new facility should have begun: it was plainly going to be needed if the policy announced by Dr Owen were to be achieved. It was government policy. It never ceased being government policy. The failure to achieve it is a sorry tale.
The Department of Health and Social Care (“DHSC”) was right to submit that in 1973 the forecasts for the factor concentrates that might be needed had not yet been made.[1791] However, as the facts set out above show, a potential need had already been signalled (both in Scotland, and by Dr Biggs); was put forward by the MRC Working Party in 1974,[1792] and by 1976, as Thomas Dutton’s paper shows, it was clear that redeveloped premises would be required not only because of their own shortcomings, described above, but to meet what was by then to be anticipated as demand grew. By October 1977, if not before, the need for redevelopment had become irrefutable.
The DHSC then points to the withdrawal of the Lister Institute from the running of BPL, the constraints of the site BPL occupied, and the time it took to purchase land from the Lister Institute to enable expansion.[1793] It has asked the Inquiry to consider delays caused by the effects of the Medicines Inspectorate report, the stop-gap improvements (and consideration of how far and at what expense they could be carried out if there was to be a development at public expense), the possibilities that private industry might be involved in a rebuilt plant, and the financial constraints upon the health service and the state more generally. These, it is submitted, explain the delays.
The points made in the evidence of Dr Walford, as set out above; the length of time it took to actually make a decision to proceed (when it was, as Dr Walford put it, “barn-door obvious” what that decision should be), and the length of time the issue had been brewing – BPL as a production facility was condemned by the Medicines Inspectorate in 1979, and the deterioration to a state in which it could simply not go on as it was had been seen to be coming by Dr Maycock in the early 1970s, and must have been visible to observers – compel the conclusion that despite these submissions the findings set out above are right.
In wartime planning, two main plants were to process plasma for the UK: one south, one north.[1794] Some idea of the proposed split of production between the central processing plants as they had by then become was given in 1965. Dr Cumming was an enthusiastic advocate of forward planning.[1795] The Ministry of Health agreed with the SHHD, informed by Dr Cumming’s views, that PFC would fractionate plasma for the NHS using plasma collected by the Newcastle, Leeds, Manchester and Liverpool regions, leading to Antihaemophilic Globulin (“AHG”) from 10,000 bottles of blood.[1796] It was supposed that the Scottish facility would supply at least one third of the UK need for AHG, ensuring that the extra costs of Scotland providing for England would be recoverable from central government.[1797]
The SHHD suggested that there should be a management policy committee covering both BPL and PFC to ensure that a common production policy would apply to both laboratories.[1798] This eventually happened in 1973 when a Joint Steering Committee[1799] was set up to consider common policies on, amongst other things, which of BPL and PFC was to fractionate what products and in what amounts, the provision of plasma to PFC from south of the border, which country was to supply which region, and the standardisation of blood products. It was precipitated by the grant of product licences to two commercial firms “which might entail large sums being spent by NHS authorities on these products.”[1800] The Scottish CMO, Sir John Brotherson, wrote from Scotland offering further support for production capabilities south of the border, saying “It has been represented to me by clinical colleagues that this is an initial step which will lead to the purchasing of human donor blood in this country, with consequent erosion of the voluntary donor principle. Clearly apart from its social unacceptability and the consternation that this would cause in our Blood Transfusion Services, the cost implications for the Health Service could be very substantial.”[1801]
By 9 May 1968 it had been decided that 1,000 litres of fresh or fresh frozen plasma could be processed weekly by PFC, using pools of eight litres. This size of pool could be handled conveniently and quickly and was supported by clinicians using the material.[1802] It was reckoned that if the north of England utilised PFC fully Edinburgh might have to cope with 2,500-3,000 litres per week.[1803] Importantly, “Mr. Watt considered that, as there was only a small possibility of expansion at Elstree, Edinburgh should be prepared to cope with the requirements of a larger part of England than originally intended so that the total growth of requirement could be handled by the two Blood Products Units. Dr Maycock considered this approach to long-term planning was the only correct procedure.”[1804]
The SHHD’s proposal that the new blood products unit “should operate on the continuous flow principle and should be designed to a workload of 1,500 litres of plasma per week; but it will be capable of adaptation, without substantial structural alterations, to operate at levels up to 3,000 litres per week should this become necessary” was approved in principle in October 1968.[1805]
The following month, it became clear that PFC’s construction would cost more than the sum approved, and that despite a planned 1,500 litre capacity, it would for this financial reason only be equipped initially to operate at 1,000 litres per week. This would reduce the estimated cost.[1806]
It had already been agreed that Scotland could make a charge on the English regions it supplied with AHG once it was operational. In December 1968, presumably in light of the same financial pressures, the SHHD sought a contribution from the DHSS for the capital cost of Liberton in return for not including any element of capital charge in the amounts due when blood products were later to be supplied. Based on the supposed extent of the supply of finished product to English regions, England’s share of the capital cost would come to more than one third. In the event, the DHSS eventually invested £400,000 in PFC towards the capital costs,[1807] which would amount to somewhere between a quarter and a third of the costs as then estimated.
In March 1969, in line with the approach thus far, Dr Maycock indicated that he expected one third of the plasma from England would be processed at Liberton.[1808]
The delays which had already occurred were such that at the end of December 1969, when a final cost estimate was approved, it was known to be unlikely that PFC would begin production before the end of 1973.[1809] Construction began in 1971. It continued until 1974. It then progressively, though slowly, came on stream.[1810]
As noted earlier in this report, the Expert Group on the Treatment of Haemophilia emphasised the importance of taking a UK view of provision for haemophilia therapy: it considered such a unitary view “essential”.[1811]
John Watt was the director of PFC whilst it was in development and for some time after. His view was that PFC was designed just to handle a minimum of 1,500 litres of plasma per week working on a 46 week year but with capacity to increase to at least 3,000 litres per week.[1812] At the minimum level of working, it was expected that 1,000 litres of plasma would come from Scotland each week, and the remaining 500 litres would come from England. John Watt observed: “How this will work in practice is difficult to define at the present time[1813] since there is no plasma available in England to send to Scotland. Elstree is, for the present, able to absorb all available plasma from the English Blood Transfusion Service. This is a matter for some concern since it affects the economic viability of this Centre.”[1814]
In his evidence, Dr Peter Foster was able to explain that, in the light of John Watt’s experience around the world as a consultant, a fractionation centre should support a population of at least 15 million to be economically viable. “So the population of Scotland was too small, in his opinion, for this to be economically viable, and that is why he saw England as being essential to the future survival of PFC, as well as obviously to the benefit of England.”[1815]
As PFC came more fully on stream, in 1976, the SHHD asked the DHSS when PFC would be provided with English plasma for fractionation.[1816] The reply was, essentially,“Not yet.” The programme to secure plasma for the production of Factor 8 blood products in England and Wales was underway in order to meet Dr Owen’s pledge to achieve self-sufficiency, but an increase in plasma supply was not anticipated “for some months yet.” BPL was said to be able to process all supplies in England and Wales for at least another year though the situation would be kept under review.[1817]
In 1976, nonetheless, ministers continued to stress the need for collaboration between Scotland and England in manufacturing blood products.[1818]
As mentioned above – repeated here to give a coherent account of what happened in respect of PFC – a haemophilia centre directors’ meeting was told in January 1977 that the maximum capacity of BPL at Elstree with its existing facilities was 14-15 million international units of Factor 8. Yet it appeared that 40-50 million units would be required for self-sufficiency. Dr George McDonald, from Glasgow, told the meeting that PFC had the capacity to make 60 million units a year but to do this would require finance for additional equipment and running costs including staff payments to enable a 24-hour shift work system. The minutes record that agreement in principle had been reached between the DHSS and SHHD and “plans had been made to divert plasma from south of the border to Liberton when Mr Watt was ready to receive it. It was planned that the factor VIII from this plasma would return to Centres south of the Border.”[1819]
There is evidence that PFC then received some plasma from England in 1977. By July 1977, the amount received totalled 20,000 litres. But that is where it stopped. In July at a meeting of the directors of SNBTS, PFC and SHHD, it was agreed that “a system acceptable both to BTS England and Wales and to SNBTS would have to be evolved”before further supplies were arranged,and the need for this“should be borne in mind by those presently negotiating the supply of plasma from England to PFC.”[1820]
By January 1978 no further plasma had yet been supplied from England. It was again agreed that a detailed plan was needed before large scale processing of plasma from England and Wales should begin in Scotland.[1821] The meeting agreed that Scotland should provide for its own supply of fractions before undertaking work for the NBTS in England.[1822]
Thus, by the start of 1978, the position could be summarised in this way: during the Second World War and immediately afterwards it had been seen as necessary that there should be two large plants – one south and one north – between them covering the demands of the UK as a whole for blood products.[1823] After AHG was first developed in the late 1950s, it was foreseen that a demand for it as a concentrated form of therapy was likely to grow. Accordingly, planning for a new premises in Scotland included provision for making it. Scotland was to share UK production of this with the existing facilities at Elstree. Those premises were in need of some modernisation, and their capacity was limited. Planning proceeded on a UK-wide basis since, on this basis, the northern unit, being in Edinburgh, was intended to serve not only Scotland but also the north of England; and Elstree might not be capable of producing enough. The DHSS paid a substantial proportion of the capital cost of PFC development on this basis.
Throughout the early 1970s it had been said, repeatedly, at meetings of different committees, by the DHSS, and by the minister concerned, that PFC and BPL should together supply the UK with the necessary blood products. As a unit, the commercial viability of PFC as newly built was questionable if it were only to serve the population of Scotland. Matters even went as far as some plasma being supplied from England to Scotland for fractionation. But what never happened was a final agreement on detail: as to the amount of plasma which PFC would be asked to fractionate; how much of that would be fresh frozen plasma from which factor concentrates could be made, and how much would be time-expired plasma; the arrangement under which northern regions of England would, out of their own budgets, finance the production of plasma to a plant outside the scope of the NBTS for return as concentrate;[1824] and the level at which Scotland would be reimbursed for the expense in making provision otherwise free of charge to the English regions.[1825]
It is also plain from the earlier part of this chapter that BPL did not have the capacity by 1977 to produce the amounts of Factor 8 concentrate demanded by clinicians in England. Those demands could not be satisfied in the immediate future without reliance either on importing products from America, or making use of PFC in Liberton.
Despite this history, and what might seem its logical endpoint (namely the use of PFC), a U-turn was signalled on 22 August 1977.
On that date a joint meeting between the DHSS and SHHD was held to discuss mutual problems. Dr Maycock had written to the DHSS to the effect that 25,000 litres of plasma per year (500 litres per week) would be available for fractionation by PFC, and it was thought that supply of this could begin in the autumn.[1826] The product required would be plasma protein fraction.[1827] The minutes record that:
“Dr Lane, who was to succeed Mr Maycock in about 12 months time said that it was his intention to concentrate on the production of Factor VIII at the BPL. The latter and the laboratory at Oxford, were both funded by DHSS and it would be wrong, in his view, to send plasma from Regional Transfusion Centres in England to the PFC, if this had the effect of leaving spare capacity at Elstree and meant service charges having to be paid. In his view this would have the effect of duplicating costs. He envisaged that only time expired plasma would be sent to the PFC and was unwilling to enter into any long term agreement to have regular quantities of plasma fractionated in Edinburgh.”[1828]
It was pointed out that any fundamental departure at this stage from what had already been agreed about the fractionation by PFC of plasma from England could seriously jeopardise the working arrangements at PFC, and in particular could raise questions about the need to introduce shift working. While PFC could function with or without plasma from England, a sustained commitment to processing English plasma required agreement on regular quantities of plasma, providing continuity of production over a period of some years.[1829]
John Watt saw the implications of what had been said at the meeting, in particular by Dr Lane. He recognised it as a reversal of the pre-1967 agreement that PFC would receive plasma from the five northern regions of the NBTS. He realised that Dr Lane considered Scotland should not produce any factor concentrates for England. Dr Lane saw PFC as being useful to England only for recovering albumin from time-expired plasma, and saw even this only as a short-term arrangement which would be reviewed on an annual basis.[1830]
It had apparently been said in the meeting that there had never been any intention for NBTS northern regions to be delegated to supply plasma to Scotland. In light of the history set out above, much of which John Watt repeated in his indignant letter, he regarded this as simply incorrect. The documents produced to the Inquiry show that he was right on this.
He went on to note that
“it is my own belief, supported by the Working Group on Trends in Demand for Blood Products, that the UK requires to process plasma at a rate of about 10 000 litres per week. That is about 2.75 million donations of plasma per year. There is capacity potentially available for this purpose in the country as a whole and, adopting the spirit of the first joint meeting, this does not require any major rebuilding in Scotland or in England.”
He commented that the views expressed were “surprising since they followed on the decisions of the first meeting of the group that it was the intention of the group to consider, plan and act on problems for the processing of plasma on a UK basis and that the two main centres would proceed on an equal status and not on the basis of a master/servant relationship.”[1831]
The problem of securing an agreement acceptable to the workforce if asked to run a 24- hour shift system (which would be necessary if plasma from England was to be processed by PFC to any considerable extent) led to a letter from the SHHD, in which a possible solution was proposed.[1832] The letter appears to have provoked an internal memo within the DHSS:
“even if all the difficulties in shift working at Liberton could be overcome tomorrow, it would not be regarded as sensible policy to put all our eggs in the Scottish basket as the planners appear to have originally intended. We must concentrate much more of our attention on building up the capacity of Elstree so that in normal times it would provide us in England and Wales with our full requirements of the key products identified by the Trends Working Party. (Albumins and Factor VIII) without the necessity of dependence on Liberton … I am bound to admit that it is difficult to see how the Scots could function effectively at Liberton on anything like full capacity without guaranteed supplies of plasma from England and Wales. And if by some means this problem of input could be resolved, there would still remain the difficulty of possible over-production of some at least, of the blood products. What may be needed is a complete re-appraisal of their sources of supply and outlets for production, including a possible export market. But this is for the Scots, not ourselves, to institute. We are attempting our own review exercise for England and Wales, as I have said, based on the realisation that a fully integrated ‘UK’ approach to the fractionation of blood plasma is not a practical proposition, and this is causing us headaches enough. However, it is not going to be easy to disentangle ourselves from the implied moral (and actual financial) commitment that our predecessors undertook in connection with the building of Liberton.”[1833]
This memo cannot pass without comment. The underlying assumption in the memo was that development at Elstree rather than utilisation of an existing plant of PFC was what was needed. The suggestion that “all our eggs”will be put in the Scottish basket is a gross overstatement: the proposal had actually been for an equitable division between the two units, one south and one north, for the whole of the UK. No reasons are given for “the realisation”that a fully integrated UK approach was not practical. Yet the author recognises that if his proposal is to be accepted it will make life exceptionally difficult for PFC, and that he is proposing an action which reneges on a commitment. Since Roland Moyle would say the following summer in Parliament that BPL was working at full capacity,[1834] it might appear that the policy goal of self-sufficiency was being sacrificed on the altar of “England for the English” and “Scotland for the Scottish”.
Since, about this time, it had become apparent that Elstree was in need of complete overhaul or replacement, and might face the condemnation of the Medicines Inspectorate, it might be that the author was motivated by a desire to see a bigger and better BPL built, and feared that might not happen if it were only going to receive plasma from the southern two thirds of England. That ultimately should have been a decision for ministers. A surprising aspect of the change from a joint UK approach in which Scottish participation was essential is that there appears to have been no ministerial involvement. This is despite what might be seen as a U-turn on policy, the abandonment of a “UK approach”which had been endorsed by ministers previously, and pursuing a policy which would make much of an existing plant in Scotland redundant despite the investment which the UK as a whole had made in its construction. Views of this type, and those of Dr Lane, in effect marked the death knell for a contribution from the Edinburgh plant towards a goal of self-sufficiency. Though on its own PFC may not have been able to achieve it, a very substantial contribution could have been made.
This approach was misguided. It proved harmful. It was determined without direct ministerial involvement. It prevented the UK-wide achievement of self-sufficiency.
Relations between Dr Lane and John Watt were part of the history that led to this. They were never good. Dr Lane belittled the claims made by John Watt for the production capabilities of PFC and for its claims in respect of yield.[1835] John Watt (and SNBTS generally) thought that those in England had underestimated the likely demand. They would have known that Dr Lane’s approach was Anglo-centric, and focussed upon achieving a bigger and better BPL, which he was to lead as director. They must, also, have considered that the change of director from Dr Maycock to Dr Lane caused a change in policy toward the contribution Scotland could make to the UK.
Matters might have rested there. There was nonetheless further consideration of the possibility that PFC might make a contribution to the supply of factor concentrates in the UK.[1836] On 20 June 1979, John Harley and Thomas Dutton from the DHSS visited SHHD and Liberton, meeting a number of people from both. John Harley reported to the Under-Secretary, Peter Wormald, that Liberton had spare capacity, and recommended that the question of England’s use of that capacity should be re-opened. He recorded that there would be difficulties and suggested how they should be tackled, beginning by asking the Scientific and Technical Committee to investigate problems relating to the quality of materials and products and to determine standards acceptable to both England and Scotland. Peter Wormald asked him to proceed. He recalled:
“There appear to have been some follow-up discussions, but I was not copied into the papers and I do not know what action, if any, resulted. It is possible that the discussions took a back seat in September when the Medicines Inspectors’ report on BPL was presented. However, I remained keen to get a return on our investment in Liberton. Greater point and urgency was given to consideration of this (a) by the Medicines Inspectors’ report on BPL, and because of the need to plan the long term capacity of BPL or whatever was to succeed it; and (b) because of the desirability of reducing purchases of commercial blood products.”[1837]
He noted that “although no decision had been yet on the redevelopment of BPL, there was a need to determine its future capacity; which in turn raised the issue of what part Liberton would play in meeting capacity.”[1838]
In September 1980 Dr Walford visited PFC, with colleagues, and understood from her visit that “Liberton had a substantial capacity for expansion” notwithstanding “substantial”staffing difficulties.[1839]
In 1981 a trial of shift working was conducted at Edinburgh.[1840]
By October 1981, some 90% of the blood products used in Scotland were manufactured in Edinburgh, making Scotland virtually self-sufficient.[1841] John Watt is recorded as having nonetheless stressed that the plant was considerably underutilised and could process blood to serve a population of around 25 million.[1842] However, this would require some capital investment. New warehouse and storage facilities would be required. So, too, would a shift system if there were to be continuous working in Edinburgh. The Edinburgh plant had been designed to accommodate continuous flow production. This was John Watt’s design. Dr Foster told the Inquiry how he had improved it further.[1843]
This theoretical potential depended in practice on how the factory coped with a 24-hour continuous process. It already operated on a process known as “continuous small volume mixing” (“CSVM”) but it was not until October 1981 that there was a test study to show those designing the BPL plant how CSVM worked in practice. This had not happened before, it seems, because of a shortage of plasma for continuous CSVM, and a lack of agreement as to the terms upon which those working at the plant would be employed. As it happened, instead of examining three shift working (three eight hour shifts),[1844] the trial involved two shifts, each of 12 hours.[1845]
The plant was observed in operation for a week by representatives of BPL. David Wesley[1846] (from BPL) produced a balanced, detailed report on this feasibility exercise. Critically, it concluded that the CSVM system was capable of continuous operation for periods of at least 120 hours.[1847] With the exception of quarantine storage, through to inspection and dispatch, all support sections appeared to have the capacity to handle the product from 1,000 litres of time-expired plasma per day. However:
“Storage space throughout the whole of PFC was at a premium and increased production as achieved during week 2 and 3[1848] will probably place an even greater strain on what is already an overloaded system. The production of Stable Plasma Solution, from plasma storage through to the release of the finished material, relies heavily on each link in the chain functioning correctly. Because of limited in-process storage capacity what may appear at first to be a minor problem, overcome without undue difficulty under normal conditions, may develop because of ‘knock-on effects’ into a much more serious situation when dealing with the products of continuous CSVM operation. The capability of PFC to withstand this type of problem was not challenged during the Feasibility Exercise.”[1849]
A Policy Steering Group meeting followed on 18 December. Mr Hibbert reported on shift working, having attended as an observer during the experiment. Though he did not expect the findings of the exercise to prove conclusively that continuous working would overcome the short-comings of the existing system, the experiment had shown that the equipment could function on such a basis. However, his general impressions were that PFC was capable of improvement: its layout was not ideal, and its output might be increased if the present system were changed. There were doubts that it was more cost effective than BPL. However, he noted that PFC hoped eventually to serve the northern English regions. The group thought it essential to obtain a firm commitment from the SHHD as to the amount of plasma from England which PFC could fractionate.[1850]
There is a telling comparison of the views expressed in 1990 as to what the shift working experiment actually showed. Professor John Cash suggested it provided evidence that Scotland had “very substantial spare capacity” to assist with fractionation of plasma from England and Wales.[1851] He considered that it was a grave error of judgement not to use it.[1852]
Dr Lane, for his part, considered that the results were inconclusive: the trial had been short, and Factor 8 had not been produced by it since the trial involved time-expired plasma which would have no Factor 8 activity.[1853] He thought it unrepresentative of what would occur in practice, and that it was not sustainable for PFC to operate on a 24 hour basis without further investment in facilities, plant and equipment.[1854]
John Harley of the DHSS and Angus MacPherson of the SHHD had however communicated contemporaneously about the results of the trial. It had concluded satisfactorily but (said Angus MacPherson, agreeing in this respect with Dr Lane though without the same dismissive tone) “PFC, Liberton, could process substantial quantities of English plasma only if further ancillary facilities can be provided, and … more land will be needed for the building required.”He gave a figure of around £6-7 million being necessary with an appropriate proportion of the capital cost for the additional facilities to be funded by the DHSS. The necessary building works could be completed in approximately two and a half years, and agreement through the Whitley Council would be needed before staff at PFC could be expected to work in shifts regularly.[1855]
On 1 March 1982, the Policy Steering Group convened once more and agreed that as PFC would not be able to fractionate any substantial quantity of English plasma without the introduction of a three shift working system, plans for the redevelopment of BPL should not proceed on the assumption that it, PFC, would process plasma for England and Wales. Instead, PFC should process plasma for Scotland and Northern Ireland.[1856]
It appears that it was not appreciated that of the £6-7 million identified by Angus MacPherson, a substantial proportion would be needed to rectify the shortcomings which the Medicines Inspectorate had identified in its processes.[1857] Their report on PFC was not at all as critical as it had been in respect of BPL. Nonetheless there were faults which undoubtedly required to be put right, and these would involve the expenditure of considerable funds.
It was the estimate of £6-7 million that put a stop to any further discussions with Scotland.[1858] It may be that a paper prepared in January 1982[1859] is the best source now available for a decision which appears to have been confirmed in September 1982.[1860] It said that “Given that the present BPL has to be redeveloped … it would be more expensive to build a smaller BPL (£18.6 million) and invest £4 million in PFC than to build a BPL capable of achieving self-sufficiency (£21.03 million). In any case, in the view of DHSS officials, it remains highly doubtful whether a shift-working agreement can be negotiated with staff at PFC without serious repercussions on pay of other groups in the NHS and the Industrial Civil Service.”[1861]
In oral evidence to the Penrose Inquiry, Dr Foster later commented that “the decision ultimately was to build the large plant for the whole of England and Wales and not to send plasma to Scotland, and that was justified on some costings that I think, looking at now, could be seen to be quite wrong.”[1862] He amplified this in his written statement to this Inquiry.[1863] If PFC processed plasma to produce Factor 8 for England, then less would be needed to be spent on BPL, since BPL would then process smaller quantities of plasma, and since smaller quantities required less manufacturing space and equipment, it would cost less to build.[1864] He pointed out that Dr Cash’s figure for the additional costs of utilising PFC to process plasma from England for Factor 8 production was £1.2 million[1865] and there would be a saving of more than that sum under the provisional estimates for the building of BPL.[1866]
In summary, after 1977 planning was not conducted on a UK-wide basis. Instead, the two principal production units, at Elstree and Liberton, were each seen as primarily serving the interests of the country in which they were located, rather than the joint interests of both. Plans which had been developed, and funded, in the mid 1960s envisaging two equal units of production were no longer pursued. Dr Lane saw PFC as a rival, bidding for funds that were needed to renew BPL,[1867] rather than as a partner in an enterprise to ensure a UK-wide sufficiency of product. The costs of renewing BPL were considerable. There was no alternative but to incur them, given the contents of the Medical Inspectorate’s report and the policy of achieving self-sufficiency. This in turn led to the Government considering whether the production unit should be run by Beechams rather than by the NHS. It might not have helped the development of a larger unit at BPL[1868] if, at relatively modest expense, the CSVM system operated in Edinburgh could be pressed into service to meet a third or more of the demands for products in England and Wales. Whether or not this was part of the reason for his doing so, he expressed scepticism over the abilities of PFC to produce product in the quantities they said they could. As almost the other side of the coin, it is to be inferred that John Watt was frustrated[1869] that, as a result of delays in reaching agreement as to the supply of fresh frozen plasma from England in sufficient amount to utilise PFC as had been intended, its operation was rendered less efficient than it should have been. John Watt and Dr Cash thus wished to emphasise the advantages they saw PFC as having over BPL, particularly those of the scale of production and the length of time it would take to provide the same levels of production from a new build in England.
A contributory cause to the failure to utilise Scotland was the failure in England and Wales to obtain sufficient fresh plasma before Dr Owen’s initiatives in 1975 to 1977. Since all the available plasma from the north of England was being recruited to production in BPL it left none available for PFC. The way in which the regions were funded to provide for blood products may thus be seen both as a cause of the continued importation of commercial concentrate into the UK[1870] and a contributory cause of the failure to utilise PFC to bridge the gap between supply and demand. In challenging economic conditions the increase of use of commercial product itself led to a lack of incentive to plan immediately for a replacement for BPL, because of the extent of capital commitment that would involve.[1871] The state of BPL was then officially recognised as so poor as to require urgent expenditure: but rather than this being seen as a need which urgently must be met, it in turn led to the Government delaying any long-term plan in order to consider the extent to which pharmaceutical companies might be able to play a part in future factor concentrate provision for the UK. Delays which were described as “unconscionable”and compounded by indecision then simply made the problem worse.
A further, sad, feature of this story is that the focus was largely on making more product available. It was not, as it should have been, making more safer product available.
If self-sufficiency had been achieved, the views generally expressed to the Inquiry, with which I agree, were that a considerable number of cases of AIDS would have been avoided, and, it follows, a significant number of deaths.[1872]
Self-sufficiency was achieved with relative ease in Scotland. The only exception to this was when it came to producing hepatitis-free heat-treated product. BPL got to that goal first – though Scotland was ahead when it came to heat treating all NHS product to be supplied. These themes, and the sad events which remind any reader that self-sufficiency did not by itself provide total protection against the risks of AIDS and other blood-borne diseases, are picked up in greater detail in the next chapter on Viral Inactivation.
Between 1972 and 1998, Northern Ireland was governed by direct rule from Westminster. This included responsibility for blood collection and other health matters.
In 1973, following a major restructuring, health care in Northern Ireland was administered by four health and social boards representing the east, north, west and south, covering a population of approximately 1.5 million. The Northern Ireland Blood Transfusion Centre, which was part of the Northern Ireland Blood Transfusion Service was based in Belfast. Its director from 1968 to 1980 was Colonel T E Field. He was replaced in June 1980 by Dr Morris McClelland.
There was one haemophilia centre. It was based at the Royal Victoria Hospital, Belfast. It was designated a reference centre in September 1981 by the Northern Ireland Office. The director of the Centre between 1978 and 1999 was Dr Elizabeth Mayne. The hospital itself was part of the Eastern Health and Social Services Board.
Northern Ireland was too small to produce factor concentrate itself, though it was able to make cryoprecipitate from local blood donors.[1873]
Accordingly, haemophilia patients in Northern Ireland who were treated with concentrate received NHS products manufactured elsewhere in the UK, or imported commercial products. It received what were described by Dr Mayne as limited quantities of concentrate from Elstree and Oxford.[1874] Because it was too small a population to support a fractionation centre manufacturing concentrate of its own, Northern Ireland was never itself self-sufficient in blood products. Rather, it has to be viewed as part of the greater entity which is the UK.
From 1980, thought began to be given to obtaining factor concentrate from Edinburgh. This reflected the view of Dr Morris McClelland that there were capacity issues at BPL, but apparent spare capacity at PFC.[1875] In December 1980, the health departments serving the four nations of the UK discussed the role that Edinburgh might play in supplying Northern Ireland with blood products. This had impetus because under the pro-rata distribution system introduced from 1 April 1981, Northern Ireland would not be entitled to any factor concentrate: none of the plasma which it collected was sent to BPL.

Following a pattern similar to that in England and Wales, cryoprecipitate usage dropped off after 1976 as factor concentrate use increased. However, the amount of NHS concentrate used in Northern Ireland was minimal compared to the amount of commercial concentrate until around 1984 when for a period of time the use of NHS concentrate began to, and then did, overtake the use of commercial concentrate. The amount of factor concentrates made from voluntary donors is reflected in the chart from 1982/3 onward.
BPL ceased sending its factor concentrates to Northern Ireland with effect from 1 April 1981. PFC did not begin to fractionate plasma until some eighteen months later. There were a number of reasons for this delay. The main one was that the plasma in Northern Ireland was not tested for the presence of Hepatitis B by using an RIA test. Plasma in Scotland was. Accordingly, it would run an unacceptable risk of transmission of Hepatitis B if plasma from Northern Ireland which had been inadequately tested for the presence of hepatitis were to be mixed in the Edinburgh processors with plasma from Scotland which had been more reliably tested. Next, plasma supply from Northern Ireland needed to be increased. Existing refrigeration facilities for plasma were not adequate for freezing the amounts of plasma which would be required to be transported (in a refrigerated truck, and quickly, from Northern Ireland to Edinburgh) and there were some other logistical and administrative difficulties to be overcome. Though the exact date is not clear, it appears that it was in the autumn of 1982 before supplies began from PFC.[1877]
The consequence of Northern Irish plasma being sent to BPL, and Northern Ireland in return receiving Factor 8 concentrate manufactured at Liberton, is that the quantity of NHS factor concentrate used in Northern Ireland increased dramatically.[1878]
Seeking to ensure that the UK did not need to rely on blood products from abroad in order to treat haemophilia was the aim of many of those involved –clinicians who raised the problem early, transfusion directors who arranged for supplies for the UK effort at local expense, fractionators who prided themselves on their professionalism, a minister and some civil servants who were far-sighted, the Haemophilia Society which raised the gap between policy objective and actions – and yet ...
The account in this chapter is haunting as to what might have been. If the DHSS had been more curious about Scottish forward planning in the 1960s, and had echoed it in making provision for England, Wales and Northern Ireland; if they had heeded the full range estimated by the Medical Research Council Working Party in 1974 as well as the increased estimates later coming from the Trends Working Party; if they had in 1976 faced up to the reality that the Medicines Inspectorate were almost certain to condemn BPL as it was, and had grasped the implications of their minister declaring by mid 1978 that BPL and PFL were both working to capacity; if they had briefed Dr Owen in 1974 that what he was being asked to agree – to increase the flow of plasma – would not be enough, so that the Haemophilia Society wouldn’t have had to try to tell him a year later … then matters might (indeed should) have turned out differently.
If, too, the delays in taking a decision to rebuild BPL had not been “unconscionable” – to take the years from 1978 until 1982 to do so, all the while offering commercial products, riskier than should have been supplied to patients in need of treatment, was a disgrace – then much disease might have been avoided.
Each and all of these opportunities were missed. The consequence was that commercial concentrates carrying HIV virus, as well as non-A non-B Hepatitis, were supplied in greater quantities from the US to patients in England, Wales and Northern Ireland[1879] than would otherwise have been the case, not just until 1985 but until the late 1980s so far as Hepatitis C was concerned for, with the exception of Scotland, the UK was still not self-sufficient.
It is not that some in the DHSS did not see the problem and do what they could to draw the attention of others to it but, overall, the DHSS bears a greater part of responsibility for the failures to achieve self-sufficiency than do others. Ministerial indecision contributed to delay in the late 1970s and early 1980s, but (so far as can now be determined given that many of the submissions to ministers have disappeared) ministers may have been inadequately briefed; and the documents that survive suggest that Roland Moyle was not consulted about the decision to abandon the UK-wide approach that had hitherto been adopted. However, they bear some responsibility too for the systems that contributed to what occurred: they include: regional financing, leading to lack of central control over what was a National Blood Transfusion Service in name only; the licensing of commercial concentrates which led to demands for more and more concentrate which were difficult to resist; a lack of central guidance on the importance of giving blood transfusions only when necessary. Those responsible for such systems might wish to reflect that they have the luxury of drawing them up at some leisure in conference rooms and Cabinets, but their consequences are often felt in conditions of urgency and emergency at patient bedside, in wards and hospitals where there is little time to pause and reflect.
What happened was now a long time ago (although its consequences still resonate today on the lives of people who were infected and their families). Some of the voices from those times still ring down the ages, and set the right note on which to end this chapter.
First, Dr Cumming (writing in 1975): “those inadequacies which exist in modern developed countries are entirely the fault of the organisation of the Service … One of the important features of a successful voluntary blood donor system is forward planning.”[1880]
Dr Smith (writing in 2020, about 1975):
“Although national self-sufficiency in blood products was strongly endorsed by the WHO [PRSE0003476], no-one could claim that the principle, and its consequent responsibilities, were embraced as energetically in England as in Scotland … Coming from Edinburgh to Oxford in 1975, I was shocked by this lack of appetite for self-sufficiency at a national level … We were constantly being reminded that it was not DH practice to spend large sums on ‘speculations’.”[1881]
Dr Snape’s final words to the Inquiry sum up what happened. He said he had tried to focus on what BPL/PFL did from 1970 onwards, what was achieved and “what stopped us doing more?” Then his final two paragraphs:
“Now I know that my evidence is the only oral testimony from BPL/PFL. If I had to summarise what we achieved in just a few words, it would be too little, too late.
I know that BPL/PFL staff worked tirelessly, achieved a great deal, but that influences external to BPL/PFL stopped us doing more and doing it sooner. And for that I’m profoundly sorry.”[1882]
Lord Owen (giving oral evidence):
“We all wanted, for everything. You have to choose, and of course it is difficult. But we did it … The Department made their observations, I made the decision, they loyally followed it, they chased, they guarded, they put it in things, and that limited amount of money achieved a substantial way towards self-sufficiency. It didn’t achieve it but, against a rising trend of demand, it overachieved what we expected. So I don’t think there is any reason for anybody who was involved in the Department during that period to hang their head in shame about this at all.”[1883]
Many reading this chapter will think that, contrary to his views, he was less well served than he should have been, since from such documents as remain available it appears he was not informed of the MRC Working Party estimate based on Dr Biggs’ paper by his civil servants,[1884] nor made aware of the creaking nature of the production facilities even if a sufficient supply of plasma might be achieved. Had he been, at a time early in his (short) period of office, the outcome might have been different.
This chapter looks at whether heat-treated products could and should have come earlier in the UK. It also considers the extent to which heat-treated products were used, once available, and examines the events which led to the withdrawal of Armour’s heat-treated product in October 1986.
1945 Discovery that heat will inactivate hepatitis virus (in albumin).
1972 Cutter conducts experiments with heat treatment which show Factor 9 activity could be preserved.
April 1974 research underway at PFC to find a way of physically removing Hepatitis B.
June 1977 Dr Harvey Alter calls for viral inactivation. Calls by others too.
1977 Cutter creates task force to try to solve “the hepatitis problem”.
1978 Behringwerke conducts experiments in heat treatment and begins clinical trials.
1978/1979 Cutter and Hyland experiment with dry heat approach, followed by Armour.
October 1980 Behringwerke presents its heat-treated process at Bonn Conference.
September 1981 PFC starts performing experiments on pasteurisation.
1982 Alpha assesses it has the “nucleus of a process that needs about three or four months’ work”, applies for FDA licence for heat-treated product in January 1983.
Early 1983 BPL starts development work on a heat-treated ‘Hepatitis-Safe’ Factor 8 product.
March 1983 FDA licenses Hyland’s dry heat-treated product.
January 1984 FDA licenses Armour’s heat-treated product, followed by Alpha’s and Cutter’s products in February 1984.
Mid 1984 Haemophilia centres at Sheffield, St Thomas’, Middlesex and Margate start to use heat-treated concentrates.
July 1984 BPL starts intensive development of what will become 8Y.
November 1984 Reported at symposium in Groningen that heat treatment at 68°C for 24 hours inactivates HIV; PFC is heating its Factor 8 stocks; CBLA announces plans to heat all BPL Factor 8 by April 1985.
10 December 1984 PFC issues heat-treated Factor 8 for routine use; meeting at Elstree of reference centre directors and others to devise treatment recommendations.
February 1985 commercial heat-treated concentrates are licensed in UK; BPL releases first batches of 8Y for clinical trial.
2 May 1985 all Factor 8 issued by BPL heat-treated by this date; only 8Y issued after September 1985.
October 1985 BPL and PFL heat-treated F9 becomes routinely available.
October 1986 Armour withdraws heat-treated Factorate following seroconversions.
April 1987 PFC issues Z8, the equivalent of 8Y free from hepatitis as well as HIV.
Dr Peter Foster head, Research & Development Department, PFC
Dr Richard Lane director, BPL
Dr James Smith scientist in charge of fractionation at PFL in Oxford (1975 - 1992) and also head of coagulation factor production at BPL in Elstree (1979 - 1982)
BPL Blood Products Laboratory (Elstree)
PFC Protein Fractionation Centre (Edinburgh)
PFL Plasma Fractionation Laboratory (Oxford)
Though the virus causing Hepatitis B was identifiable before 1970, following the discovery of the Australia antigen in 1965, identification of what is now known as Hepatitis C proved intractable. There is nothing to suggest that the principal cause of non-A non-B Hepatitis (“NANBH”) (as Hepatitis C had been called) could and should have been identified sooner than it was (in 1988, by the Chiron Corporation[1885]). It therefore could not be eliminated by testing donations and excluding those which carried specific markers for the virus,[1886] because these were unknown. Before 1970, however, it was widely known (a) that hepatitis transmitted by blood or blood products was caused by a virus, and (b) that that virus (or those viruses[1887]) might be inactivated by one of a number of means. Principal among those means was the possibility that heat might inactivate the virus (just as it is commonly appreciated that boiling water will kill most biological contaminants within it, so lesser heat may inactivate some viruses completely, and in any event may reduce viral activity). Because some viruses were known to be enveloped – that is, to have a fatty (“lipid”) coating – another possibility was that solvent detergents could be used to destroy the coating and render such a virus inactive. It was known, too, that some possibilities could be discounted: in 1950 attempts to inactivate serum hepatitis by irradiation with UV light had failed.
The possibility that hepatitis viruses in blood products could be inactivated by heat was seriously considered. Albumin, a blood product, had been successfully heat treated since the late 1940s to eliminate the risk of hepatitis arising post-injection.[1888] This arose after a chance observation[1889] led ultimately to the discovery of chemicals which preserved the integrity of the albumin protein when subjected to heat (“stabilisers”). As a result, it proved possible to pasteurise albumin: applying heat through water in which a vial of albumin and the stabilisers were present. Pasteurisation in this way was introduced in the US from June 1945, and proved effective to inactivate serum hepatitis.[1890] Clinical trials of pasteurised albumin started in London by 1952.[1891]
As early as 1952, a World Health Organization (“WHO”) Expert Committee report on the prevention of serum hepatitis had “Sterilization of blood-plasma” as one of five measures which might be taken to prevent its spread.[1892] This was plasma – not whole blood containing red blood cells too. So far as heat treatment is concerned, whole blood for transfusion is not, and has never been, heat treated, because to do so damages its constituent parts. Heat can, however, be applied to plasma or blood products. Applied to them in their “wet” form this is akin to pasteurisation. It may alternatively be applied to the freeze-dried product (a process known as “dry” heating).[1893]
It was recognised by 1970 that the biggest single problem in administering factor concentrates to people with haemophilia was the accompanying risk of conveying serum hepatitis. Though this did not then lead to any determined efforts to eliminate or reduce the risk, adverse publicity had already been created for the pharmaceutical companies. Professor Garrott Allen, repeatedly, wrote as did others about the risk carried by blood which was sold, rather than donated.[1894] Whether this was the reason, whether it was a desire to enhance the safety of its products, or whether for some other reason,[1895] in 1972 Cutter (manufacturer of Konyne and Koate products, to treat Factor 9 and Factor 8 deficiencies respectively) conducted some experiments with heat treatment to see if it might inactivate hepatitis in Factor 9. It had been thought before then that if heat treatment were applied to Factor 9 at temperatures and for times which would inactivate the hepatitis virus it would so affect the molecular structure of the Factor 9 protein that little or no coagulation activity would remain. In short, the “yield” of Factor 9 from a given volume of plasma would be minimal and make the process uneconomic.
What happened in those experiments was something of a revelation. As reported in Cutter’s Biochemical Research Department Quarterly Progress Report for April-June 1972, experiments were conducted by Cutter to see if the virus with which Factor 9 was spiked could be inactivated whilst the Factor 9 was kept active. Its activity was indeed maintained when heat was applied to concentrate in dry form in the presence of “salts”. The text reveals that very little clotting activity was lost – although the viruses (which, importantly, did not include hepatitis virus) remained active.[1896] This was of particular interest because it showed that heat did not of itself “de-nature” Factor 9 and it might therefore have been thought that the same could apply to Factor 8, assuming in both cases that appropriate “salts” were present. Of such importance was the result of the test that when Hyland, Alpha and Armour beat Cutter[1897] in the race to license their heat-treated products during the AIDS crisis, an internal Cutter memo noted these experiments as being a reason to avoid patent restrictions.[1898]
Dr Shohachi Wada was the person who conducted these experiments. He did so as directed by senior managers.[1899] Their purpose was to determine if Factor 9 could be stabilised to withstand 60°C wet heat.[1900] He described in a deposition in American litigation how he was aware that the plasma used to make Factor 9 at Cutter carried a risk of transmitting hepatitis, of patients getting it and dying.[1901] He described how four different stabilisers were tested,[1902] and how he experimented on Konyne using 60°C dry heat, with and without salts. None worked to inactivate the two viruses used,[1903] but Factor 9 activity was almost entirely preserved in the presence of salts.[1904] He would have tried with different concentrations and different pHs, “If I had time” he said.[1905] He knew that different proteins needed different stabilisers; that sucrose (which he did not use) was a general protein stabiliser; and that although in his experiments he used 50% glycerol, 75% was described as the optimal solution.[1906] In short, he showed that activity could be preserved in heating; and he would have gone further and conducted further tests if he had been asked to do so. Though his research could have benefited from more time, as he said, he was allowed none.
Throughout the 1970s a number of other attempts were made to inactivate hepatitis. Not all involved heat. Although the use of solvent detergent was not widely explored before 1970, suggestions were made during the 1970s that it might be of some effect. Dr Edward Shanbrom, who worked as a vice-president of Medical and Scientific Affairs Hyland from the late 1960s until 1972 and there developed the first commercially marketed freeze-dried Factor 8 concentrate,[1907] became convinced it might work, and eventually patented a process, but his suggestions attracted only minimal support in the 1970s and very early 1980s.
Dr Shanbrom noticed that a form of hepatitis became airborne in plasma mists around the processing plant, which was dangerous because it was concentrated in the pools of plasma from which concentrates were made, and he expressed his concerns about this and the attendant dangers in writing. He said that he had suggested to the executives that they should no longer take plasma from hepatitis hotspots such as downtown Los Angeles and from prisons because of the risks. He was removed from his role at Hyland, and worked both at home and for Merck where he developed the idea of using detergent to inactivate viruses in clotting factor concentrates;[1908] he hawked his idea around the major manufacturers, but they showed no interest:
“According to Dr Shanbrom, he tried to persuade the four major manufacturers of clotting-factor concentrates to use a detergent process for viral inactivation as early as the mid- to late 1970s. Though some of the companies demonstrated interest in the process, there were no takers because, as Dr. Shanbrom recalls, ‘They said, ‘We don’t have a problem.’’ … he approached what was then the Hepatitis Division of the Centers for Disease Control, hoping to interest them in using and studying his detergent process of viral inactivation. The response was a letter from the CDC that he has saved to this day. The CDC expressed interest in Dr. Shanbrom’s process but regretted that it did not have enough chimpanzees to enable researchers to conduct experiments with it. For want of adequate funding to the CDC for chimpanzees, clotting factor remained infectious.”[1909]
Dr Shanbrom patented the process in 1980, and eventually it was taken up by the New York Blood Center in 1988.[1910] Solvent-detergent inactivation became the most prevalent method of viral inactivation after that, to the extent of replacing much of what had previously been heat-treated products.
Sporadic efforts such as those of Dr Wada (as directed by the Cutter management) and Dr Shanbrom (self-directed) did not become sustained efforts of the pharmaceutical industry as a whole till later in the decade: as Dr Shanbrom’s experience suggested, companies were not particularly interested.
Meanwhile, in the UK, there is no evidence that research into viral inactivation or removal occurred at the Blood Products Laboratory (“BPL”) or the Plasma Fractionation Laboratory (“PFL”) (Oxford) in the early to mid 1970s. At that stage, the Lister Institute, a research institute[1911] supported largely by private donations, managed the plasma fractionation centre at Elstree. It struggled financially in the 1970s (selling up valuable premises in Chelsea and eventually relinquishing its Elstree site in 1978), which may help to explain the limited nature of any research effort which it would have been possible for Lister to conduct.
By contrast to the position south of the border, when Dr Peter Foster was appointed as Head of the R&D Department at the Protein Fractionation Centre (“PFC”) in April 1974 he said he found that research was underway there to find a means of physically removing Hepatitis B virus from factor products.[1912]
Whilst the desirability of removal of hepatitis virus was clear, there was no research as yet in the UK on applying physical techniques such as heat, or chemical techniques such as the use of solvent/detergents to inactivate the virus, as opposed to seeking its physical removal.[1913]
By the mid 1970s, concerns were increasingly expressed, by clinicians and bodies whose central interest was the safe treatment of bleeding disorders, about the need to remove or reduce hepatitis viruses from blood products used to treat them. It was part of the reason for the Haemophilia Society, clinicians, politicians and administrators in the UK seeking self-sufficiency in the supply of blood products. But the concerns were strongly felt internationally, and by many in the US in particular. In March 1976 a conference sponsored by the Food and Drug Administration, the National Institutes of Health and the National Hemophilia Federation and called Unsolved Therapeutic Problems in Hemophilia noted that “Research in a number of laboratories has been directed towards developing means of removing HBV from final products while maintaining the labile clotting factors.”[1914]It recorded interest, and implicitly recognised a need: but it did not record progress.
Then, in June 1977 Dr Harvey Alter[1915] called for viral inactivation: “The major thrust of posttransfusion hepatitis research must now be directed at developing detection methods for the non-A, non-B agent(s) or developing some reliable method of viral inactivation or removal which would be independent of testing.”[1916] In the same month the World Federation of Hemophilia also “called on the makers of clotting concentrates to kill viruses in their products for the sake of future generations of persons with hemophilia”.[1917] Dr Joel Spero, who gave a presentation to the World Federation (subsequently published) at its annual meeting, said that “a major effort is necessary to develop a ‘clean’ product rapidly for the treatment of the next generation of hemophilic patients.”[1918] There is evidence that Baxter approved a study, again in the same month, of the feasibility of removing hepatitis from Hemofil.[1919]
These calls for greater efforts coincided with the commercial market seeming to pharmaceutical producers to have become stagnant, as Hyland were to observe: “It is clear that with the number of competitors now on the market … and the stagnant AHF consumption, a product innovation would be very timely to maintain our current price level and increase our market share.”[1920] The Baxter project begun in June 1977 aimed to “result in dramatic increases in unit sales and average selling price.”[1921]
This view may explain the fact that at about the same time as the calls for focused research became stronger and pressing (in the latter half of the 1970s) a number of commercial fractionators began to experiment to see if the hepatitis virus could be inactivated by heat, either applied dry to freeze-dried concentrate or by pasteurisation. Thus at the same time as the World Federation of Hemophilia called for a clean product, Hyland began to study the feasibility of removing hepatitis from Hemofil,[1922] and Behringwerke (in West Germany) conducted initial experiments in heat treatment.[1923] Again in 1977, the work which Cutter had been doing on stabilisers and heat after 1972 began to bear fruit and it created a task force to try to improve Koate and Konyne, and partly to try to solve “the hepatitis problem”.[1924]
Thus, by 1978 three companies (Behringwerke, Hyland, and Cutter) were more actively engaged than they had been previously in what was seen as promising research into heat treating factor products so as to inactivate viruses.
In outline, since it was already known that heat would destroy hepatitis viruses, there was in addition a need for appropriate chemicals to be found to ensure that the application of sufficient heat did not destroy the activity of the proteins of interest (here Factor 8 or Factor 9), which were known to be particularly vulnerable to heat. The chemicals needed were to “stabilise”the protein of interest (ie protect it against heat) so that it remained substantially in a form in which it could be used. Pharmaceutical companies would of course need to identify a stabiliser which would work with the particular method of manufacturing adopted by the company concerned. They also needed to refine their particular method of production so that nothing would compromise the effectiveness of heat treatment.
The research was not without individual stories of good fortune. Dr Peter Fernandes, a biochemical engineer at Cutter, discovered an appropriate stabiliser by accident. He forgot one evening to turn off the heating to a water bath in which he had left modified immune serum globulin together with a carbohydrate stabiliser. He suspected that when he came back in the morning it would have become a thick gel or solidified mass. However, when he looked at the water bath he discovered that the globulin had not been as badly affected by the heat as he had expected. It must have been the stabiliser which had had that effect. Realising this, he quickly moved on to show in December 1978 that similar stabilisers to those which worked with the globulin could work with antihemophilic factor (“AHF”).[1925]
There is no evidence that other pharmaceutical companies were aware of Dr Fernandes’ fortunate discovery by error. Nor that any similar piece of luck enlightened them. Yet they also discovered appropriate means of preventing heat from irreversibly damaging the coagulation activity in their concentrates. Each company had a product which had been prepared by a slightly different process. Inactivating viruses in each was a case of independent applied research, not a case of “one size fits all”. Dr Milton Mozen, the director of Biochemical Research and Development at Cutter, emphasised this in his evidence to the Institute of Medicine in the US, and also to the Krever Inquiry in Canada, saying: “As manufacturers of coagulation products use different purification procedures, the impurities present in one manufacturer’s product will not be the same as those in another manufacturer’s. That a heat treatment process is successful as applied by one manufacturer, it does not follow that this process would be applicable to the unique products of the other manufacturer.”[1926] Inevitably, the process of identifying a stabiliser that would work to protect the coagulation activity of Factor 8 or Factor 9 in a particular product was a matter of persistence until reward.
Although pharmaceutical firms, like many manufacturers, were careful to preserve commercial secrecy[1927] (and Dr Foster’s evidence suggested that to this day it is not known precisely how the pharmaceutical companies preserved the stability of the coagulation factor in their products[1928]) it became more difficult once clinical trials began to keep secret the fact that they had done so. Thus Behringwerke began clinical trials in 1978 in Germany of what was known at first as “Factor VIII Behringwerke”.[1929] Hyland learnt of this in February 1979, in a report to their head office later confirmed by another Hyland employee.[1930] Knowing that a rival had reached the stage of conducting clinical trials gave further impetus to their work. Having then heard that the clinical trials of the Behringwerke product were almost complete, and had promising results,[1931] Hyland decided to pursue Hemofil-HT[1932] as a major project.[1933]
Whereas Behringwerke used a “wet heat” approach, akin to pasteurisation, Cutter[1934] and Hyland both used dry heat, applying the heat to a product which had already been freeze-dried. So did Armour (which, in 1979,[1935] followed them in beginning work on a dry heated product).
By 1980 the research and development department of Cutter had made a strategic commitment that all new plasma products would be pasteurised, although it acknowledged that its studies were continuing to find ways in which their Konyne product might be rendered non-infective.[1936]
By October 1980, there was no need any longer for pharmaceutical companies to rely upon such intelligence as their agents could discover about the German product. Behringwerke presented its process to the medical public at the International Haemophilia Conference in Bonn, and claimed it had successfully inactivated hepatitis virus by applying wet heat.[1937] Dr (later Professor) John Cash was present at the conference.[1938] When he returned to Scotland, he told Dr Foster (PFC) of the presentation. Dr Foster was “shocked”. He had thought it “inconceivable” (until then) that heat could be used to inactivate a virus in Factor 8 or Factor 9, because his understanding had been that those proteins were so vulnerable to heat that their coagulation activity could not be preserved.[1939] Yet within about three years, despite the limited resources available to him, PFC too had developed a method of heat treating factor concentrate so as to inactivate viruses within it – by then, importantly, and particularly, the virus responsible for AIDS.
Behringwerke’s presentation was written up under the heading “Factor VIII concentrate – now free from hepatitis risk: progress in the treatment of haemophilia”.[1940] Behringwerke had potential rivals in Germany: it was a big market for the pharmaceutical companies. Hyland decided to proceed with heat treating its product on the basis not that it would eliminate hepatitis, but reduce the risk of it,[1941] and aimed to market it in Germany, providing competition for Behringwerke.
Behringwerke’s product entered production, though there was a cost penalty to be paid since the process resulted in a significantly reduced Factor 8 activity in each unit, and treatment with it was more expensive as a result.
By the early 1980s, other major pharmaceutical companies had begun to prepare both wet and dry heated factor concentrates for active marketing. They each adopted slightly different processes, as the table below shows.
| Manufacturer | Method[1942] | FDA[1943] licence | UK licence | Product |
|---|---|---|---|---|
| Hyland (Baxter) | Dry heat 60°C 72-74 hrs | March 1983 | February 1985 | Hemofil-T |
| Armour | Dry heat 60°C 30 hrs | January 1984 | February 1985 | Factorate HT |
| Alpha | Heated in solution 60°C 20 hrs | February 1984 | February 1985 | Profilate HT |
| Cutter (Miles) | Dry heat 68°C 72 hrs | February 1984 | February 1985 | Koate HT |
Alpha was later than Hyland, Cutter, and Armour to begin work in the US on viral inactivation by heat. Alpha became aware of the Behringwerke patent in January/February 1982.[1944] By that stage it was already doing research upon purifying its product (“purification” in this context means removing superfluous proteins from the product: in particular, reducing the amount of fibrinogen or fibronectin present in the source material from which the Factor 8 product comes). Work on this higher purity product was well advanced. Alpha thought that developing a process of heat treatment to inactivate hepatitis would be assisted by starting with a product of higher purity. It considered it already had the “nucleus of a process that needs about three or four months’ work.”[1945]The prediction was right: it took only some four months before an application to the Food and Drug Administration (“FDA”) for a licence for their heat-treated product was made, in January 1983,[1946] and it was licensed in the US in February 1984.[1947]
Importantly, for the conclusions which are to be drawn from the whole of the facts, Alpha chose not to replicate the Behringwerke process: “The decision was made to take the process that was almost in the finishing of development at Alpha and see how that stood up to adding sugars to it and to adding various other things that Behring pointed out because we had a whole process in place, and we felt we could probably move ahead in our research and development just as fast with our new process as trying to repeat this Behring process.”[1948]
What, then, was the impact of these international developments on UK production? The account begins in the early 1980s. PFC in Scotland was proactive. It began working on a method of heat treating factor concentrates almost as soon as Dr Foster became aware of the claims that Behringwerke had made in Bonn in October 1980. Experiments on pasteurisation of Factor 8 were performed from September 1981,[1949] in January 1982 a “Factor VIII Study Group” was formed by Dr Cash to coordinate further developments,[1950] and by February 1982 preliminary results were reported on the pasteurisation studies.[1951] By contrast, work in England did not start in earnest until 1983, and remained at a “very preliminary” phase until May 1983.[1952]
Dr Richard Lane, director of BPL, recorded that no work was done by BPL during 1981 to research heat treatment.[1953] 1981 did not, however, pass without there being at least some discussion about the possibility of beginning a research project. Thus on 27 February 1981 Dr James Smith proposed to Dr Lane some first outline proposals for programmes to research tackling the transmission of viruses by coagulation factor concentrates. He wrote: “The significance of a product demonstrably free of hepatitis risk cannot be ignored and it is essential that BPL/PFL be well placed to take advantage of such developments.”[1954] This proposal, according to Dr Lane, marked “the start of a move towards a viral inactivation programme.”[1955] Dr Lane reported to the Scientific and Technical Committee of the Central Blood Laboratories Authority (“CBLA”) during the next month that “a research project into the development of coagulation factor concentrates with reduced risk of hepatitis transmission, was an appropriate case for central funding.”[1956] A paper was produced by the Research and Development department of BPL, which considered a report that year that another protein important in the clotting process, antithrombin, had been stabilised with sodium citrate and withstood heating for at least ten hours at 60°C. It noted that heating albumin products for such a period in the presence of a stabiliser had a “good record in the elimination of hepatitis virus infectivity” and that “If similar stabilisers can be established for coagulation factor products then heat inactivation will become the treatment of choice.”[1957] Yet no work was actually done at BPL during 1981 to research ways of heat treating factor concentrates, let alone develop any pilot product. There were, rather, discussions about whether to research the possibility, a slow process to glean information about the degree of success commercial firms had in reducing hepatitis transmission, and answers being sought to questions about the safety and efficacy of those heat-treated concentrates which were being developed elsewhere.[1958] Throughout, according to Dr Lane, a “requirement for central funding for research and development was a continuous theme in 1981.”[1959] He records that he proposed to the CBLA Scientific and Technical Committee in the spring of 1981 that a research project into the development of coagulation factor concentrates with reduced risk of hepatitis transmission was an appropriate project for central funding.[1960] The minutes and such documents as are available do not provide clarity as to what became of this proposal, but any practical consequence of it was slow in emerging.
BPL’s work on heat treatment only really started in 1982. That was in relation to Factor 9, not Factor 8.[1961]
From mid 1982 onwards the risk that people with haemophilia treated with blood products might suffer AIDS (in addition to the risks they had of contracting hepatitis) became progressively clearer.
Some encouragement for the potential of heat treatment in Factor 8 came in the journal Transfusion in late 1982.[1962] Dr Robert Gerety and Dr David Aronson in an invited review recognised the potential of heat treatment to remove both Hepatitis B and non-A non-B Hepatitis infectivity.[1963] They focused on hepatitis, not on the suspected viral cause of AIDS.
At the end of 1982, Dr Diana Walford wrote a minute flagging that Travenol (Hyland) were planning a symposium in early 1983 to launch a reduced hepatitis risk product. Stanley Godfrey, to whom it had been copied within the Department of Health and Social Security (“DHSS”), responded with a handwritten note worrying whether doctors might insist on using such a “hepatitis free” product at great cost, and would “turn away from the BPL product”, and also expressing concern that if BPL were to obtain the technology on licence such would the reduction be in yield that “Goodness knows what size factory we’d need!”[1964]
Whether prompted by rivalry with commercial producers, or not, it was only at the start of 1983 that BPL began working on heat-treated Factor 8.[1965] In February 1983, Dr Smith visited PFC in Scotland to discuss research and development in respect of coagulation factors, and put forward to Dr Lane a “Proposal to Develop a ‘Hepatitis-Safe’ Factor VIII Concentrate”.[1966]
In March that year Hyland, well ahead of BPL at this stage as this chronology shows, was licensed by the FDA in the US to market dry-heated concentrate. It had a head start of some nine months over its pharmaceutical rivals. Hyland’s success in gaining a licence was followed in January 1984 by the grant of FDA licences for Armour’s product[1967] and Cutter’s pasteurised product[1968] and in February 1984 for a product from Alpha[1969] and for Cutter’s dry-heated product.[1970]
By this time Dr Smith proposed to make a special preparation of Factor 8 which would be subjected to dry heat (8CRV).[1971] His proposal noted at the outset that during 1982 and 1983 several companies had sought support for the clinical trial of “hepatitis-safer”concentrates of Factor 8. He said that PFL/BPL had elected to try dry heating of an existing product, 8CRV. In the proposal he recognised “our late start”[1972] in inactivation studies which “might leave us without a product to offer for a year or more, by which time many of the small group of suitable patients would have been committed to testing other products.”In short, he was concerned that the few blood product recipients who had not already been infected with hepatitis might be engaged in testing other products (ie commercial ones) to establish, for licensing authorities considering the grant of licences in respect of those products, whether they did, indeed, reduce non-A non-B Hepatitis as claimed. Since he noted that interim results showed that dry-heated Hemofil Factor 8 caused “at least some attenuation of NANBH” and also that limitation on pool size also reduced the risks, both of being infected and of the infection being severe, he thought that the first trial of heat-treated product from BPL should focus on evaluating a product made by combining both a “small pool” approach and heat treatment.[1973] It was first used from March 1984.[1974]
At the end of February 1984, the CBLA agreed to finance this trial of 8CRV.[1975]
In July 1984 BPL started intensive development of what was to become 8Y[1976] and then actively planned to apply dry heat treatment to all the Factor 8 produced at BPL because by the autumn it was shown that heat treatment appeared to inactivate the HTLV-3 virus which by then had been identified as the cause of AIDS.[1977]
The purpose of introducing heat treatment was to eliminate or reduce the scourge of hepatitis. However, it was recognised that heat might destroy other viruses, too.[1978] When it was realised, progressively after early to mid 1982, that AIDS might have a viral cause, which might be transmissible through blood products, it was therefore speculated that heat treatment might reduce or eliminate that too. Dr (later Professor) Eric Preston, Professor Geoffrey Savidge, Dr (later Professor) Samuel Machin and Dr Mark Winter had started to use heat-treated concentrates for their patients by mid 1984 in this hope. Others were more sceptical, and concerned both that there was no clear evidence that the treatment did indeed have this effect, and that to use these concentrates risked the heat having altered the clotting factor proteins in a way which caused immune reactions, even to the extent that they might not then be able to be treated at all.[1979] However, this fear should be seen in context: by now the products of the main commercial companies had been licensed in the US for up to a year or more without any such adverse reactions being reported.
In September 1984 The Lancet published an article which in its summary said that the findings reported in it “support the possible role of retroviruses in AIDS, and indicate that factor VIII concentrates must be heated to inactivate these infectious viruses.”[1980]
The next month the Morbidity and Mortality Weekly Report (“MMWR”) announced that heating Factor 8 concentrate could inactivate HTLV-3 and reported the recommendations of the Medical and Scientific Advisory Council of the National Hemophilia Federation that strong consideration should be given to the prescription of heat-treated products for all except for Haemophilia A patients under the age of four or new patients (who should have cryoprecipitate), Haemophilia B patients in the same categories (who should have fresh frozen plasma) and mild to moderate patients who should be treated with Desmopressin (“DDAVP”) whenever possible, adding: “the use of nonheat-treated factor concentrates should be limited.”[1981]
The Centers for Disease Control and Prevention (“CDC”), whose publication the MMWR was, went on a week after that to present its results to the annual symposium about blood transfusion held at Groningen. It was reported there that heating at 68°C for 24 hours inactivated HIV.[1982] Internationally, there was a move to abandon the use of factor concentrate products which had not been heat treated.[1983]
In the interim, Dr Lane had written to Dr Edmund Harris at the DHSS to notify him of his plan to dry heat all the Factor 8 to be produced “on the empirical basis that it has a satisfactory process efficacy for inactivation of HTLV-III.”[1984] Dr Harris did not agree immediately. Instead he responded by asking Dr Lane to refer his plan to an advisory group to consider if the evidence for inactivation of HTLV-3 by heat was “sufficient to warrant” taking such a step, “particularly if a screening test can be made available.” He wanted both the DHSS and the CBLA to be furnished with full details of the proposal.[1985]
Dr Lane’s view was that “the risks of transmission of HIV were such that heat treatment should be employed even if it turned out to be a temporary expedient.” He knew from BPL’s research at the time that “heat treatment was feasible and, in the longer term, the development of a superior product (8Y) carrying less penalty in terms of loss of yield due to heating and greater possibilities of virus inactivation … was beginning to look a firm possibility.”[1986] The day after Dr Harris’ stalling letter,[1987] Dr Lane reported promising trials of a heat-treated product to the CBLA Central Committee for Research and Development in Blood Transfusion and that the time scale for the new product he had in mind (“8Y”) was a year. The meeting agreed to recommend to the CBLA that BPL should start dry heating material which was already being produced, whilst continuing to examine methods to obtain a better yield, and also that trials should consider whether the dry-heated products inactivated HTLV-3 as well as hepatitis.[1988]
Dr Lane did not wait for the meeting to which Dr Harris had referred the issue. Although on 13 November 1984 his team gave him a “very provisional” date of 1 April 1985 for the implementation of heat treatment, and said it was “impossible to judge its feasibility”,[1989] by 19 November the CBLA was announcing that they planned to heat all Factor 8 manufactured at BPL/PFL from April 1985.[1990] This may have been prompted not just by Dr Lane but by reports in the popular press that a “second haemophiliac death has occurred in Britain from aids”[1991] – the CBLA announcement came a day later – and that three babies had died of AIDS in Queensland in Australia (reported during the week before), and yet further impetus was given to the need to shift to heat-treated products by Professor Arthur Bloom, who wrote to the DHSS to urge that heat-treated products be licensed so as to be freely available.[1992]
It was not however until 27 November that the Working Group on AIDS to the National Blood Transfusion Service (“NBTS”) Advisory Committee (the group to which Dr Harris had referred the question of heat treatment) met. Scotland was already ahead of England and had started to heat Factor 8 stocks in a way which would inactivate HTLV-3.[1993]
The 27 November meeting was controversial in that the record described it as having gone “reasonable [sic] well”; whereas other reports expressed a significantly different viewpoint.[1994] So far as heat treatment of blood products is concerned, however, the report to Dr Harris said: “although there is not yet the evidence to guarantee that this is satisfactory; the view was nevertheless unanimous that it should be done. This should be in addition to using a screening test when available. In the present state of knowledge bolt [sic] and braces vital. Some expressed the view that we should stop the import of Factor VIII not heat treated.”[1995]
Two days later, Professor Bloom was assured by the DHSS that prompting “the appropriate manufacturers” to apply for abridged product licences to ensure the supply of heat-treated product was a “high priority item”.[1996]
Scotland stayed ahead of England.[1997] From 10 December 1984 it was issuing heat-treated Factor 8 for routine use.[1998]
It took longer for this to happen at BPL.[1999] Dr Lane had arranged a meeting of the United Kingdom Haemophilia Centre Directors’ Organisation (“UKHCDO”) reference centre directors at BPL for the same date.
In advance of it, Dr Smith wrote to Dr Lane observing that:
“Now that CBLA have publicly stated that BPL issues from April will be heated, we will be seen as dragging our feet if the meeting on 10th December does not endorse some sensible immediate action. US companies say they can provide UK with more than enough heated product, today. This is our last opportunity to get anything resembling rational trial without exposing patients to greater risks. I think the HCDs are in a mood to co-operate, but NHS sources may have the intuitive edge over imported products only until the next scandal hits the papers.”
He added, in respect of Oxford, that “Anything going into PFL’s oven on 11th December will not be issuable until January”, and asked if there should be an interim policy on the issue of “what little dry-heated 8CRV we already stock?”[2000]
When the meeting took place, Dr Lane said that current work at BPL was directed to making available limited supplies of a heat-treated product until April 1985, and that “HT material in large quantities could not be available before April as equipment had to be ordered.” In the circumstances he would not however issue unheated product unless it was required for use and a specific request for it was made.[2001]
Despite the calls there had been at the 27 November meeting for heat-treated product to be used instead of unheated product, to the extent that further unheated commercial product should be refused entry into the UK, and the views being expressed by UKHCDO directors in their 10 December meeting at BPL, at the end of 1984 there was still little heat-treated product freely available in England. Such as there was in England either came from Scotland, which was rare, or was used on a “named patient basis”.[2002]
To conclude the events of 1984, in December The Lancet in an editorial said that the time had come when it was now reasonable to switch to heat-treated products.[2003] From the middle of December a 12 month stock of Scottish product[2004] had already been heated at 68°C for two hours and clinical trials had shown no adverse effects. Factor 8 activity had been preserved. Later, from 20 January 1985, the stock was heated for 24 hours.[2005]
By the start of 1985 the position was this.
Scotland was self-sufficient in a supply of heat-treated product. It had been tested, in Edinburgh, successfully, such that on the 6 December 1984 Dr Robert Perry, the acting director of the PFC, was able to write to the five Scottish regions and Belfast to tell them that they would be supplied on 10 or 11 December with sufficient heat-treated product to cover a month, and that a continuous supply would be made thereafter in sufficient quantities to enable non-heat-treated product to be recalled.[2006] In Scotland, therefore, only heat-treated product capable of eliminating HTLV-3/HIV was issued from 10 December 1984. It was later trumpeted as being the first country in the world to be self-sufficient in Factor 8 concentrate heated so as to eliminate a risk of AIDS. It deserved that accolade. But this product did not prevent the transmission of hepatitis. For that, Scotland had to wait over another two years.
Cutter’s product, Koate HT, had been available since November 1984.[2007] So too were the products made by Armour, Travenol/Hyland, Alpha and Hoechst.[2008] However, though some were supplied on a “named patient” basis, the licensing of commercial concentrates had to wait until February 1985. It was then, but not before, that the heat-treated products of Baxter, Alpha, Armour, Cutter and Immuno were all licensed,[2009] after which they were more freely available.
BPL had not yet (it appears) caught up with its “late start”.[2010] At a Haemophilia Society Executive Committee meeting in January 1985 it was reported that “the introduction of heat-treated materials has been ‘patchy’ and that at least one Supra-Region had not yet introduced heat-treated materials.”[2011]Part of the reason was a shortage of domestic supply. There had as yet been no clinical trial of 8Y. The first batches were released from BPL for a clinical trial of safety and efficacy in February 1985.[2012] Heat treatment was being applied to BPL’s existing product, HL, but both because self-sufficiency had not been achieved, and because the yield of clotting activity per litre of plasma was reduced a little by the treatment, there was less to go round even than there had been in 1984.
In a written answer to a parliamentary question Kenneth Clarke, the Minister of State for Health, said that BPL manufactured almost half the NHS consumption of Factor 8.[2013] It had started to heat treat its Factor 8 and that “limited amounts will be distributed to the National Health Service for clinical trials within the next two weeks. Heat-treatment capacity is being increased, and it is hoped that, by April this year, all BPL factor VIII will be heat-treated.”[2014] By contrast, (though his statement did not acknowledge this) commercially produced heat-treated products were now circulating freely.
It is plain that not all home produced Factor 8 was yet heat-treated, for in April Haemofact 6 reported that Lord Simon Glenarthur, Parliamentary Under-Secretary of State for Health, speaking in the House of Lords, had made it clear that all home produced Factor 8 would be heat-treated “from April 1985”.[2015] It was not until 2 May 1985 that all Factor 8 concentrate issued by BPL had been heat treated under at least “HT2 conditions.”[2016] This was heat applied to existing 8CRV or HL products.
Thus almost five months after the NHS in Scotland had been able to provide nothing but heat-treated product from PFC, and despite the reassurances given in Parliament (which by inference had been given by BPL to the DHSS as to its progress, though it may have been that the DHSS continued to work off the November announcement to brief ministers) heat-treated Factor 8 product was generally and finally available on a universal basis. Unlike PFC, BPL did not offer recall and replacement of Factor 8.[2017] As for the commercial companies, some but not all offered to replace unheated with heat-treated product.[2018]
The problem of ensuring a supply of concentrate which was likely to be free of the virus which caused AIDS was not simply one of delays in achieving the necessary domestic supply.[2019] In England, Wales and Northern Ireland part of the picture remained a considerable commercial supply of products which had been made by pharmaceutical companies from sales to them of plasma (by individuals or brokers) which may not have been screened to exclude HIV. There was also some reluctance at some hospitals to pay the extra to purchase heat-treated commercial products, at a price premium, whilst non-heat-treated concentrates were available much more cheaply. It is to these two issues – reluctance to purchase heat-treated commercial products, and untested plasma sources – to which this chapter now turns.
It seems clear that there was some resistance by some clinicians to the use of heat-treated product.[2020] There may have been more than one reason for this. One may have been that NHS concentrate remained available, with the assurance that came from knowing it had been produced from plasma which had been voluntarily donated from a donor base in which the prevalence of AIDS (and therefore, presumptively, its viral cause) was relatively low by comparison with the United States. It may with some justification have been thought that though some risks came with the use of NHS concentrate[2021] very considerable ones did so with the use of unheated commercial concentrate, and this in turn led to the thought that applying heat treatment to what was demonstrably infective plasma as a base material may have been only partially successful. It may have been an attachment to the status quo.[2022] It may have reflected the fact that many haemophilia clinicians spent only a limited period of their working week as haematologists in that capacity, rather than more general haematology, and were not fully apprised of the options. A strong possibility however is the strain it would put on regional health finances, though many regional treasurers were entirely supportive.
Some indication of the cost pressures can be gleaned from three sources. The first is a record from the meeting of UKHCDO directors on 10 December 1984. The meeting having agreed that heat-treated product should be given to all patients if freely available, including those who were HIV positive, and should be obligatory for those who were HIV negative, Dr Savidge then commented that “this has and would continue to create severe financial problems for treatment centres.”[2023] The second is a couple of lines in a sales report about December 1984 produced internally to Cutter which read: “There are a few centres still using [unheated] NHS product. Those known are the London and small centres in South East London that cannot afford commercial material.”[2024]The third is a letter of 14 December 1984 to the North East Regional Health Authority.[2025] It pointed out the very considerable additional cost if it were to change to heat-treated product. Commercial providers were charging a minimum of 50% more per unit than they charged for non-heat-treated product. The letter implied, too, that existing stocks of non-heat-treated product might need to be replaced, for if heat-treated product were to be supplied because it was thought to be safer, that would be the logical consequence. By mid December 1984 those stocks were valued at over £33,000 in the North-Eastern region alone, and the incentive to seek to exhaust them first before switching to a wholly heated supply must have been strong so far as regional treasurers were concerned.
The summary in this particular letter from the district general manager to the regional general manager is to be applauded, but it is nonetheless revealing: “This is one of those rare circumstances where patient safety, family health, public policy and legal considerations all coincide to compel a decision to be made first [ie to deliver only heat-treated product] with any argument about money being undertaken subsequently.”It shows that the writer was conscious of the need to make a very strong case indeed that financial considerations should be secondary if their objective was to be achieved: in this region funding for heat treated concentrates was made available, but other regions may have been less forthcoming.[2026]
There was commercial pressure to continue purchasing non-heat-treated concentrate. In early December 1984, at the same time as UKHCDO directors were deciding that only heat-treated products should be used, an internal sales report to Cutter showed a determination to continue to try to sell it.[2027] A subsequent internal report of Cutter speaking of the UK sales position in May 1985 recorded that a small “short dated batch” was sold during the previous month,[2028] and that “several other contacts have shown an interest in other batches and the material has been offered for sale.”[2029] It should not, however, be over-interpreted: there is considerable evidence from Cutter’s internal paperwork that shows that despite the early December position, Cutter had been willing to take back unheated product for replacement with heat-treated concentrates from centres (and that most (though not all) centres had chosen to take advantage of this), and that as from mid March 1985 (if not before) Cutter had taken the strategic decision to stop selling unheated stock to UK centres.[2030]
It is also consistent with, and supportive of, concerns amongst leading haemophilia clinicians about the extent to which non-heat-treated product might still be being purchased and used. To obtain a proper factual basis for what was simply suspected to be the position, Professor Bloom issued a questionnaire to haemophilia centre directors. It asked whether (and to what extent) they were still using non-heat-treated product. At a meeting of the AIDS group of UKHCDO directors his analysis was discussed.[2031] It appeared to show that a substantial number of centres were still using non-heat-treated Factor 8, though only one centre was using commercial non-heated Factor 8 and two commercial non-heated Factor 9. The results were published in the British Medical Journal. The published article noted that some of the use of UK unheated Factor 8 “may have represented clearing of existing stock.” If this is well founded (and the fact that it is stated in a leading peer-reviewed medical publication in the UK indicates that it probably is), it records a conscious decision to use existing (unsafe) stock rather than acquire new (safer) stock.[2032] Dr Philip Mortimer, from the Public Health Laboratory Service (“PHLS”), told the meeting that he was concerned to see that a large number of centres were still using non-heat-treated Factor 8, and suggested that all directors should be advised not to use it.[2033]
The next meeting on 17 June 1985 of the AIDS group of UKHCDO directors agreed to recommend that only heat-treated product should be used thereafter.[2034] Their recommendation was emphasised when Professor Bloom, Dr Charles Forbes and Dr Charles Rizza then wrote to the British Medical Journal on 22 June 1985 on behalf of the directors of the UK haemophilia reference centres to “express our concern about the safety of blood and unheated blood products.” Their letter noted that “The safety of cryoprecipitate[2035] and unheated UK blood products with regard to HTLV-III infection can therefore no longer be assumed, especially as these materials may need to be administered in repeated doses … we no longer consider that the use of cryoprecipitate or other non-heat treated concentrates is justified.”[2036]
It nonetheless remained the case that some non-heat-treated product remained in the stock of commercial suppliers in the UK (presumably available for supply and sale if requested or thought necessary).[2037]
One of the more concerning issues is the failure of the CBLA (BPL and PFL) or the Licensing Authority to recall unheated stocks of domestic product in England and Wales,[2038] as had been done in Scotland. Part of the reason for this is linked to the failure of England and Wales to achieve self-sufficiency, since BPL in 1984 was not in a position to produce heat-treated product more quickly, nor produce more of it. Part of the reason was also articulated by Dr Terence Snape. He said that “At the time, the unheated UK product was still considered to be ‘a product of choice’ by many physicians and the product was not withdrawn … Some UK haemophilia specialists took the decision to continue to use unheated NHS concentrate, in preference to heated (US) commercial concentrate, until such time as 8Y was readily available.”[2039]It follows that there continued to be a demand for the product. Dr Snape records that it was not until Dr Harris, the Deputy Chief Medical Officer, wrote to all haemophilia centre directors (on 15 August 1985) to confirm availability of heated Factor 8 concentrates from various sources and advised “There would thus appear to be no longer any need to use un-heat-treated Factor VIII concentrate” that there was any definitive DHSS response to the threat to patient safety which the use of unheated product offered.[2040] It would follow, inferentially, that whereas in Scotland all unheated product had been recalled at the start of 1985, until August non-heated product remained in use in England and Wales.[2041]
By way of comment, it is understandable that there was reluctance amongst many clinicians to embrace commercial heat-treated products. Although Cutter[2042] and Alpha[2043] had both published the results of tests which showed that their heating processes had inactivated HTLV-3/HIV virus load to a degree sufficient to show they were almost certainly (generally) safe, and the use of heat-treated product had been strongly endorsed by The Lancet,[2044]the Medical and Scientific Advisory Council of the US National Hemophilia Foundation,[2045] the CDC[2046] and the Bureau of Biologics in Canada,[2047]it was rightly believed that the sources from which those products were made were likely to be more heavily infected than domestic products. AIDS was not the problem yet in the UK as it had been for a while in the US. There were questions of trust which were rightly to be asked, bearing in mind the way in which the World in Action documentaries had appeared to show that commercial rhetoric about the nature of their products did not correspond to the everyday reality of plasma collection from unsuitable persons keen to sell it to manufacturers or plasma brokers. There was as yet little direct evidence of how reliable claims were in practice. The UK had no facilities (apart from the Centre for Applied Medical Research (“CAMR”) Porton Down) capable of testing a batch to verify that it was truly virally inactivated so far as HTLV-3 was concerned. It might be the case that side effects would emerge from the use of heat-treated concentrates that had not yet become clear (although this had not yet been shown to be the case despite over a year of use of such products in North America). Moreover, it was not until early in 1985 that heat-treated commercial products were licensed for use by the regulator. To clinicians used to arguing for self-sufficiency, to avoid the dangers of commercially sourced imports, it would have stuck in their throats to seem now to endorse commercial products rather than domestic ones simply because their manufacturers claimed that they had been heat treated. A supply of heat-treated domestic concentrate was in the offing. It is not difficult to see why clinicians may have preferred to wait rather than to change their treatment practices for what would probably seem only a short interim period before domestic supply of heat-treated product increased. Further, commercial products were believed to be more likely to carry hepatitis than domestic ones.
Understandable though this reluctance was, it did not excuse continued use of unheated products beyond a short period into 1985. Nor was it, ethically, the clinician’s choice: the patient should have been alerted to the balance of risks and advantages, reminded of the alternatives of no treatment in some circumstances, or of cryoprecipitate, and given information sufficient to enable them to make the choice. Part of that information should have been that haemophilia centre directors had since 10 December 1984 collectively thought that priority should be given to heat-treated products over unheated ones. Dr Richard Tedder (albeit not a treating clinician) had indeed reminded clinicians on that date that “advice to patients should go hand in hand with treatment”.[2048] Yet the evidence is clear that, in the main, patients were not given the information or the choices it involved.
Assessing that unheated Factor 8 concentrates should not have continued long in use into 1985 is not substituting a judgement purely in retrospect for that made at the time: the critical point is that from 10 December 1984 onwards, in the light of their assessment of the available material at the time, the leading clinicians[2049] had reached the view that heated concentrates, whether commercial or domestic, were safer so far as the risks of transmission of HTLV-3/HIV were concerned. The question then becomes what the consequences of recognising a risk to health should have been. The answer is removing the risk, as far as was practicable.
If unheated Factor 8 concentrates had been recalled, there could be no realistic possibility that treatment would be made using such products. It was the logical corollary of recommending the use of heat-treated product on the grounds of safety. Commercial heat-treated Factor 8 products were available. Safety argued for their use when a factor concentrate was needed and domestic product was not available.
By contrast, as soon as heated Factor 9 product was routinely issued all unheated stocks were recalled.[2050] The principle of recall was thus undisputed, but a similar process did not happen with Factor 8.[2051]
It is difficult, therefore, to justify the failure to recall stocks of unheated Factor 8 product, at least by the start of the next financial year (ie after 31 March 1985),[2052] by which time commercial heat-treated product was licensed, and it was obvious that supplying such a product was to take an unjustified risk with the safety of any patient.
There had, until 1985, been little recent history of commercial Factor 9 concentrates being purchased. The UK was in essence self-sufficient so far as this product was concerned. However, at a UKHCDO Hepatitis Working Party meeting on 6 February 1985 Dr John Craske identified eight patients treated with (unheated) Factor 9 who had seroconverted.[2053] Reporting the meeting to Dr Lane, Dr Snape wrote: “a significant number of HTLV-III Christmas disease patients, treated only with NHS IX and with no other risk factors, argues strongly for haste with manufacture of heated factor IX.”[2054]
To begin to use commercial heat-treated product was likely to protect patients better against the risk of AIDS, but would expose patients to a greater risk of hepatitis. Though heat treatment may have reduced the risks of hepatitis – as some results indicated it might – it did not eliminate them, leaving it a close call whether patients would be safer overall being given NHS Factor 9 concentrate rather than heat-treated commercial factor concentrate. The choice was properly that for the patient to make. Clinicians should have discussed it with patients, who should have been told about the merits and demerits of the options. There is no evidence that this happened. The Inquiry would be likely to have had some trace of it if it had. The survey published in the British Medical Journal showed that a fifth of centres were using heat-treated commercial Factor 9.[2055]
BPL and PFL issued some heat-treated Factor 9 for clinical evaluation in July 1985 and it became routinely available from October 1985.[2056] Between June and October there was a discontinuity of supply from BPL, with little or no unheated Factor 9 released for sale after June and the first batches of heated Factor 9 for regular issue not released until September. Commercial heat-treated products filled the gap.[2057] There had been particular concerns that if Factor 9, produced from a later fraction of plasma than was Factor 8, and subjected to a slightly different process of manufacture, were to be exposed to significant heat in manufacture it might cause thrombosis when administered. Concerns about thrombogenicity had to be resolved, therefore, before the product could be issued. This was done with experiments in dogs prior to clinical trials in humans.[2058]
BPL and PFC recalled unheated Factor 9 in October 1985.[2059]
Scotland had produced DEFIX, which was virtually identical to the product of BPL/PFL (“9A”). There were similar worries that use of it might lead in some cases to thrombosis. After researchers at PFL and PFC had each discovered that a relatively small change to the product formulation was all that was needed to be able to withstand dry heat treatment at 80oC for 72 hours and pass a laboratory test for thrombogenicity, it remained only for studies of thrombogenicity in animals to be completed successfully before it could be routinely released. The studies were completed in August 1985. Heat-treated Factor 9 was issued routinely from the beginning of October 1985, and any stocks of the unheated DEFIX were recalled and destroyed.[2060]
Though the amount of heat and time of exposure to it varied between the heat-treated products offered by the principal manufacturers, given their differing manufacturing processes, all were usually free of the risk of transmitting HIV. However, this did not apply with the same force to Factorate, made by Armour (US), as it did to the products of other companies.
By early May 1985 Armour had learned that a batch of heat-treated Factorate to which a donor who had subsequently developed AIDS was known to have contributed had been distributed to eight centres in the UK between December 1984 and January 1985.[2062] In July 1985 Armour was informed that a patient in Lewisham had seroconverted after receiving a dose from this batch and noted that “This patient is the first to show sero-conversion from HTLV-III negative to positive following administration of the batch of Factorate Heat Treated in question.”[2063]
In December 1984 Armour (US) had contracted Dr Alfred Prince, an eminent virologist, to conduct viral inactivation tests on its product, the purpose of which was to determine whether a measured quantity of HTLV-3 would be inactivated by the heat treatment regime that Armour (US) had adopted in manufacturing it.[2064] On 24 January 1985 Dr Prince reported: “Disappointingly the HTLV-III stock which had previously titred 10 5.3 TOID 50/ml gave a titre of only 102.5 to 103.0 when tested at a 1:4 dilution. Thus we were unable to show the >5 log kill as had been hoped. The most that can be concluded from the study is that the combined effect of lyophilization and heating inactivated ≥2.5-3 logs.”[2065] His subsequent conclusion as reported to Armour (US) later in 1985 following further studies[2066] was that Generation I, Generation II and Factor IX were not rendered virus free when they had been contaminated with HTLV-3 and heated in the dry state at 60°C for even as much as 72 hours. Dr Prince recognised that his findings were “in marked contrast” to those reported by Dr McDougal and Dr Evatt on behalf of CDC and noted that “It is difficult to explain the difference between the results reported by McDougal et al and the present findings.”[2067] In November 1985, Armour (US) refused permission to Dr Prince to make this information public.[2068]
However, in February 1986 the possibility that Factorate HT, Armour’s heat-treated Factor 8 product, might have caused HIV transmission became widespread knowledge. It did so because on 12 February Dr Peter Jones told a conference in Newcastle of suspected seroconversions after using the Armour product in the Netherlands and the US.[2069] Armour, though they had been told of the possibility of such a seroconversion in Lewisham, had still not reported this to the DHSS.[2070]
Following these revelations by Dr Jones,[2071] the DHSS sought confirmation on 13 February that all the Factor 8 “now being supplied” by Armour in the UK was collected from donors who had individually been tested for the presence of HIV/HTLV-3.[2072] Dr Peter Harris of Armour supplied this confirmation on Armour’s behalf.[2073] Robert Christie of Armour provided a document to the sales force dealing with the fallout from the Newcastle revelations. In it, he said that the view expressed by Dr Peter Jones was premature and speculative.[2074] In evidence to the Inquiry, Christopher Bishop said that this was based on advice from the US and UK medical people.[2075]
At the same time as providing this document to the sales staff it was known that Armour in the UK still held stocks of Factorate which came from untested donors.[2076] At an Armour (US) meeting on 20 February 1986 in Fort Washington it was acknowledged that the heat treatment regime might not be totally effective and the decision was taken to upgrade the heating cycle “since it appears that higher longer temperature is more effective.” Shipments of concentrate from unscreened donors would be stopped but “centers where unscreened donor product may have been delivered will not be contacted until the situation is clear.” This included centres in the UK which “may have received product within the last three months.”[2077] Seven days later there was another meeting in Fort Washington and it was agreed that Armour (US) would continue to withhold distribution of unscreened product “as long as, or unless, we only have that type of product to distribute within the market.”[2078]
In late February 1986 Dr Jones wrote to Armour to say that, in particular, their product should not be given to “previously untreated seronegative patients” and that he was “particularly averse to its prescription for children.”[2079]
The DHSS followed up its communications with Armour at a meeting on 3 March 1986. By this time the Lewisham case had been reported to the DHSS, Dr Harris of Armour stating in an internal memo on 18 February that “I am now obliged to report Dr [David] Whitmore’s patient who sero-convereted following treatment with Factorate HT Y69402 (AIDS donor in pool) to her as Dr Whitmore has confirmed that the patient remains HTLV-III positive.”[2080] The note of the meeting made by Armour records “We were asked how much material was in the market originating from unscreened donors. We estimated approximately 5 million units or about 3 months’ stock. We were not asked to withdraw this material.” The note recorded further that “There was no evidence that the DHSS regard our current heat treatment method as unsatisfactory, but are looking for evidence that we are steadily moving towards improved procedures of screening and processing that will provide extra guarantees of safety … No indication was given that they wish us to withdraw batches of product from unscreened donor pools.”[2081]
In a paper on the safety of heat-treated Factor 8 prepared by Dr Rotblat of the DHSS the following day, she reported (referring to the Lewisham and Netherlands cases) that there were two cases of seroconversion after treatment with heat-treated Factorate from a batch known to contain a donor who had AIDS; the US case (understood to have involved a Hyland product) was described as one with other risk factors.[2082] In relation to the Lewisham patient, Dr Rotlbat recorded that information had been obtained from his physician and that he “is a mild haemophiliac who has no other risk factors. He was tested for HTLVIII antibodies in January 1985 and found to be negative. He had received no treatment since 1980. In February 1985 he received two bottles of batch Y60402 and HTLVIII antibodies were found in May 1985 and confirmed in November 1985.”[2083]
The paper was considered by the Biologicals Sub-Committee of the Committee on Safety of Medicines (“CSM(B)”) on 5 March 1986 which decided that there was “insufficient evidence for action to be taken on any specific product” but that “close surveillance should be maintained on the two possible cases of HTLV-III transmission in recipients of Armour material.”[2084] CSM(B) advised that “if any of the data provided by manufacturers on viral inactivation suggested a danger, urgent consultation should be sought with appropriate members.”
The Expert Advisory Group on AIDS (“EAGA”) also considered Dr Rotblat’s paper at its meeting on 11 March.[2085] It discussed whether there was a need to issue a statement on the safety of heat-treated Factor 8 “to counteract that made by Dr Jones.” It was agreed that a statement should be made as follows, subject to review by the CSM: “The EAGA has carefully considered the safety of currently available Factor VIII and IX concentrates in the light of the most up to date medical information. As a result, the EAGA has concluded that there is no evidence that HTLVIII infection has been transmitted in heat treated Factor VIII and IX concentrates.”
It is difficult to understand how EAGA felt able to agree to issue a statement that there was “no evidence” when its own discussion of the cases described to it by Dr Rotblat acknowledged that the Lewisham patient (referred to in the minutes as the patient with mild haemophilia who had not received treatment since 1980) could not be explained by late seroconversion.[2086]
On 13 March 1986 Dr Harris of Armour wrote to a number of haemophilia centre directors providing data about Armour’s viral inactivation process. The letter asserted that there had been no reported case of AIDS and no reported seroconversion associated with the administration of Factorate to “a virgin patient not at risk for AIDS.” This latter claim was capable of being misleading in light of the information in Armour’s possession about the Lewisham patient. If a “virgin” patient is regarded as someone who had never been treated with blood products, this assertion may be strictly true. However, though he had had treatment between 1975 and 1980, and adopting the terminology in use at the time, was not necessarily a “virgin” so far as concentrates were concerned, he was in a very similar position to a “virgin” patient. He had received no treatment with concentrates since 1978, and no treatment at all since 1980 (when treated with cryoprecipitate). He was HIV negative in January 1985, was treated with batch Y69402 in February 1985 and was HIV positive in May 1985. He was in no other risk group for AIDS.[2087] Accordingly, the omission of any reference to the Lewisham case is of concern.
The letter continued by emphasising that each donation “is now specifically screened for HTLV-III antibody and all product being supplied is donor tested.” It was acknowledged that there might be material in centres or in the home that was not derived from donors tested for anti-HTLV-3, which would “aggravate the potential for distress to the haemophiliac, because of the patient’s inference that non-donor tested material may be less safe with regard to the AIDS risk. Further, we recognise that any decision to give a patient this information rests with you as the unit director.”[2088]
On 15 March 1986 The Lancet carried a report of HIV seroconversion in a person with mild haemophilia following administration of high doses of a heat-treated Factor 8 concentrate at North Carolina Memorial Hospital in Chapel Hill in the USA.[2089]
The Committee on Safety of Medicines (“CSM”) considered the safety of heat-treated Factor 8 at its meeting on 26 March 1986. Dr Jones had written to the CSM on 17 March 1986, stating that it would appear that, contrary to an earlier Armour statement, Factor 8 concentrate which had not been individually donor tested was still in circulation. Dr Jones urged that any material which had not been “(a) collected in low risk areas, (b) individually donor tested and (c) heat treated in a manner approved by [the CSM] be withheld, at the very least, from seronegative people.”[2090] However, the CSM merely endorsed the recommendations of CSM(B), agreeing that there was insufficient evidence for action to be taken on any specific product.[2091] The minutes of the CSM meeting make no reference to Dr Jones’ communication or to The Lancet report: they refer only to Dr Rotblat’s paper and the CSM(B)’s recommendations.[2092]
On 10 June 1986 Dr Rotblat reported to Dr Alison Smithies that Armour in the US had been told that if they had a seroconversion (such as the Lewisham case) “they should put this on their data sheet.” She observed that Armour “are extremely anxious about this” and that Dr Harris of Armour was trying to persuade Dr Whitmore to release some plasma to carry out Western blots on the Lewisham patient to make sure that this was not a false positive result.[2093] She recorded that “I feel that really we have no further information than we had at the EAGA meeting when I presented the response to Dr Jones’ letter.” Dr Rotblat was intending to discuss the matter further with Robert Christie of Armour to ascertain if he had any possible new evidence.[2094]
On 11 July 1986 Dr Harris of Armour wrote to haemophilia centre directors recommending the return of all non-donor tested Factorate so that it could be exchanged for material manufactured from screened donations.[2095] Although the letter was said to be written with the agreement of the DHSS, it does not appear that it was being sent as a result of any action by the DHSS: it may have been prompted by the fact that Armour in the US had the previous month written to all US blood bank directors and haemophilia treatment co-ordinators recommending the return for exchange of any non-donor tested material.[2096]
The response to the steps taken in the US was mixed. Christopher Bishop had wanted to prepare a “defence” document designed to restore confidence in Armour’s heat-treatment process and stop further deterioration in sales.[2097] He maintained that there was “yet no proof” that a British patient had developed antibodies as a result of treatment with Factorate and that the Dutch patient “was not, repeat not, a clean virgin patient.” He continued: “Unfortunately, the mention of Dr Michael Rodell’s statement that we are reviewing our heat treatment process now prevents us from preparing an official ‘defence document/article’ to The Lancet … We can not [sic] on the one hand defend our existing treatment and then immediately introduce a new one”.[2098] Dr Harris likewise expressed concern: “the American exchange programme of Armour product took everybody by surprise and has put us in a potentially very weak situation with regard to the DHSS and haemophilia unit directors.” He referred to the possibility that “the DHSS, having put our product under the microscope, may start to ask us awkward questions concerning product safety … there will be some difficulty in defending too hard our present product in the light of publicly announcing … our interest in developing a more stringent heat treatment process.” Dr Harris reported that Dr Rotblat “had been summoned to the Chief Medical Officer of the DHSS to answer questions concerning our product recall and discussions held in March concerning potential problems with Armour Factorate HT.” He added that Dr Rotblat was “no longer to be viewed as a sympathetic ally” and that “I do not believe that we have her goodwill any longer”.[2099]
On 7 August 1986, Christopher Bishop recorded (referring to concentrate produced under the existing heat-treatment regime) that “we have a considerable quantity of existing material in inventory and the last thing we need is for people to hold off ordering until the new product comes through.”[2100]August also saw reports of a further possible seroconversion (in Swansea) following treatment with batch Y69402, which it reported to Dr Rotblat.[2101]
On 29 September 1986 Dr Frank Hill at the Birmingham Children’s Hospital rang Armour to report that two children who had been treated with Armour heat-treated product had seroconverted. Dr Harris “reported the findings in broad outline to Dr Rotblat at the DHSS and promised to supply further, more detailed information as soon as we receive the written report promised by Dr Hill.”[2102]
An Armour file note of a conversation between Dr Rotblat and Dr Harris of Armour on 1 October 1986 reported that it was currently DHSS opinion that one of the Birmingham seroconversions was probably the result of heat-treated Factorate: “Add to this the sero-conversion case in Lewisham and it is DHSS opinion that we now have two established sero-conversions with our heat treated product. Dr Rotblat questions the safety of our heat treatment and notes that this is the least stringent of the dry heat treatment processes.” It was the DHSS’s feeling “that the Armour product may need to be removed from the market.”[2103] Dr Rotblat’s senior, Dr David Jeffreys, telephoned Dr Harris the following day to indicate “You are no doubt looking at voluntarily withdrawing the product on Monday.”[2104]
On 3 October a meeting with Armour took place at the DHSS, with Dr Rotblat providing a summary of the current position “as seen by the DHSS”: namely that there were two cases of clear-cut seroconversion in response to heat-treated Factorate (the Lewisham case and one of the cases reported by Dr Hill) and three other cases where there was “not quite such a definite product relationship” (the Dutch case, the Chapel Hill case in the US and the second case reported by Dr Hill). The upshot of the meeting was that if Armour did not agree to a voluntary withdrawal the DHSS “would need to consider the case further as to what their course of action should be.”[2105]
On 7 October 1986 Armour’s heat-treated Factorate was withdrawn from distribution in the UK and Armour relinquished its two product licences.[2106]
From the information available to the Inquiry, the behaviour of Armour in the respects highlighted gives rise to a number of concerns. Armour did not report the Lewisham case to the DHSS until February 1986, despite being aware of it since July 1985.[2107] Its letter of 3 October 1985 was potentially misleading in its omission of reference to that case. Armour did not, as far as the contemporaneous documentation suggests,[2108] bring Dr Prince’s concerns about the effectiveness of its heat-treatment process to the attention of the DHSS: it could have communicated those concerns whilst also drawing attention to the conflicting results obtained by others.[2109] Armour confirmed to the DHSS that all product now being supplied to the UK was from donors who had been individually tested, but there remained in stock product from unscreened donors that Armour was apparently open to supplying. Armour did not voluntarily withdraw all such material, as it should have done in the interests of ensuring patient safety. The letter sent by Armour to haemophilia centre directors in March 1986 was misleading by omission in the absence of any reference to the Lewisham patient. When in July 1986 Armour in the UK finally wrote to directors recommending the return of all non-donor tested Factorate, it did so having effectively had its hand forced by the decisions of its parent company in the US. The contemporaneous documentation supports an inference that patient safety was not accorded the weight that it should have had during this sequence of events. .
The conduct of the regulatory authority (for practical purposes, as Dr Walford had described it in her evidence, the Medical Division of the DHSS)[2110] from February 1986 was also wanting.[2111] It did not take any regulatory step to ban or secure the withdrawal of the product until October 1986 when it did belatedly achieve a withdrawal by Armour without the necessity of a process which could involve a series of appeals and hearings. It is surprising, and disappointing, that Armour were not asked to recall all the stocks which had been distributed and came from untested source plasma. Although the issue came promptly to the attention of the CSM(B), its decision, subsequently endorsed by the CSM, that there was insufficient evidence for action to be taken failed to place safety at the centre of decision-making. EAGA’s agreed statement went even further, concluding that there was “no evidence” that HIV had been transmitted in heat-treated concentrates and thus ignoring the Lewisham case. It took the report from Dr Hill for the DHSS to act. Whilst action then was prompt, it should not have taken the report from Dr Hill to push the Licensing Authority into action.
It is further surprising and disappointing to note that the Chief Medical Officer’s (“CMO”) immediate response to Dr Jones’ actions in February 1986 was to condemn them,[2112] at a point in time when the CMO could not have known whether Dr Jones’ claims were capable of substantiation or not, and that a DHSS spokeswoman felt able to say that the Netherlands case could be discounted, when the DHSS could not have known at that time whether or not the Netherlands case was one of seroconversion caused by Factorate. These responses, and those of the CSM(B), CSM and EAGA, are unhappily redolent of the “no conclusive proof” line that had been erroneously adopted by the DHSS in 1983.
It is also a matter of comment that when Dr Hill rang the Armour representative, the confidential memo circulated by Robert Christie contained the following: “Dr Hill agreed that this incident should be reported to the DHSS and he also believed that a publication describing his experience should be prepared. In the latter case, he was happy to consider Armour participation in such an article at whatever degree was considered appropriate.”[2113] It is concerning that when a serious infection was identified in patients as a consequence of having a particular product, with implications for public health because others might in turn have been infected by that patient, that the first port of call of the clinician concerned should not have been the DHSS, but was instead the manufacturer.[2114] It is difficult to understand quite why Armour was offered “participation” in any article about the matter, rather than being told of the form of the publication and permitted to comment if they wished.[2115] It appears from the terms of the memo that it was an employee of Armour who reported the findings to the DHSS, and not Dr Hill.
Finally, the following exchange occurred at the end of the evidence of Christopher Bishop. He asserted that Armour had done:
“everything possible to provide the best possible treatment and the most up-to-date systems in accordance with the state of art at that time. It’s very easy to be Monday morning quarter backs who will have the benefit of hindsight.
Q. … Is there anything you think you or Armour should have done differently with regards to your non-heat-treated product?
A. No.
Q. Anything you or Armour should have done differently in relation to the heat-treated product?
A. No.
Q. Having regard to the documents that we’ve looked at today, do you accept that Armour should have withdrawn the heat-treated product earlier than October 1986?
A. No, I do not accept that.
Q. Do you accept that Armour should have been more open and transparent with the information it was providing to clinicians about possible risks from its heat-treated product?
A. No, I think we did everything we could with the information that we had available on any patient or the disease, or what have you. We at all times -- you know, we did, I feel -- and I’m very proud of the fact that we did do everything in the right way.
Q. Were any lessons learnt by Armour from what had happened?
A. Not that I -- no, no specific lessons because we, you know --again, you know, with the benefit of hindsight lots of things could be done differently. But we didn’t, you know, we didn’t have the benefit of hindsight.
Q. It might be said, at least in relation to the 1985/1986 period that we’ve been looking at, that Armour’s overriding focus was concern about losing ground to the competition rather than ensuring the safety of patients treated with its product. Do you have any comment on that?
A. That was my -- as a marketing person, for which I was employed, that was a major concern, commensurate and secondary only to the safety factor and the welfare of the haemophiliac patient and his family and the teams looking after him.”[2116]
It is difficult to reconcile those answers satisfactorily with the material and the evidence set out above.
When heat treatment was introduced, it was at a time before tests to screen donations were regularly available. The “Armour saga” showed the risks of product being made from plasma which had been donated by some donors who had not been tested for the presence of HIV, although their heat treatment also proved inadequate. Having the dual reassurance both that donations had been tested and the product had been subjected to viral inactivation procedures was important, especially in the period shortly after the introduction of heat-treated concentrates.[2117] Until a little time had passed for experience of the use of the eventual products to build up, it could not have been known for sure how reliably one or the other or even the combination of the two would work in eliminating risks of AIDS.
Universal testing of blood donors for HIV/HTLV-3 did not begin in the UK until 14 October 1985. Even that did not give rise to the testing of plasma which was used as the base material for heat-treated factor concentrates. PFC Liberton first issued Factor 8 from plasma tested for HIV/HTLV-3 in February 1986.[2118] In this respect, they were not far out of step with some pharmaceutical companies: the first batch of Cutter product, Koate HT, which was made from 100% tested plasma was shipped to the UK in January/February 1986.[2119]
There was, of course, a gap between production of factor concentrate and its distribution to haemophilia treatment centres. At the end of June 1986 Dr Foster reported to the directors of SNBTS at their meeting that the Factor 8 concentrates being issued (ie distributed) were derived from unscreened plasma, but it was anticipated that the position would change fairly soon. By contrast, “most of” the Factor 9 products were now derived from screened plasma.[2120]
The use of products made from unscreened plasma, the dangers of which were highlighted by the Armour saga, was again evident in July 1986. An internal Cutter memo recorded that although “Cutter will only sell 100% screened material”nonetheless “some Centre Directors are happy to use up their existing stock of unscreened Koate HT.”[2121]
In Parliament, Baroness Trumpington, who had succeeded Lord Glenarthur as Parliamentary Under-Secretary of State for Health, made clear that NHS products derived from screened plasma would become available for distribution during August 1986 throughout the UK.[2122] The distinction here is between production and distribution. There is a further stage: that of use. In a letter from Dr Rizza to the DHSS he records that:
“BPL will start releasing 8Y prepared from tested donors by the middle of August and by the end of September, if not sooner, all the NHS factor VIII being issued will be from tested donors. There will therefore be a 4-6 week period during which there will be a gradual change from untested to tested material being issued. I gather that the proportion of untested material issued to begin with may be of the order of 50%.”[2123]
Of course, what has been issued previously may remain in stock, and thus may continue to be used for a while unless and until it is recalled. There is some evidence that some of this stock of NHS products made from unscreened donations was destroyed, but little evidence of recall as such.[2124]
8Y, produced by BPL, not only protected against the risk of AIDS but it progressively became apparent that it was also effective against hepatitis viruses. By the end of July 1985, though 8Y had not yet been widely distributed, BPL were in a position to issue information sheets which stated that the clinical trials of 8Y at six haemophilia centres showed that several patients had by then safely passed the point at which the first evidence of non-A non-B Hepatitis viral transmission would normally occur with non-heated Factor 8.[2125] These results were repeated with greater assurance, because of the greater lapse of time, in May and then again September 1986.[2126]
Scotland produced a similar product, Z8, at PFC – but this was from April 1987.
Why was it that Scotland lagged behind England in producing a hepatitis-free product? An explanation was forthcoming in the evidence of Dr Peter Foster to two Inquiries – first, the Penrose Inquiry and, second, this Inquiry.
The background to this is that PFC in Scotland started to experiment with heat treatment before BPL did in England. As explained already, the development in England was hindered by delay, which was in part a consequence of a lack of funding and a lack of will to achieve viral reduction in factor concentrates. However, the English efforts led to the development of what came to be known as 8Y.
From March 1986 onward (approximately six months after 8Y was routinely issued in England and Wales) Dr Smith was able to say that the interim results of 8Y, albeit relating to a limited number of batches, suggested that the severe heating given to the English product (80° for 72 hours) had been more effective in preventing transmission of non-A non-B Hepatitis than the milder heating to which at least two commercial products had been subjected by their American manufacturers.[2127] Indeed, by 9 July 1985 it was already being reported that the clinical trial of 8Y was at a stage where “several patients have already safely passed the point at which the first evidence of NANBH transmission would have been expected.”[2128]
Though Scotland had begun before England, its research originally concentrated on seeing if pasteurisation would be effective. It did this not only because in theory pasteurisation offered greater potential for controlled heating, but also because of reports that Behringwerke had in 1980 developed a pasteurised product which appeared to be free of hepatitis. It was not unreasonable to look first to pasteurisation (wet heat) rather than its alternative (dry heat). The emphasis changed to dry heat-treating product when it became known that this would be effective against HIV, since it could be introduced much more quickly than its pasteurised equivalent.[2129]
BPL was a little ahead of PFC in beginning to experiment with dry heat treatment. It attributed the apparent success of 8Y in eliminating the transfer of hepatitis viruses to the degree of heat applied. They knew that heat could often destabilise a protein, and would do so with Factor 8 (a protein) unless particular care was taken. However, they believed that the plasma fraction used in their process could withstand as much heat as it did (80° for 72 hours) in the presence of an appropriate stabiliser becauseit had been made to be to be “high purity” – in other words, it did not contain much protein additional to the Factor 8 protein of interest.
As Dr Foster explained, the reason given for 8Y being able to withstand the heat treatment it did was thought to be because it was more highly purified. That led PFC biochemists to believe that their Scottish product could be heated even more severely than 8Y was, to give a greater margin of safety, because they could produce a very high purity Factor 8 concentrate in their research laboratory.[2130]
However, theory in this case did not correspond with reality. When they tried to freeze dry their very high purity product after heating, it did not withstand freeze drying. That then led to PFC designing a new freeze drying process. The high purity product then did indeed withstand freeze drying – but it no longer withstood heat treatment at 80° even though it was very highly purified. This was completely the opposite of what had been expected. Dr Foster went on to say: “But what we did discover was that a sample of existing Factor VIII that had been included in that experiment as a control did withstand dry heat treatment at 80 degrees, and that told us that BPL’s success wasn’t because their product was more highly purified; it suggested it was because it was the way it had been freeze dried.” When that was explored with Dr Smith at PFL, who had developed the process they realised that this was indeed the case. Accordingly, if they took a lower purity product, freeze dried it in a way which would be effective for that lower purity product, and then applied 80° heat treatment to it, that then would work.[2131]
So, in effect that was what Z8 was – a strongly heated intermediate to low purity product.
What Dr Foster was describing was a process of scientific discovery. No-one had realised until the practical tests were done at PFC that the magic bullet for securing a strongly heated freeze-dried product lay not in the purity of the product to which the heat was applied, but in the process of freeze-drying the results.
It was not careless in any way to take the approach which PFC had done. If the reason had been purity, it would probably have been successful, and the delay as between England and Scotland would have been a matter of a few months if that. A better product might have resulted. It would not have been 18 months as it was.
The reason the gap between England and Wales was as long as it turned out to be was largely (though not entirely) because BPL had been fortunate in having adopted a process which worked, and instead of accurately understanding the reason for their success had attributed a reason to it that misled those at PFC. Neither BPL nor PFC is in any way to be criticised for this: knowledge of how best to heat-treat products and freeze-dry them was still at an early stage.
There were some small delays which did not depend upon scientific revelations. These were firstly a delay in PFC resolving some problems with freeze drying in August 1986,[2132] and then a two month delay in the start of clinical trials of Z8. These had been due to start in December 1986 but did not begin until February 1987. Part of the reason for that was that no proper arrangements had been made to ensure that patients who took part in the clinical trials of this new product were guaranteed they would be compensated if the product being trialled caused harm to them. Dr Ludlam in particular was insistent upon this assurance being given.[2133]
Accordingly there is an explanation why in England a heat-treated product effective against hepatitis was available outside clinical trials some 18 months before one became available in Scotland; the other delays are real, but are minor by comparison. By way of comment, if (as this chapter concludes) research into viral inactivation had been pursued actively earlier as it should have been, any delay as between Scotland and England would have had less effect because the virus would have been inactivated earlier in both nations.
It should be emphasised that this is not an explanation for the infection of people with bleeding disorders in Scotland, the causes of which are multifactorial and addressed throughout this Report. Nor has it anything to say directly to people who were infected with hepatitis by blood transfusion rather than blood products. It does not deal with the question of whether Scottish patients were exposed for too long a period to hepatitis – but solely with the question whether they were exposed longer than they should have been by comparison with people with bleeding disorders receiving concentrates therapeutically in England.[2134]
Although initial results suggested that Hemofil was successful to some extent in reducing hepatitis infections, it began to be noticeable by the spring of 1985 that commercial products which had involved only dry heating of freeze-dried concentrate might not be as effective as those which applied heat in a “wet” process: not just Behringwerke, but also Alpha which used a solution of n-heptane. Commercial rivalries meant that pharmaceutical companies kept a close eye on the successes or failures of their competitors. The maintenance of market share was important. An internal Cutter memo in May 1985 headed Wet process vs. Dry process described how Dr Savidge had recently presented results of trials on the Alpha Factor 8 product, Profilate HT, which “provide evidence to support Alpha’s claim that Profilate HT is free from Non A Non B hepatitis.”[2135] Dr Peter Kernoff and Dr Richard Wensley had made similar reports. The memo included the comment that “After the results of this trial and many other small trials, it is becoming very difficult to resist Alpha’s infiltration into our accounts. Despite the loyalty of our clients, some Haemophilia Directors feel that it is unethical to use anything but Profilate HT, especially on virgin haemophiliacs and children.”The memo then went on to discuss ways in which market share might be maintained whilst developing a better Cutter product.[2136]
The position became clearer still in respect of commercial products at the start of 1986. An internal Cutter memo showed that all heat-treated product made commercially carried a significant, though reduced, risk of hepatitis. None had eliminated it.[2137] This memo reported that Dr Kernoff had shown that Alpha had a 20% level of infection;[2138] Cutter itself had shown a rate of 20% in “virgin or near-virgin” patients in studies in Bonn and Freiburg, and Hyland (Hemofil) had a rate of 80% in a multi-centre study conducted by Dr Pier Mannucci.[2139]
The general picture was that in relation to hepatitis, 8Y from BPL was the safest product to use,[2140] Haemate P (the pasteurised product from Behringwerke) the next safest and the third safest was Profilate HT, the Alpha product. This was reflected in a letter of July 1988[2141] which informed Immuno of Vienna that:
“the Regional Haemophilia Directors in the U.K. have sent a circular letter[2142] to all the Haemophilia Centres informing them that the only Factor VIII products to be used in the U.K. are as follows, in order of priority:
1. Factor VIIIY [from] BPL[2143]
2. Haemate P [from] Behring
3. Profilate [from] Alpha
A customer of ours who has constantly been in touch with us to establish when we are going to obtain a Licence, has contacted one of the Regional Haemophilia Director’s [sic] in response to this letter and has been informed that if she uses unlicensed products then she will not have any backing from the Haemophilia Directors and must take sole responsibility for its use. She is, therefore, now having to decide whether to change to another product. We will have to be very careful that this situation does not extend to Feiba[2144] as this currently provides a very important part of our turnover.”
It was not until the end of the 1980s that further significant developments occurred in viral inactivation. The use of genetically engineered blood clotting agents was announced in October 1988 at the Royal Free Hospital.[2145] These products, which are not made from human plasma and are therefore free of the risks of viral contamination, were known as recombinant. Solvent detergent products were progressively marketed. In October 1989 Alpha applied to vary its licence to incorporate its new solvent detergent process. In March 1990 it was licensed.[2146] It was very effective against viruses with a fatty (lipid) coat, but not against non-enveloped viruses, requiring a second inactivation step to eliminate viruses such as parvovirus.
By this time, too, self-sufficiency had largely been achieved.[2147]
The use of recombinant product was widely recommended by clinicians, and endorsed by patients, for whom the memory of HIV and hepatitis infections transmitted by blood products was all too raw. Cost delayed its universal availability. It became the subject of a campaign by the Haemophilia Society in favour of all having access to it, which was given added urgency when the threat of vCJD was shown to be both real and serious towards the end of the 1990s. Further details are given of access to recombinant in the chapter on Access to Treatment.[2148]
Could and should heat-treated products have come sooner in the UK? This is perhaps the critical question which arises from the facts set out in this chapter.
The critical fact which answers it, and from which it can confidently be said that the answer “yes” is not a judgement resulting erroneously from hindsight is this: the four principal commercial pharmaceutical firms which made factor concentrates in the US all developed heat-treated products which they claimed to have reduced the risks of hepatitis within a few months of each other in the very early 1980s. They had begun more intensive work towards this earlier, in the late 1970s. The idea that it might be achievable had come earlier still, as the work by Dr Wada shows.
This very fact demonstrates that the technology required methodical work, rather than a moment of individual scientific genius. The companies were in competition with each other.[2149] They patented their processes. They were working independently to achieve the same goal, of hepatitis reduction. The remarkable coincidence of timing of six large companies – the four principal US pharmaceutical producers, Immuno of Austria and Behringwerke of Germany – each with slightly different approaches, in making and marketing heat-treated[2150] product leads to the inference that the processes essential to its manufacture did not depend on a single inventive step, or on one scientist, such as the chance discovery of penicillin by Fleming. If it had been otherwise, one company would have achieved a result long before others.
The coincidence of timing did not depend on a watershed development in understanding elsewhere in science, nor on any technological breakthrough: there is no evidence of either. The timing of what occurred is nonetheless of significance, for the work of research, conducted separately in each of the six major firms, must have begun some time in the mid to late 1970s for it to bear fruit in the early 1980s. It was then sufficiently complete to enable the field and laboratory tests necessary for regulatory licensing from 1983 onward to be satisfied, and sufficiently advanced to justify production on the scale which followed.
It is also clear that it was not the risk of AIDS but the need to reduce hepatitis as far as possible that inspired the work, which in each case led to a similar result, albeit in each case by a slightly different production process.
It is central to fairness that where the risks of a treatment have been increased significantly by the actions (or failures to act) of those responsible for providing it, then the elimination or reduction of that risk should be fully resourced. Failing that, it becomes incumbent on the State to put patients back into the position they would have been had the risk been eliminated or reduced, as far as money can do it: but it should at the same time be recognised that this is always likely to be second best, since money cannot be an adequate substitute for health and life.
So far as viral inactivation measures in the UK were concerned, risk of suffering hepatitis had been increased both by a failure to act (not resourcing and encouraging research sufficiently, nor sufficiently early),[2151] and by actions for which the State has responsibility. These actions were: first, licensing commercial concentrates known to be likely to cause hepatitis to a greater extent than domestic products made from true donations;[2152] second, acquiescing in, or failing to regulate, repeated increases in the size of pools from which domestic plasma products were being made. One of the ironies of the position into which domestic production after 1973/4 came is that as awareness grew stronger during the rest of the decade and into the early 1980s that viruses contaminated blood products and people suffered as a result, so also did plasma pools used for production at BPL grow ever larger too. It is another of the ironies that as appreciation of the risks grew stronger and stronger over this period, properly resourced opportunities and facilities for meaningful research into how best to reduce them became less and less available in England (until the early 1980s).
Both taking steps which were known to increase the risks of hepatitis to people with haemophilia, and acquiescing in very significant increases in pool sizes[2153] which inevitably amplified that risk, were actions for which the state had responsibility. In short, if steps are taken which increase risk, reasonable steps must be taken to see if that risk can be eliminated, and if not, reduced.
The measures that could be taken to reduce the problem of an infection caused by what was at the time[2154] an unidentifiable[2155] virus included[2156] researching methods of viral inactivation that might well be effective, and then conducting a trial of the resultant product. This required sufficient resourcing (both human and financial), sufficient facilities in which to conduct the research, and the political will to make it happen. None happened soon enough. By the time that commercial methods were developed for at least partially reducing hepatitis infectivity, almost all people with severe haemophilia receiving regular treatment with concentrates had been infected with non-A non-B Hepatitis.
The essential technology to manage some effective inactivation by heat was as available in the 1970s as it was in the early 1980s (there were refinements over time, but the basic essentials were the same).
If research had been purposefully pursued from the mid 1970s onwards in the UK (therefore some six years before it was) would the result have been a product that would at least have reduced the risks of hepatitis, and of the viral cause of AIDS, if not eliminated them?
As I will go on to discuss in greater depth, experts in the US have since commented that given some resource and the necessary will it is reasonable to think that inactivation could and should have been achieved earlier than it was in the US.[2157] What was true of the US was all the more true of the UK, since it was incumbent on the State, for the reasons set out above, to support research and development whole-heartedly. It was the view, for instance, of Professor Edward Tuddenham, who had been a director of one of the two largest haemophilia centres in England – the Royal Free Hospital – and who was particularly interested in research into aspects of Factor 8, that it should have happened in the UK.[2158] He was not alone in this.[2159]
Different views have been expressed from impressive sources who were particularly expert in protein chemistry. One was Dr Foster. He was a biochemist, who became head of the PFC research & development department throughout the period of central interest to the Inquiry: April 1974 to February 2009. Another was Dr Frank Putnam, a university professor in the US. Dr Foster took the view that Dr Putnam was a very eminent academic protein chemist who was taken seriously, and deserved to be.[2160] Dr Putnam gave evidence in the multidistrict litigation in the US on behalf of the plaintiffs, against pharmaceutical companies. In his evidence he described why he believed that pasteurisation of Factor 8 could have been achieved much earlier than it was. Dr Foster disagreed. His opinion was that pasteurisation of coagulation factors could not have been developed earlier. Despite his view of Dr Putnam’s eminence and expertise he thought that Dr Putnam’s evidence in the US litigation was based on hindsight: that “knowing how Behringwerke had stabilised their factor VIII, he had outlined a set of experiments to produce the same answer.” He thought that the technology of heating Factor 8 in solution was difficult. The difficulties created problems in reaching a sufficient output of finished product: it could not (at least initially) be produced in sufficient quantities to make commercial production viable.
Nor did he think that an alternative to pasteurisation – solvent-detergent treatment of Factor 8 (as patented by Dr Shanbrom in 1980) – could have been developed into production any sooner than it was (reported in 1985 and put into production later by the New York Blood Center).[2161] The chemical solvent/detergent would have to be removed from the product after viral inactivation to make the product safe for human use, but manufacturing technologies suitable for achieving this were not fully developed until the mid to late 1980s.[2162]
In the course of his testimony, there was nonetheless the following exchange:
“Q. [In the late 1970s] the underlying science of heat treatment was understood and known. There was nothing particularly novel about heat treatment as a concept, was there?
A. No.
Q. In terms of the reason why the heat treatment of Factor VIII wasn’t developed earlier, what was the main missing piece of knowledge? Was it how to maintain the stability of the product?
A. Yes.
Q. Was that the result of a lack of technological advances? Was there not the relevant substances or equipment available or was it just that scientists had not yet worked out what the solution might be?
A. It was a lack of knowledge about Factor VIII. The Factor VIII molecule wasn’t defined -- I mean, it wasn’t purified until Ted Tuddenham did it in the mid 1980s. And in the 1970s it wasn’t even known what Factor VIII was. Some people thought it was a carbohydrate. The [size] of the molecule wasn’t known. When I got involved it was called the Factor VIII complex, but it turns out that the measurements we were making of that were actually detecting the von Willebrand protein, not the Factor VIII protein. How the Factor VIII protein was biochemically put together wasn’t known at all. What was known was that it was highly unstable. Even at room temperature, and at slightly warmer temperatures, the activity was lost quite quickly. So it seemed to be the idea of heating just wasn’t conceivable. Because -- heating in a way that you had to destroy the virus as well, that just -- wasn’t just heating on its own.
…
Q. Do you think, looking back now, if PFC had had greater resources, that you might have been able to develop a heat-treated product earlier?
A. No, I don’t.
Q. Why is that?
A. Because I think -- as I say, the work -- the way it was discovered was a series of accidental discoveries made by certain people, and then that led -- opened up the way. And I can’t -- I don’t think that it would necessarily have happened at PFC if we’d had more staff. It was [sic] just happened -- it was just circumstances in that one particular company.
Q. Again, looking back now with all the knowledge that you now have, do you think that PFC should have embarked upon work relating to pasteurisation earlier than it did?
A. No, I don’t. Because I think what was most critical was evidence that the viruses could be destroyed by these processes and the agent for non-A, non-B hadn’t been discovered, the agent for AIDS hadn’t been discovered. So nobody could work out how to deal with them. How do you remove something that hasn’t been discovered? That’s not straightforward.”[2163]
These views owed a lot to Dr Foster’s personal view that heating concentrate, whether by dry heat, or by pasteurisation, to a temperature sufficient to destroy viruses was to heat it to a temperature which was certain to destroy the Factor 8 protein as well, since Factor 8 was known to be unstable, and would deteriorate very easily in heat. This meant that treating concentrate with heat during manufacture was irreconcilable with producing a usable product. His personal view went back to his student days: in what was in 1964 the foremost textbook on biochemical engineering he had learned that “Albumin can be pasteurised at 60°C for 10 hours but the other fractions are heat labile.”[2164] He described how in 1975 his own practical experience at PFC supported this statement. What happened was that preparation of the Scottish Factor 8 concentrate involved filtration using a membrane filter. Filtration was being performed at 20°C. It proved difficult. PFC therefore consulted Dr Alan Johnson in the US, who had devised the filtration method, to see if the process could be improved. He advised that filtration should be performed at 30°C rather than 20°C. This would increase the solubility of fibrinogen[2165] which Dr Johnson thought might be the problem, since he believed it was partially blocking the filter, thereby holding Factor 8 back and slowing down the whole process. PFC changed the process as he suggested. This succeeded in improving filtration, but at a cost. PFC noticed that filtration at that degree of heat resulted in an even greater loss of Factor 8 activity than at 20°C. It therefore reverted to the use of the lower temperature. Even a rise of just 10°C, to a relatively low heat, had resulted in too great a loss of Factor 8 activity.[2166]
Given his training, his experience in 1975, and a general perception amongst many fractionators to the same effect, I do not criticise Dr Foster for having the firm view he indicated, such that he was “shocked” when he heard of Behringwerke’s claims in 1980.
The view that heating could not be done without destroying Factor 8 was, however, wrong – as the history has shown.
There can be little doubt that the US Committee to Study HIV Transmission through Blood and Blood Products (whose report was informed by a significant number of experts in relevant fields) was correct in its analysis in 1995, to the same effect as Dr Putnam and contrary to that of Dr Foster, that:
Both of these conclusions, if justified, are important. The first implies that the risks of hepatitis were considered by commercial companies[2169] to be of a sufficient magnitude as to justify time, resource, and effort being put into research and development of methods that might reduce or eliminate it, no doubt at the expense of taking preference over other potential projects. It implies that it was not the threat of AIDS which stimulated research; it implies, too, that each of the six major pharmaceutical companies thought that it was a reasonable commercial bet that a result (whole or partial viral inactivation) might be achieved, and that this would be a result worth having. The protein chemists and scientists in each of those companies plainly did not share Dr Foster’s view for, if they had done so, none of these commercial companies would have decided to spend time and money on pursuing what they believed to be a hopeless quest. Though Dr Foster makes a case that Dr Putnam’s views are retrospective, the fact is that in the mid to late 1970s scientists directly involved in concentrate production contemporaneously thought that heat treatment might inactivate hepatitis viruses, and that it might be compatible with large scale production.
It is clear from the facts therefore that the first conclusion is justified.
So too is the second. The evidence for this is that each of the principal pharmaceutical companies – Behringwerke in Germany, Immuno in Austria, and Hyland, Cutter, Armour and Alpha in the US, each of whom produced their Factor 8 concentrates by slightly different methods (so it seems) – was able, independently of each other, as commercial secrecy dictated, to treat their concentrate products with heat in a way which they believed would eliminate or reduce hepatitis. There is some evidence that heat treatment indeed did reduce the risks of hepatitis, though as Dr Foster pointed out, all of the US products still remained capable of transmitting some non-A non-B Hepatitis infections. They had not eliminated the risk. More severe heat was necessary to do so: and to achieve this stabilisers and methods of production that suited that degree of heat had to be developed, without compromising the solubility of the final product so much that it became too difficult to use. The risk that commercial concentrates might transmit hepatitis was not effectively eliminated until the very end of the 1980s.
The fact that commercial concentrates reduced, but did not eliminate, the risks of viral hepatitis being transmitted does not mean that heat treating their products was worthless. Reduction of risk is a valid goal in itself. As the US Committee said: “In a crisis, decisionmakers may become so preoccupied with seeking solutions that will dramatically reduce danger that they will fail to implement solutions that are less effective but are likely to improve public safety to some degree. Partially effective risk-reducing improvements … can save lives, pending the development of more efficacious safety measures.”[2170]
The second finding – that heat treatment effective to reduce or eliminate viral transmission could have been effected before 1980 – leads to the question “why did it not happen?”. The answer to this question reached by the US Committee is necessarily specific to the US. Nonetheless, it is informative: “Treaters of hemophilia and Public Health Service agencies did not, for a variety of reasons, encourage the companies to develop heat treatment measures earlier. Strong incentives to maintain the status quo and a weak countervailing force concerned with blood product safety, combined to inhibit rapid development of heat-treated products by plasma fractionation companies.”[2171]
Whereas all of the six companies mentioned had begun work on viral inactivation by heat before the cause of AIDS being transmitted through blood products was appreciated, and thus focused initially on the risks of hepatitis, BPL in England began actively to work to inactivate viruses in Factor 8 and Factor 9 concentrates under the shadow of AIDS. Although it “started late”, although there were fears that the Factor 9 concentrate in particular – but also Factor 8 – might give rise to a greater risk of thrombosis from the heat-treated product, although research facilities were limited, scientific staff were few, and BPL suffered from a lack of viral containment equipment, and although initially the scientists involved were unable to test their products definitively because there was no test as yet for the virus or viruses they wished to eliminate, BPL nonetheless managed to develop a heat treatment effective against HIV in less than two years from starting active research and development. (It should be pointed out that BPL “lost” a couple of years before starting a research project to achieve this). It managed despite these limitations. It also managed to produce a product free of hepatitis. This took only a little longer but BPL managed that too within two years of starting research.[2172] PFC took some 18 months longer, so far as hepatitis was concerned, but as the above account demonstrates was able to produce (and distribute) a product which by reason of heat treatment was free of the risk of causing AIDS by 10 December 1984.
The overview expressed in the US Committee’s report that: “all of the product treatment methods that were ultimately proven to be effective in inactivating the hepatitis B and C viruses, and HIV, were developed within the laboratories of the plasma fractionators or by individuals closely associated with these industries. With the exception of Behringwerke, A.G., in Germany, each of the major plasma fractionators developed their inactivation methods at approximately the same time and entirely independently of each other”[2173]is entirely consistent with the evidence before this Inquiry.
This material shows that each of six major fractionators – Behringwerke, Immuno, Alpha, Armour, Cutter and Hyland – followed by two more in the UK, BPL and PFC – were able, each in their own way, independently, and within a relatively short period of time, to apply heat treatment in the course of manufacturing their concentrates without (except initially in the case of Behringwerke) sacrificing yield to such an extent as to render large scale commercial production lacking in viability.
There is evidence, principally from Dr Foster, that a number of technical developments over time helped to improve the processes. There is, however, no evidence that there was any sudden development in the mid to late 1970s that made it possible to heat treat factor concentrates when it had not reasonably been possible beforehand. There was no “watershed moment”. The essentials were finding a way of preventing the application of heat destroying the effect of the relevant coagulation factors whilst being sufficient to eliminate – or reduce – the risks of hepatitis. That meant finding the appropriate stabiliser and method of production. The track record of each of the pharmaceutical companies demonstrates that given some determined effort it was a matter of trial and error. There is no evidence that there was any technological impediment[2174] to this in the early 1970s that had to be overcome to enable what could not have been done before.
The reasons why heat treatment was not employed earlier to combat hepatitis and other viruses potentially in factor concentrates are a matter of inference. There are likely to have been a number. Some are general to both the US (so far as can be gleaned) and the UK.
There was considerable complacency. Thus in the US and the UK hepatitis was regarded as an inevitable consequence of treatment for haemophilia. One demonstration of this comes from February 1975 when Professor Bloom wrote to a local GP concerning a patient. He said “A small percentage of these freeze dried preparations contain, unavoidably, the virus of serum hepatitis and therefore potentially dangerous to the patient, his relatives etc.”[2175]The word “unavoidably” betrays an acceptance of the position, an acquiescence to the status quo.
There was clearly unease about hepatitis. But it seems likely that in the UK reliance was placed upon the low rate of infections in the community as a whole, and in the donor population in particular,[2176] as likely to protect patients from most of it. For some, it seems to have become an article of faith that a blood service which accepted donations only from voluntary non-remunerated donors would not be likely to manufacture blood products from those donations which would carry infection. Whereas it was absolutely right to place very considerable weight upon the importance of a voluntary system, it led in some to a disbelief that voluntary blood donation systems could ever transmit significant infection.[2177]
In the early 1970s efforts to inactivate hepatitis virus were probably also discouraged in the US by the hope that screening tests for Hepatitis B antigen, though imprecise in their first generation, might improve sufficiently to reduce the risk by enabling fractionators to discard plasma which tested infective.[2178] The extent to which this may have discouraged research may not have been as great as reliance on the voluntary donor system. In December 1973, Alter et al speaking in an article of the value of improved testing for Hepatitis B nonetheless concluded by saying “it is important to emphasize that the impact of HBAg testing on post-transfusion hepatitis is minimal when compared with the potential impact of eliminating the use of commercial blood. By far, the single most significant measure for the reduction of posttransfusion hepatitis is the total exclusion of the commercial donor.”[2179]
Later in the 1970s it was anticipated that a vaccine might become available against Hepatitis B, which led to the expectation that uninfected individuals and infants might be protected against it.[2180]
Next, the appreciation that the discovery of Hepatitis B was not the discovery of the cause of serum hepatitis, but only of part of what caused serum hepatitis, was slow: as described in the chapter on Hepatitis Risks 1970 and After. Appreciation of the prevalence and severity of non-A non-B Hepatitis developed slowly,[2181] though gathered pace in the second half of the 1970s. Further, plasma fractionators, government, the medical community and society as a whole did not seem to realise that new serious pathogens or latent dangers might also be present in untreated concentrate. The undisputed rhetoric was that the giving of blood was inherently risky, but there was insufficient attention to adopting the practical steps to reduce those risks that should logically have followed.
Finally, there was little commercial incentive to spend time and resources on inactivating a virus with which, in essence, consumers of the product had learnt to live, when the pharmaceutical companies were enjoying considerable success. It was only when growth in the market was perceived by those companies to have slowed down and be approaching saturation, and there were a number of calls from influential quarters to inactivate hepatitis in factor concentrates, that it seems to have been thought that some of the yield of Factor 8 and Factor 9 from the plasma supplied for fractionation might be sacrificed in order to make a safer – and potentially therefore more attractive commercial product. More intensive efforts at inactivation then began. These factors may help explain why Dr Shanbrom’s approaches to pharmaceutical companies in the early to mid 1970s were met with little interest and it was not until 1985 that he found a willing partner to develop and test his method. The commercial companies had to balance their interest in the good they might achieve by pushing the effectiveness to patients of their products further, and gaining competitive advantage, with their concerns over yield and cost. The pharmaceutical companies all began actively to develop heat treatment to inactivate viruses at about the same time in the late 1970s, when there was more of an imperative to improve market share.
Nor was there encouragement by the authorities which could have given it.
The US Institute of Medicine Committee report found the FDA gave little encouragement to the pharmaceutical industry to research methods of viral inactivation.[2182]
That viral inactivation did not take place earlier than it did in the UK, although it could have done, was in summary likeliest to have been because of a mixture of complacency, and an absence of encouragement by Government, by haemophilia centre directors, by the blood services in both England and Scotland, and by a system which had in effect surrendered control of whether treatment was virally inactivated to commercial suppliers (whose presence in the market was created by the absence of self-sufficiency). This was coupled with the view taken by those in charge of fractionation in the UK that to experiment would be futile because heat treatment had no prospect of working.[2183]
Just as the US Institute of Medicine Committee concluded, there had been little encouragement by the Public Health Service agencies in the US,[2184] little was done by governments in the UK.
There is no evidence of any significant funds being devoted to research into viral inactivation at BPL, whereas it should have been a priority. Dr Maycock, in his final report as director in 1978, made a point of saying that NBTS lacked a central research laboratory:
“DHSS, in order to be able to carry with confidence its responsibility for providing the transfusion service in England and Wales, should consider fostering the development of a central transfusion research laboratory. Without a basis of research and development, a modern effective transfusion service cannot be maintained. DHSS should, at least, ensure that the production work of BPL and PF Lab are supported by adequate research and development, for without this, production will tend to stagnate … It should be an accepted principle that research and development will not be sacrificed to growing demands for products.”[2185]
Factor 8 concentrate was produced mainly at Elstree (BPL). The production facilities at Elstree run by the financially struggling Lister Institute had been refurbished in 1965, and extended in 1972, but even then were cramped on a site which gave little room for expansion. A need to update them was recognised by their director from the start of the 1970s.[2186] They were, by 1978, outdated and in dire need of modernisation and improvement. This was at the same time as demand was increasing for it to produce Factor 8 (Factor 9 was made principally at Oxford during this period). The need for development was drawn to prominence by Dr Rosemary Biggs in 1967.[2187] These shortcomings were not only known to the director, but had been reported in public by mid 1974, when the British Medical Journal carried an editorial drawing attention not only to them but also asserting that the protein fractionation centres “now lack sufficient staff, accommodation, equipment and the basic organizational units to do the job.”[2188] The shortcomings were later to be confirmed authoritatively following inspections by the Medicines Inspectorate in 1979 and subsequent years.[2189] The need to remedy them required financial input. Research was left as a poor orphan.
In particular, although the origins of BPL lay in the research interests of the Lister Institute as well as the post-war organisation of blood supplies through the Medical Research Council, and its name contained the word “Laboratory”, as did PFL in Oxford,[2190] the facilities for research were so poor that the only place advanced research work on viruses could be carried out was at the Centre for Applied Medical Research at Porton Down, since it alone in England had the necessary containment facilities: it was not until the early 1980s that PFC in Liberton had its research facilities upgraded, consequent on improvement work which followed the upgrading of PFC such that it had a laboratory with more appropriate viral containment facilities. It is noteworthy that tests for viral presence in 8Y produced at BPL were then conducted at the PFC laboratory, because BPL did not itself have the facilities until after its own regrade had been completed.[2191]
Professor Savidge of St Thomas’ Hospital, a leading haemophilia consultant who practised at the time, subsequently attributed the failures to effect self-sufficiency and to eliminate viral contamination of plasma product to “poor leadership relying on the assumed safety of BPLs [sic] products and reluctance to endorse intensive research into [heat] inactivated products” and to a “lack of political will to spearhead these essential changes that were quite evident by 1978 for hepatitis.”[2192]
In conclusion, research into methods of viral inactivation to protect recipients of blood products from the dangers of hepatitis in the UK should have been encouraged, and funded adequately, by central government [2193] no later than the mid 1970s. Had this happened, it is reasonable to conclude that a heat-treated product likely to reduce the risk of hepatitis would have been available no later than 1980/81, and quite possibly earlier. Had it been, then – albeit by chance – the risk that any recipient would have suffered HIV infection would have been reduced almost to extinction, and the risks that a recipient might suffer hepatitis would have been significantly lessened. The necessary research did occur – but later. Viral inactivation happened. But it happened late. That is simply because the necessary research did not start early enough, when it could – and should – have done. It was not encouraged as it should have been. The facilities to conduct it were rudimentary and withering on the vine. Yet instead of taking steps to minimise the risks of viral infection, the authorities either organised (at BPL) or acquiesced in (in the DHSS) a rise in pool sizes which increased those very risks; and even when alerted to claims by commercial producers that their heat treatments might inactivate viruses still (at BPL/PFL in England) procrastinated before beginning serious development work.
This chapter examines the risks that arise from increased pool sizes for the production of concentrates, what was known and understood about those risks, and the extent to which pool sizes in the UK nonetheless increased. It also looks at the information regarding viral risks provided by BPL and PFC on the product labels for their products.
June 1944 paper presented to MRC Jaundice Committee recommends restricting the size of pools.
February 1945 Ministry of Health, MRC and others agree to use small pools; by 1951 the use of large pool plasma is abandoned.
1952 WHO Expert Committee on Hepatitis recommends control of pool size as a measure to reduce spread of serum hepatitis.
June 1954 Ministry of Health, MRC and Department of Health for Scotland study shows restricting the size of plasma pools greatly reduces the incidence of jaundice.
June 1973 BPL plans to move to pool size of 250 litres (1,250 donations).
1975 Dr Craske reports on the Bournemouth hepatitis outbreak and refers to the associated risk of using large pool concentrates.
1975- 1977 pool size used to make concentrates at BPL increases from 830 to 2,000 donations per pool.
1976- 1980 maximum pool size at BPL increases from 1,500 to 5,000 donations.
1981 capacity to accommodate larger pool sizes increases at PFC.
1983 maximum pool sizes at BPL increases to 7,500 donations; by 1985 10,000 donations.
Dr Rosemary Biggs director, Oxford Haemophilia Centre
Dr John Craske virologist, Public Health Laboratory Service
Dr William d’A Maycock consultant advisor to the CMO on blood transfusion and director, BPL (until 1978)
Dr Richard Lane director, BPL (1978 - 1990)
Dr Robert Perry director, PFC
Dr Terence Snape scientist in charge of quality control at PFL
Leon Vallet Lister Institute and BPL
BPL Blood Products Laboratory (Elstree)
PFC Protein Fractionation Centre (Edinburgh)
PFL Plasma Fractionation Laboratory (Oxford)
This chapter looks at one of the two most significant matters which determine whether plasma or a blood product made from plasma may transmit infection: the number of donors whose donations have contributed to the pool from which it is drawn. Although our mental picture of transfusion is the giving of single units of blood, each of which comes from one donor only, this chapter examines a very different picture. It is one of treatment not from single donor units of products, but from plasma or blood products taken out of pools in which several donations have been mixed. The chapter examines first the theoretical risks that arose from pooling, and whether that risk increased with the size of the pools used. It then asks whether (and when) any such risk was a real one, and was appreciated scientifically or by those who, in various capacities, were responsible for utilising those pools in the treatment of patients. It sets out the evidence of increases in pool sizes. It next considers whether those responsible for the administration of blood products in the UK knew or ought to have known of the risk, and if so what they did to reduce or eliminate it; or whether instead they tolerated it because any rise in the risk accompanying an increase in pool size was more than matched by an increase in the safety of those who were receiving the eventual product.
The chapter shows that – alarmingly – they were informed, took little notice, and instead of taking action to reduce the risks by reducing the number of donors whose plasma contributed to a single product or infusion, presided over an increase in the risk to levels which were more than 300 times higher than they had been at the start of the 1970s. The early 1970 pool sizes consisted of donations in numbers which had deliberately been avoided by the blood transfusion services for around 20 years as being too high for blood safety: but they then grew larger, exponentially, as charts drawn from the fullest available information as set out below will demonstrate.
The chapter will end with consideration of whether this surging rise in pool size in itself significantly increased the risk that people with bleeding disorders in the UK would suffer AIDS, hepatitis or other viral insults.
It has long been recognised that the risk of transmitting viral infection increases the more often a person receives blood from different donors. A transfusion of a single unit of blood may carry an infective particle or organism. The chances may strongly be that it will not. But if another transfusion, from another donor, is given, and yet another and so on, the risk that one of them will be infective begins to grow.
The frequency with which a single donation is infective will depend centrally upon who the donors are who are selected to donate it. If they come from an area in which there is (for instance) a low level of hepatitis, or in which there is less “risky behaviour” (such as the sharing of needles) the risk from their donations is also likely to be low. If they are paid for their blood, and use the money they are paid to secure their next fix of narcotics, or if they come from places which are recognised as having a high level of hepatitis (or latterly HIV) such as prisons, then, again, the risk run by receiving a donation they have given is itself higher.
In general, therefore, the risk of being infected with, for instance, hepatitis will depend upon the frequency with which donors with hepatitis contribute their blood for the purpose of transfusion, or to make a blood product. The risk cannot be ignored, but it is undoubtedly small where it reflects a low prevalence in the donor population. When plasma is taken from that blood for the purpose of making a single unit of cryoprecipitate there will be no more risk of infection from that single unit than there would be in receiving a transfusion of blood: it will be no higher than it is in the general donor population.
However, there may be good reasons to want to “pool” blood. It may provide a more efficient system of transporting plasma from place to place (eg in frozen packages). It may help a clinician better to gauge the dose to give to a patient if what is to be injected comes from at least a small pool. This is because it is known that where cryoprecipitate which comes from a single donation is to be used to replace a clotting factor which is missing from the recipient’s blood stream there will be uncertainty about the amount of clotting factor which it contains. The average level of clotting factor in the blood is given the figure 100%. Some people may have as much as 150% of this normative value: others, however, will have 50% or less. A clinician administering a unit of cryoprecipitate will thus be unsure how much Factor 8 activity it will contain. This can tend to overprescribing to ensure that the desired level of clotting factor is achieved. However, overprescribing can be avoided if rather than have single-donor cryoprecipitate, a small pool of, say, ten donations is used, for when taken together the difference in the factor levels of the individual donors tends to even out towards the 100%.
It was established by the mid 1950s that the potential infectivity of hepatitis viruses was high.[2194] As little as two hundredths of a millilitre was regarded as capable of transmitting infection. Roderick Murray, reporting in May 1955, showed that an exceptionally small amount of blood containing virus could be infective. He also quoted a study which showed infectivity at the rate of 4.0 x 10-5 ml, which “represents a very small amount of blood or plasma. So small in fact that the amount remaining on an instrument even after vigorous washing and meticulous cleansing might be infective.”[2195]
In short, any “dilution effect” resulting from mixing one infected donation along with several hundred donations which were not infective would be negligible.
As already described in the Report, it was well established by the end of the Second World War that serum hepatitis was transmissible by transfusion. On 20 June 1944 a paper was presented to the Medical Research Council (“MRC”) Jaundice Committee on Administrative and Field Aspects in which it was said:
“The observation that hepatitis may result from injection of homologous[2196] serum after a long interval has now been confirmed beyond doubt. At the present time transfusion with pooled dried serum appears to be the source of greatest anxiety although comparatively small quantities of this product have been used … The problem of serum jaundice is not only an immediate one but may become of increasing importance as the use of dried human serum in therapeutics is developed … by comparison with the estimated mortality of epidemic hepatitis fatalities from homologous serum jaundice have been disproportionately numerous … The long latent period of serum jaundice is a feature of special interest … There is a strong suspicion that the severity of hepatitis varies with different batches of serum. Some kill and others produce relatively mild disease. It is also probable that serum hepatitis occurs without jaundice and that some patients may remain ambulant and uncomplaining … Although radical measures for the control of serum jaundice must wait on further knowledge concerning the nature of the jaundice producing agent and how to remove it, much can be done in the way of prevention, without this knowledge, by:-
The paper went on to discuss the need to keep complete and continuous records so that the source of harmful material could be traced (enabling an effective lookback) and concluded “We should evolve a carefully prepared plan, and provide adequate facilities for it to be carried out.”[2198]
The probability is that this wartime paper reflected the battlefield use of large quantities of fresh frozen plasma. If frozen and freeze dried, it could easily be transported. To produce it in transportable quantities for battlefield use it was natural to use a number of donations pooled together. However the message that pool sizes should be restricted was taken up at the Ministry of Health in the following year, for in February 1945, representatives of the MRC Jaundice Committee and the Ministry of Health met and decided that the Cambridge drying plant should turn over to such small pools.[2199] On 5 April 1945 at a meeting between the MRC, the armed services, regional blood transfusion officers and blood supply depot directors this decision was confirmed.[2200]
Further commentators reinforced the need for caution as to the size of pools. Thus in September 1946, an article in the British Medical Journal urged that human serum for prophylactic purposes should not be pooled, and for transfusion purposes only small pools should be used. The article had a footnote which read: “We understand that only small pools are now used by the Ministry of Health for the preparation of blood products.”[2201] (This understanding was misplaced: for there is evidence that later that year Dr William d’A Maycock was taking steps to withdraw large pool plasma which had been in use until then in Liverpool).[2202] In 1947 a study of British Army medical records showed that troops who had received plasma suffered higher rates of jaundice than those who had received whole blood, and the cause was suspected to be the pooling of up to 500 donations in one plasma pool.[2203]
By 1951 the use of large pool plasma had been abandoned.[2204]
A Welsh example typifies this period. Dr Drummond, director of the Cardiff Regional Transfusion Centre, wrote to Dr Maycock in January 1950 saying that he could not justify the continued use of large pools when the prevalence of homologous serum jaundice was 10% compared to 1% for small pools. He added that if the case went to the law courts they would not look favourably, especially as it was practicable to make small pool plasma.[2205]
In the leading textbook on blood transfusion in clinical medicine Professor Patrick Mollison wrote in 1951:
“Lehane and others, (1949) have reported the following figures for the incidence of homologous serum jaundice: after whole blood, 0.8%; after transfusion of small-pool plasma, (derived from not more than ten donors), 1.3%; after large-pool plasma (derived from not less than 300 donors), 11.9%. The use of large-pool plasma has, of course, now been abandoned … even an incidence of about 1% is undesirable and it remains very important to find some method of killing the virus. Incidentally, the discovery of an effective agent would make it possible to revert to the more convenient practice of preparing large pools of plasma.”[2206]
By way of comment, this is an early example of the tension between convenience in preparation of a blood derivative, against the safety of that blood derivative once prepared. It shows the extent to which even within the economic constraints of the post-war economy convenience yielded to safety. It was entirely right that it should. The contrast with what was to happen during the 1970s and early 1980s is made all the more stark by the use of the words “of course” dealing with the obvious need to stop using large pool plasma.
When in late 1952 the Expert Committee on Hepatitis of the World Health Organization made recommendations of methods that should be adopted to reduce the risk of transmitting hepatitis, in a document which was contributed to by UK clinicians, it urged amongst other methods of reducing the spread of serum hepatitis that there should be control of pool size.[2207]
By 1954 it was indeed now plain that large pool sizes had been abandoned in favour of small pool sizes, and that this had had a beneficial effect. The Ministry of Health, the MRC and the Department of Health for Scotland organised surveys which were carried out by regional transfusion directors in Cardiff, Glasgow and the West of Scotland, Liverpool and Manchester, and contributed to by Dr Maycock and Leon Vallet of the Lister Institute (which ran the Elstree plant until 1978). Their report confirmed that restriction of the size of a plasma pool greatly reduced the incidence of homologous serum jaundice arising from it, and that the risk of such a complication after receiving a transfusion from small pool plasma was little greater than that attaching to whole blood.[2208]
Factor concentrates were first made in the mid 1950s[2209] and led to increasing pool sizes. These were however small. Although no commentator in the 1960s denied the view that increasing pool sizes came with some additional risk, there were differing views about quite how great an addition to the risk this was, and how significant it might be for a patient’s health. Some discounted the risk; others strove to avoid it.
By the 1960s, preparations which concentrated Factor 9, for use in treatment, began to be made in Oxford using precipitate from Elstree: a document recording the preparation and use in two patients of product prepared from the precipitate of “45 to 50 litres of plasma” was published. 45-50 litres of plasma equates, roughly, to the plasma from 225-250 donors.[2210]
By 1963 pools used to prepare antihemophilic factor (“AHF”), as such preparations of Factor 8 were then known, were 14-22 litres in size. This amounted to the use of pools made from a maximum of 90-110 donations. There were said to be no “contra-indications to the prolonged or repeated use of the product.”[2211]
However, later that year Dr Peter Wolf at Lewisham Hospital, where AHF was produced for use from three litres of plasma[2212] commented “The risk of contamination of blood with the virus of infective hepatitis limits a single fractionation batch to a donor pool of 50” but “Human A.H.F. concentrate, produced in this way at multiple centres throughout the country, could provide sufficient to treat all the known classical haemophiliacs in Great Britain”.[2213]
In February 1964, Dr Maycock and Leon Vallet, of Elstree, proposed to “retain the present pool size (30L) because of the risk of transmitting serum hepatitis.”[2214] But even that carried some risk, as appeared the following month when a working party on human antihaemophilic globulin decided “As the HAHG [human antihaemophilic globulin] concentrate prepared from plasma pools of up to 30-40 litres in volume apparently carried a risk of transmitting serum hepatitis, it was considered inadvisable, when planning increased production, to increase the plasma pool volume much above this size, unless further observations indicated that the risk was smaller than the present series of cases suggested.”[2215]
Despite having been a party to the report of the working party, Dr Maycock wrote less than three months later to say that in the UK antihaemophilic globulin (“AHG”) was made from 60-100 donor pools, and described a “paucity of reports of hepatitis” associated with this.[2216]
In 1965, Dr Jean Grant of the Oxford Regional Transfusion Centre recorded in her “Complications of Transfusion” that “It has been found that a minute fraction of a millilitre of virus-laden blood was enough to cause hepatitis (Murray, 1955) and it was for this reason that the production of large-pool plasma, made from the contributions of more than 300 donors, was abandoned in favour of limited pools derived from not more than ten donors.”[2217]
At the end of 1965 Dr Robert Cumming and colleagues, from the Edinburgh Transfusion Centre and Blood Products Unit, described preparing AHF (an early form of what has become known as factor concentrate) from small pools consisting of six donations. They commented “Because of the risk of transmitting serum hepatitis, small-pool operation is preferable, in preparing antihaemophilic fractions. The simplicity of the procedure described is thus an advantage in large-scale production.”[2218]
Thus far, the story had been one of blood transfusion services, and those who were pioneering the gradual development of factor concentrates, drawing back from using larger pools despite the convenience that might bring. They were concerned about increasing the risk of infection by increasing the size of the pools used, although there was some uncertainty about the extent to which risk was increased by increasing pool size.
In 1967 pressure grew for an increase in the pool sizes used to make AHF. There was a meeting of a working party on the use of the cryoprecipitate method.[2219] Dr Rosemary Biggs had in mind estimating the amount of Factor 8 concentrate that would be needed as AHG, and had spoken to Dr Maycock in advance of the meeting. She wrote to the MRC in advance, to say that he “also thought that we should probably consider the question of serum hepatitis and, in view of the American activities, whether or not it would be reasonable to increase the pool size for fractionation.”[2220] The expression “American activities” is probably a reference to the large pool fractionation methods starting to be used commercially by US pharmaceutical companies to produce factor concentrates.[2221]
By contrast, in early 1968 work had already begun on the expansion of the blood products unit in Edinburgh. One of the products it would make would be factor concentrate. Dr Cumming briefed Dr Maycock and Leon Vallet on the pool sizes he had in mind:
“Dr Cumming explained that, after consultation with clinicians using this material, it was decided that Edinburgh should use a pool of 8 litres. The clinical opinion in Edinburgh was that a pool of this size was sensible for general use but that larger pools could be used for major surgery where large quantities were required for one patient. It was explained that in the Edinburgh Blood Products Unit it had been decided that a pool of 8 litres could be handled conveniently and quickly. Production plans had been established on this basis to process ultimately 1,000 litres of fresh or fresh frozen plasma weekly.”[2222]
Eight litres is equivalent of roughly 40 donors.
What we see is that at the start of the 1970s there were the same two broad strands of opinion – one tending to regard the additional risks as minimal, the other taking a more cautious approach – whilst there was a growing sense that the UK might need to move towards matching the US practice of using large pools if manufacturing was to be efficient in producing the largest volumes of product in the shortest period of time.
At the end of the 1960s and start of the 1970s Factor 8 and Factor 9 were being made at the Plasma Fractionation Laboratory (“PFL”) Oxford. The number of donations in the mean pool size for Factor 8 in 1969 was 160 donations: in 1970 192 and the same in 1971.[2223] So far as Factor 9 was concerned, larger pools were used: in 1969, 439 donations was the average, in 1970 it was 384, and in 1971, 300.[2224] Thus, at the start of the 1970s, so far as National Health Service (“NHS”) plasma was concerned, pool sizes were larger than had been accepted in and since the early 1950s, but were still relatively small in scale compared to what was yet to come, and compared to those in use in the US for making blood products commercially.
By 1970 there were authoritative warnings of the desirability of limiting the exposures of patients to blood and blood products so far as practicable. Professor Garrott Allen had written that the risk of serum hepatitis (which he described as a serious clinical problem) from transfusions derived from prison and skid row populations was at least ten times that from the use of volunteer donors. He was speaking of the United States: but ended up by saying the most practical method of reducing the hazard of serum hepatitis from blood was “to limit the use of blood by giving one transfusion instead of two, two instead of three, etc, and especially by excluding, if possible, all prison and Skid Row donors.”[2225] Though he was speaking of transfusions of blood, rather than infusions of blood products, what he said would suggest that pooling to make the latter should be limited. On Professor Garrott Allen’s approach, drawing an injection of Factor 8 concentrate from the pools by then in use at BPL would have the same effect as giving a hundred or more transfusions instead of one. Dr Carol Kasper and Dr Shelly Kipnis in their letter published in 1972 considered the risks of taking blood products prepared from pooled plasma more directly, when they wrote that for older children and adults who had had little exposure to blood products, especially those with mild haemophilia, “single-donor products are preferable.”[2226]
In mid 1972, in a report later published in 1973, Dr Biggs wrote about the risks of hepatitis from using pools of the sizes from which her products came. She began:
“About 1 in 800 donors is a carrier of hepatitis B antigen. The larger the number of donors concerned in the preparation of concentrate the greater the risk of exposing the recipient to material containing hepatitis B antigen. The use of freeze-dried concentrate, which is made of pools of 200 donors (or even higher numbers for commercial material) must carry a higher risk than single donations. But there is the possibility that the development of jaundice may be dose related and that single infected bottles may be more dangerous to the individual patient than pooled material in which the virus is diluted. Despite this the frequency of hepatitis in severely affected patients does not seem to increase significantly with increased use of freeze-dried concentrates.”
She went on to say “An exception to this rule concerns the mildly affected patients to whom very little treatment is given. These patients do seem to have a high incidence of hepatitis if large pool fractions are used.”[2227]
What she does not say is that the risk was lower with concentrates than it was with single donor cryoprecipitate. There were both theoretical reasons why it was higher, and experience which plainly confirmed that it was – indeed, Dr Biggs’ use of the phrase “does not seem to increase significantly” suggests there was some increase, albeit it, in her judgement, was not “significant”.
By March 1973 the die was cast. In that month, the Expert Group on the Treatment of Haemophilia – only, as it happens, considering Hepatitis B – repeated what Dr Biggs had said. She was a member of the working party. It noted that in practice:
“studies in several centres have shown that the incidence of hepatitis among severely affected patients who have been treated with the freeze-dried preparation is not very much higher than that at centres not using freeze-dried concentrate and this suggests that the development of hepatitis in these multi-transfused patients may be dose-related. It was agreed that the theoretically increased risk of acquiring hepatitis (which does not seem to be borne out in practice)[2228] should not be a deterrent to using the freeze-dried preparation and in any case this complication will decrease with universal screening of donors for hepatitis antigen.”[2229]
In the same month, Scotland began planning to produce high purity Factor 8 concentrates, with a planned production capacity for the new Protein Fractionation Centre (“PFC”) of one pool of 200 litres per week.[2230]
By June 1973 BPL had plans to move to a pool size of 250 litres (thus some 1,250 donations). There was no discussion in advance of this about the increased viral risks from increasing pool sizes.[2231] The risks were nonetheless widely appreciated: for instance, it was in 1973 that Dr Duncan Thomas, as a senior medical officer in the Department of Health and Social Security (“DHSS”), when advising on the application for a licence in respect of Hemofil noted his concern that the larger pools used in making the American product carried with them an increased risk of hepatitis from the product.[2232]
By 1975 the pools which were in use to make NHS concentrates at BPL contained 830 donations. They were to rise to 2,000 by 1977.[2233] By 1975, however, other events were showing that larger pools could be particularly harmful, in part because they were larger. Dr John Craske reported then on the outbreak of hepatitis in Bournemouth, and referred to the risk of using large pool concentrates which he considered was associated with the outbreak: “The risk is greatly increased with factor-VIII concentrates prepared from pools of more than a thousand donations.”[2234] At a meeting of the UK Haemophilia Centre Directors’ Organisation (“UKHCDO”) in September 1975 Dr Maycock accepted that all infected batches would not be excluded since the test would not pick up all levels of Hepatitis B virus. He acknowledged too that some hepatitis was caused by viruses not detected by the test. (He referred, in effect, to non-A non-B Hepatitis.)[2235]
It was clear then, as it was clear more generally,[2236] that large pool sizes came with an increased risk of causing hepatitis. Though the theoretical risk of hepatitis was greatest for those who had been little treated, had mild haemophilia, or were children, by the mid 1970s no-one had suggested, and no-one was suggesting, that an increase in pool size did not mean an increase in risk. Lord David Owen accepted in his evidence to the Inquiry that he knew this when Minister of State for Health.[2237] The view of Dr Biggs, expressed in her article and through the working party in which she was prominent, that the increase in risk was only modest was based upon her study of pool sizes which had a mean size of 190 donations.[2238] The change in 1976 was to a pool more than six times as large. Dr Biggs’ conclusion in her 1973 study (of infections from 1969-1971) could not simply be applied as if, whatever the size of pool in 1976, there would be no significant risk from the increase in the number of donations to it. Dr Biggs herself accepted that “volunteer donors and small pool fractionation methods will result in the safest plasma fractions.”[2239]
There can be no substantial doubt that an increase in pool size led to an increase in the number of infections that occurred in people who were given injections or infusions from these larger batches.
Since hepatitis was regarded in the 1970s as a significant complication of treatment for haemophilia and since it caused the concern it did then and in the 1980s, there can be only one answer to this question: “Yes”. The increase in pool size, as set out above, was known or believed to increase the risk. The studies which have been mentioned involved in most cases observers or participants who came from the DHSS; and a substantial number involved Dr Maycock who was a consultant adviser on transfusion to the Chief Medical Officer (“CMO”). Moreover, those who read the medical press would be aware of the risk; the Licensing Authority was aware of the risk;[2240] and haemophilia centre directors were aware of it too. In the UKHCDO meeting, for instance, of September 1975 there were in attendance centre directors from each of the four home nations, as well as Dr John Cash of the Scottish National Blood Transfusion Service (“SNBTS”), Dr Craske of the Public Health Laboratory Service, Dr Maycock, Dr Terence Snape of PFL Oxford, Dr Sheila Waiter from the DHSS, and Reverend Alan Tanner from the Haemophilia Society.[2241] In short, the fact that an increase in pool sizes led to an increase in risk was known to those who prescribed the products, those who were concerned with public health, and those who were administrators.[2242] When the production facilities in the UK accepted that they should observe the same regulatory regime as the commercial suppliers did, the regulator was notified of any increase in the maximum pool size.[2243] Labelling, dealt with below, was subject to regulatory oversight. Labels had to contain the maximum pool size permitted. The regulator[2244] was in practical terms the DHSS. In short, if the DHSS did not in fact “know” of the pool size increases it was given the information it needed to do so.
The evidence of the actual pool sizes used at BPL has to be pieced together from different sets of data. This is set out in Figure 1 below. To understand what it shows, some explanation of the different data sets is necessary.
First, from the mid 1970s BPL product labels recorded the maximum number of donations that would have contributed to the pool from which a product was made. In March 1976 the maximum pool size was 1,500 donations.[2245] That increased to 5,000 donations by 11 September 1980,[2246] 7,500 donations by 1983,[2247] and it was 10,000 in March 1985.[2248] It follows that the pools used to manufacture Factor 8 concentrate in 1983 could be almost 40 times as large as the number of donations used to treat patients at Oxford in 1971.[2249]
Second, correspondence between fractionators and others which refers to pool size gives the snapshot of the view of the writer at the time as to the size of the pool that was being used. These snapshots are broadly consistent with the picture given by the maxima set out on product labels, although they show that it was in January 1982, at least, that 7,500 donations per bottle started to be in use.[2250] They also record a figure of 25,000 donations in June 1986 (although this was after heat treatment had been introduced, and hence it was at a time when viral inactivation might reasonably have been thought to have been achieved, even though the definitive studies on hepatitis transmission had not yet shown conclusively that 8Y was free of transmitting such a virus).[2251]
A “maximum” pool size does not mean that pools were in fact manufactured to take full use of that limit. Accordingly, as a third source, the Inquiry examined data provided by Dr Snape. He set out the number of donations contained in specific batches of Factor 8 manufactured at BPL between 1975 and 1989 (“specific batch data”). His estimate of the number of donations in a batch in 1975 was 750. The number of donations rose, on his evidence, to 6,000 donations from 1982 to 1985.[2252] This was eight times the number of donations used in 1975, and more than 30 times as much as Dr Biggs recorded for Oxford in relation to 1971.[2253]
The fourth set of data derives from batch history. The batch history does not show the date on which each batch was issued, and for this reason the data presented uses an approximate pool size for each year, rather than identifying a particular pool size used on a specific date. The batch histories show an increase from 1978 (when batch histories begin) to 1986. They rose from 2,250 donations in a batch to 6,000.[2254]
The documents from which the data derive use a variety of metrics to express pool size. Most documents give the number of donations assumed, whereas others give the volume of blood in litres or the weight in kilograms. Where the latter occurs, and there is no reference to the number of donations assumed, it has been assumed that the UK plasma donations were typically 180ml in size, rather than 200ml to which they are often rounded up. This is because the amount of plasma recovered in different regional centres varied.[2255] Both Dr Snape and Dr Richard Lane used slightly higher figures: Dr Snape used the rounded up 200ml and Dr Lane, in 1983, used a conversion figure of 190ml.[2256]
From 1984 onward, considerably more plasma was removed from whole blood donations where SAG-M was used: accordingly, there would have been fewer donations per litre.
It is to be stressed that the calculations are only estimates, and cannot be relied upon for point accuracy. However, the true figure will be close to the estimate, and the figures used are indicative of what is likely to be a broadly accurate conclusion.
Where records are drawn from a range of pool sizes used to manufacture NHS factor concentrates (without distinction between the concentrate concerned) the larger pool sizes are included and the smaller pool size omitted. If a report gives a minimum pool size which may have been exceeded on occasion, that figure is used because it is the only figure provided.
Contemporary reports starting first in December 1975 go from 830 donations then to 5,000 donations by 1 September 1980: that is a sixfold increase. If the starting point is taken from the average pool sizes described between 1969 and 1971, it is more than twenty-fold.

The figure speaks for itself as to the scale of the increase in pool size, and with it an increase in the risks of hepatitis and HIV.
There is no evidence that ministers, or the CMO, were alerted to the dramatic increase in the size of pools.[2258] Nor is there evidence that there were discussions at a high level in the Civil Service about the size of pools from which products were manufactured.
Part of the reason for self-sufficiency was to reduce the risk that hepatitis would be transferred by blood products. Accordingly, it is particularly surprising that there is no record of any of the consultant advisers to the CMO in the 1970s and 1980s – first Dr Maycock, then Dr Geoffrey Tovey, and next Dr Harold Gunson – alerting a senior civil servant, or the CMO to what was happening within the UK that increased risk rather than reduced it.
It is unlikely they did not know. Dr Maycock certainly did, though his successors did not have the same oversight of BPL as he did.[2259] If they did not actually know, they certainly should have done. This is because the desire to use domestic products rather than commercial ones arose in part not only because the latter were seen as the product of paid donations, and therefore seen to carry a greater intrinsic risk, but also because of the much larger pool sizes they were produced from.
If they knew, they should have alerted the CMO: and given the exponential rise in risk from the rapid growth in pool sizes it would have been surprising if the CMO did not in turn alert ministers. In short, ministers should have heard of the increase, and be told why it mattered.
Estimates of the additional risk created by paid donations mixed in commercial pools in the US suggested that products made from those pools were ten times more likely to transmit hepatitis than if unremunerated voluntary donations had been used, simply by reason of the source of the plasma used.[2260] This was (rightly) regarded as a strong reason to avoid continuing to use commercial products – irrespective of the impact of pool sizes.
These estimates were given well before the increases in domestic pool size which occurred in 1975. Yet they could not properly be assigned to past history and ignored, for in February 1975 Professor Garrot Allen wrote to Dr Maycock to say: “it does not take much commercial blood in a mixed combination to bring up an astounding attack rate from one that is relatively unnoticed. This is the basis of my concern about Britain purchasing commercial blood products from our country.”[2261] Dr Maycock therefore knew; possibly Dr Owen knew of this too;[2262] but there is little evidence that anything was done to control UK pool sizes, or to raise the issue with ministers.
In August 1975 Dr Craske linked the risks of commercial concentrates from large pools with domestic production when he wrote that the risk of hepatitis was “greatly increased with factor-VIII concentrates prepared from pools of more than a thousand donations. When blood for transfusion is prepared from commercial donations this increases the frequency of jaundice three to ninefold for single transfusions. The pool size, however, may be critical in factor-VIII concentrates, since transfusion hepatitis is a known hazard with large-pool products prepared from volunteer donors in the UK.”[2263] The substance of this undoubtedly came to the attention of Dr Owen.[2264]
By 1980, when pool sizes at BPL were still increasing year on year, and had reached multiples of the risks as they had been at the start of the 1970s, an international symposium on hepatitis from blood products was held. It was written up by each contributor in Vox Sanguinis, a publication particularly read by fractionators and transfusionists. Professor Manucci was one such contributor. He pointed out that strict adherence to the “small pool concept” in Sweden had given rise to “a very low incidence” of post-transfusion hepatitis in people with Haemophilia B, and suggested that the adoption of such a concept would be “a significant step forward in the prevention of posttransfusion hepatitis and liver disease in hemophiliacs.”[2265]
The Council of Europe recommended that blood collection agencies and pharmaceutical companies should give treating physicians and consumers[2266] detailed information about blood and blood related products, including the nature of the donor pool from which the products were derived.[2267]
The Council of Europe recommendation was adopted by the Committee of Ministers on 30 April 1980. The DHSS was thus aware of it. That December, Dr Diana Walford would put it on the agenda for the first meeting of the Advisory Committee on the NBTS.[2268] Yet, in September 1980 Dr James Smith at PFL asked Dr Lane, as the director of BPL, to agree to his, Dr Smith’s, increasing the pool size used to 900-1,000kg of plasma (roughly 4,500-5,000 donations).[2269]
Dr Lane observed “I am sure that once one has exceeded the 100 - 200 kg pool-size, one has already exceeded any possibility of small pool protection. I have discussed this with John Craske recently and he agrees exactly on this point.”[2270] The Inquiry has found no documentary evidence of this comment which Dr Lane purported to recall. There is, however, a record of a view which Dr Craske expressed the day after Dr Lane wrote this comment to Dr Smith. This comes from the minutes of a meeting of the Hepatitis Working Party of the UKHCDO directors held on that day. It reads: “Large pool concentrates appeared to give a higher risk of hepatitis than small pooled concentrates and Dr. Craske felt that increased usage of small pooled concentrates would help to reduce the incidence of hepatitis in the haemophilic population.”[2271]
Whereas Dr Lane was using whatever Dr Craske may have said to support an increase in pool size any implication (such as appears from the way his letter is worded) that pools could safely be expanded does not, on this evidence, faithfully represent the views of Dr Craske. At best the reconciliation of Dr Lane’s recollection of what he said and the record from the working party is that there was a desire for reasons of safety to use smaller pools, but a resigned acceptance that the increase in pool sizes had by this stage already gone too far.
The exchange between Drs Lane and Smith in September and Dr Craske’s recorded contribution to the Hepatitis Working Party are not the last word on this particular exchange of views. Just over two weeks later Dr Smith sent a memo to Dr Lane, in which he suggested that three tables in a report of Dr Craske which he had presented to the working party “offer good ammunition against the importation of U.S. plasma or its products”. He saw arguments about how these tables might be interpreted but ended up drily observing, in respect of the argument that most people with haemophilia may already have been exposed to the virus (with the implication that it did not matter if they were exposed again), that he (Dr Smith) would have thought that one attack was better than two.[2272]
The evidence thus establishes that Dr Smith was uncomfortable with the use of commercial products, and that was linked to the pool sizes used. It establishes also that Dr Lane and Dr Maycock before him were aware that increasing the pool size increased the risk of hepatitis transmission but decided to do so nonetheless. It establishes that clinicians too knew of the increasing risk with increasing pool sizes. But it does not show clear evidence, despite these various events, that the DHSS saw the issue of pool sizes as one on which it should take some action.
The DHSS was probably aware of the way in which the risk of hepatitis was being significantly increased. If it was not, it ought to have been. There is no evidence that the DHSS briefed a minister as to the increase in pool sizes. There is some evidence that individuals – Dr Owen, for instance – were aware that there was a link between pool size and infection; and considerable material to show that many attributed the apparent greater infectivity of commercial concentrates to the much larger pool sizes from which they were prepared. There is no evidence of any discussion about what best could be done to secure smaller pools, or even to neutralise the worst effects of the very considerable increase there had been in pool sizes.
There is less data available to determine pool sizes in Scotland. They were not identical to those in England at BPL: the method of production was different. The Scottish system was designed for continuous 24-hour operation.
In 1973, as the new building at PFC was nearing start-up, a production capacity of one pool of 200 litres per week was planned. John Watt explained: “This was deliberately chosen to meet a projected need to process 50,000 donations of plasma p.a. [per annum] to meet Scottish needs for this product … It has been intended that the 200 litre batch size would continue through the commissioning period and that the frequency of one per week would satisfy Scottish need.”[2273]
That persisted (at around 190 litres) until early 1980 when a review was undertaken by Dr Peter Foster and Ida Dickson, who was an experienced technician. They considered that losses in Factor 8 from having to meet quality control requirements could be reduced: in conclusion “the mean plasma volume per lot … for continuous thawing has been about 190 litres, giving Q.C. [Quality Control] losses of … 11% ... for a 40 ml fill. This loss would be reduced to about 4% if the plasma pool size could be increased to give at least 500 vials of concentrate per lot. This will probably be possible once the design of the continuous plasma thawing system has been completed.”[2274]
With an increase in perceived demand, and a new-scale thawing tank becoming ready for use at the start of 1981, it was seen that the maximum pool size for crushing and thawing could increase to around 700 to 800 litres of plasma per day within standard working hours, but a serious limiting factor was the freeze-drying capability, which at that stage could not match such output. There were two freeze dryers. One was limited to the product from a plasma pool of 300kg, the other to 500kg. Greater capacity was achieved for the latter by reducing the size of the bottles, which meant that more bottles could be accommodated by adding racks within the freeze dryer, bringing capacity up to 700kg – approximately, therefore, 2,800 donations.[2275] However, it seems unlikely that pool sizes of this magnitude were ever used. When the Inquiry examined tables of batches and the pool size from which they were made in the period 1978-84 they found that of 27 batches listed only 10 were larger than 300 litres, and of these the highest figure was 555 litres (5 such batches).[2276]
Other contemporaneous sources are consistent with this. They show pool sizes ranging from a minimum of 800 donations (200kg) to 2,200 (550kg). The pool size tended to vary depending on whether the smaller or the larger freeze dryer was to be used.[2277]
Further gradual increase occurred. When in late 1984, patients from Edinburgh – the “Edinburgh cohort” – were identified as having been infected with HTLV-3 through the use of PFC products it seems that 4,000 donors had contributed to the implicated batch, an increase of around 25% from the pools recorded up to 1983.[2278] In 1985, Dr Foster and Alan Dickson recorded that pool sizes for continuous thawing were then between 600kg and 1,000kg, depending upon the size of freeze dryer available.[2279]
The increases are shown in Figure 2 below.

The answer is – none. Instead of the risk being reduced, it was increased.
There are two exceptions to this general statement. First is to recognise that there was an experiment with small pool freeze-dried cryoprecipitate in the West of Scotland, which was not a success, for reasons explored in the chapter on Self-Sufficiency. Second, PFL produced a small number of batches from limited donor pools using plasma from a small number of plasmapheresis donors.[2281]
The exchange between Dr Lane and Dr Smith might well be accurate in showing that by the time it occurred pool sizes had grown so large that the risk of pools conveying hepatitis was very high, and to reduce the risk would involve a very significant reduction in the size of pools. It might not have been easy to develop a different, safer method of production, especially with the equipment then in use, and planning for a development of new premises designed to achieve self-sufficiency in part by large-scale fractionation.
Thus, in the space of ten years, a risk, which was only a little higher than the risks arising from a single transfusion,[2282] had risen very significantly. Pools had grown so large that the risk was almost an inevitability.[2283] If this was to have been avoided, the increase in pool size needed to have been (and should have been) arrested earlier in the process.
What had happened demonstrated that a system of using much smaller pools would have had to replace the existing system. That was never likely to happen, as a practical matter, in the early 1980s[2284] – the real vice lay in allowing matters to go that far.
This chapter has concerned itself with UK production. There may have been a desire to ensure the continued viability of BPL in a world dominated by commercial concentrates which had the economies of large scale, utilising much larger pools of plasma. Although this chapter is concerned with UK pool sizes, and evidences a conclusion that they had grown too large, creating too great a risk, the chilling effects of allowing pools of plasma from which products were made to grow too large is demonstrated by a particular episode which happened in the US.
On 19 July 1983 consideration was being given in the US as to whether to require the recall of batches of product made from a pool to which it was discovered a donor subsequently found to have AIDS had contributed. Dr Michael Rodell, a vice president of Armour, spoke in relation to this at an open meeting of the Blood Products Advisory Committee of the Centre for Biologics Evaluations and Research, a standing committee which advised the US Secretary of State and the Food and Drug Administration. He is recorded as having said that on average, persons who were paid for their plasma had it collected from them between 40 and 60 times per year. At that rate and given the pool sizes used in the US, four infected persons could contaminate “the entire world supply of Factor VIII”.[2285]
This explanation was not given in order to condemn the practice, and point out the dangers of the exposure of patients to the cause of AIDS, but to put forward an argument for the pharmaceutical industry against recall being obligatory. His point was that if a donor was subsequently found to have AIDS, and the viral cause of this might have come into products made from the pool to which he had contributed, then it would not just be one pool. The AIDS sufferer’s donations could easily be represented in as many as 50 plasma pools in one year. Up to 250 million international units of Factor 8 activity could be affected, all in various stages of pooling, production and distribution.[2286] Accordingly, the potential for serious disruption of supply was quite real. If those products were recalled, there would be a crisis of supply which would mean people with bleeding disorders would be left untreated,[2287] with all the consequences that entailed. In other words the need to continue supplying a product trumped any question of whether it was safe or (in effect) potentially a poison.
The implications of allowing production pools to become too big, in effect prioritising convenience of production over the interests of better patient safety, meant that it would become exceptionally difficult to achieve the latter – unless, as happened eventually, relatively accurate testing of donations and viral inactivation techniques developed, to save the day. But they did not arrive in time to prevent dreadful consequences from the use of large pool concentrates.
It was understood at the start of the 1970s that pool sizes mattered. The smaller the pool size, the less likely it would be that hepatitis would follow. It was understood that the risks that commercial blood products from the US would transmit hepatitis were much higher than those posed by NHS products for two reasons – the higher prevalence of hepatitis amongst donors, and the much higher pool sizes used to produce them. The risk is not additive: it is multiplicative. Only a few moments of reflection are needed to realise that, from a safety point of view, the last thing policy should have aimed to do was to copy commercial products by aping the pool sizes used by commercial companies. Doing this was to copy over into the UK the risks apparent in the US. Yet copying US production methods by using ever-increasing pools was what was done.
From a manufacturing point of view, ignoring the need to produce a safeproduct, it was more efficient to have larger pools. Greater efficiency however is not the same as greater safety.
Given comments made by haemophilia centre directors from time to time, haemophilia clinicians had at least an impression of the number of donations there would be in a pool used to make products at BPL, PFL and PFC.[2288] They could compare this with the information they had about the pool sizes used in pharmaceutical manufacture.
At PFL, labels were generated or overprinted by quality control “even up to 1982”;[2289] labels at BPL, being larger, were prepared by a commercial press. What was written on them was determined by BPL in consultation with the Medicines Division of the DHSS and later the Medicines Control Agency.[2290] Dr Snape’s evidence was that the labels were intended for both patient and clinician. They contained statements as to the maximum pool size (eg “Less than 7,500 plasma donations were used in the preparation of this batch”), and some indication as to risk (“The preparation is of human origin and cannot be assumed to be free of hepatitis virus”).[2291] There was no warning as to the risk specifically of AIDS until late 1985, and then on vials of 8Y, a product which was heat-treated.[2292] By 1987 the reference to donor numbers had been removed from the label; a conscious decision was taken to remove it and Dr Snape’s evidence was that: “Certainly once we reached the 10,000-donation limit, it was hardly relevant or hardly helpful to physicians or patients.”[2293]
In Scotland, when PFC applied for a product licence for its Factor 8 product the warnings it undertook to give were aimed predominantly at doctors, though Dr Robert Perry commented that where patients were on home therapy the products would have been supplied together with the product leaflets and “many of them may well have read it. But I think the precise warning was prescribed by the requirement [of the licensing authority] to satisfy the professional requirements for the product, rather than the individual patients.”[2294] In 1978 there was a warning for Factor 8 that “Product may carry the risks of transmitting serum hepatitis”;[2295] and for Factor 9 that “none of these tests are of sufficient sensitivity to eliminate the possibility of transmitting hepatitis ... the risk of transmission cannot be disregarded.”[2296]
The slow evolution of labelling is shown by the vial labels used in the mid 1980s: in 1984 it was “This preparation is of human origin and cannot be assumed free of hepatitis virus” (for unheated Factor 8 concentrate); and the same wording was used for unheated Factor 9 concentrate. By 1985 it was “The freeze dried product has been heat treated but cannot be assumed to be non-infective” (for heat-treated Factor 8 concentrate with the label dated 1985).[2297] Nothing was said about AIDS or HIV specifically.[2298]
The outer packaging was not much more informative: “This preparation is of human origin and despite careful screening of donations cannot be assumed to be free of hepatitis virus” in the case of unheated Factor 8 concentrate.[2299] Dr Perry in evidence commented that the leaflets were primarily targeted at the prescribing doctor “and, in a sense, they had a much closer working knowledge of risks of hepatitis non-A, non-B, hepatitis B and, latterly, HIV than the manufacturer of the products. So none of this information would have been a surprise to a treating doctor.”[2300]
The pool size was required by the 1973 British Pharmacopoeia: “the number of donations in the pool from which the preparation was obtained”.[2301] Between 1973 and 1978 the requirement for a label to identify the pool size disappeared from the British Pharmacopoeia requirements, to be replaced by a warning at least in terms that “the preparation is of human origin and cannot be assumed to be free of hepatitis virus”.[2302]
Three matters of comment arise out of Dr Perry’s evidence. First, from his perspective (which was not that of a clinician, though obviously someone in close contact with those clinicians who used PFC products professionally) PFC assumed that clinicians would spell out risks to patients and that may explain why PFC did not emphasise those risks.[2303] Second, he thought that the regulatory authorities would not have looked kindly on PFC, or any manufacturer, alerting users to a risk of infection from their products without evidence that that was so, and for this reason if in 1983 or 1984 PFC had given the warning in its product leaflets that “this product may transmit” AIDS, the regulatory authorities would have come back and asked for evidence, and “at that stage there was no evidence.” He summed it up saying: “pharmaceutical companies, in the documentation that they provide, the insert leaflets and so on, they are certainly not permitted to make claims for benefits without evidence, and I think the converse of that is true as well, that they shouldn’t be pronouncing risks where a sufficient body of evidence doesn’t exist. Now, that might sound a little complacent by the system, but that’s my understanding of how it worked.”[2304] Third, in the chapter on Pharmaceutical Companies criticisms are made that warnings were neither sufficiently informative nor forceful, in particular, first, of non-A non-B Hepatitis specifically (rather than using a broad term such as “virus” or “hepatitis”) and, second, in relation to the association between factor concentrates and AIDS. So too was this the case in respect of BPL/PFL and PFC.
An assumption that clinicians would spell out risks to patients may help to explain why risks were not highlighted to patients by manufacturers, but it critically depended upon an assumption being made about the practice of others – and the overwhelming weight of the evidence which the Inquiry has received indicates that the assumption was erroneous. His account of how information about risks was to be handled is concerning: if accurate, it displays a woeful approach to ensuring safety so far as the licensing authority is concerned. If, as is more likely, it was Dr Perry’s actual, but erroneous, view of the approach the regulator would take it shows that work needed to be done by the Medicines Division of the DHSS[2305] to ensure that those involved in the preparation and administration of pharmaceutical and biological products understood that risk needed to be highlighted, rather than marked down as requiring further study and more proof before it could even be raised as a risk, let alone an actuality. The exchange speaks of a complacency to risk by authority, and demonstrates that that is what significant figures in the field such as Dr Perry thought the culture was.
The purpose of warnings is to communicate that there is a risk to those who need to know of it. A proper approach by manufacturers to risk – that is, they should alert professional users and patients to risks of which they are aware once there is enough material to show that there is such a risk – is one aspect of a system which has three points at which notice of a risk may be given: by the manufacturer, by the regulator, by the prescribing clinician. The system should ensure that the patient is properly informed of the risk. It cannot achieve this if the manufacturer does not say sufficient about the risk but leaves that to the regulator or clinician, if the regulator in turn does not require a full account of the risks or prevents the manufacturer from talking of risk because it looks for certainty, and if the clinician leaves it to the manufacturer (or regulator) to reveal the risk. What could be a “triple fail-safe” in effect becomes instead a system in which each part leaves the matter to the other. In the case of BPL/PFC the same failings are evident in respect of the manufacturer’s part in this system – that of product labelling (for the patient and any prescribing clinician) – as they were in respect of the labelling and product warnings given in respect of commercial concentrates.
This chapter has shown that a large cohort of patients was exposed by an increase in pool sizes to a much greater risk of contracting hepatitis, in particular non-A non-B Hepatitis, during the 1970s than would have been the case had single-donor or small pool products been used. This was at a time when the risks of hepatitis, and in particular non-A non-B Hepatitis, were becoming ever clearer. It was thus at a time when efforts should have intensified to reduce those risks. The story of this chapter is that instead of reducing it, those responsible for the production and control of blood products in the UK increased it. Not marginally – but very, very significantly. The evidence about product labelling shows that, at least so far as BPL was concerned, civil servants in the DHSS knew of the increase. Indeed, the evidence about consultation with the Medicines Division and the Medicines Control Agency confirms that this must have been drawn to their attention if only they had compared one label, showing a greater maximum number, with its predecessor.
There were some reductions in the risk in the early 1970s, following on from the introduction of tests for the presence of Hepatitis B, though these were capable of detecting only a minority of infections when first introduced, and were never until the early 1980s capable of identifying most infections. These reductions pale by comparison with the extent of the increased risk from increased pool sizes. Dr Maycock’s view that testing offered a defence (by reducing the risk in one way) to increasing the risk (in another way) was ill-considered. The argument that a reduction of risk in one way justifies an increase in risk in another way is without merit, especially if priority is to be given, as it should have been, to safety. The one should be reduced where it can be; the other should not be increased.
The fact of increasing pool sizes should have given impetus to research efforts to achieve viral inactivation. If the state, for its purposes, increases a risk it should all the more strive to take measures which will then reduce or eliminate it. As is apparent from the chapters which have gone immediately before this, the state did not.
Pool sizes mattered. Some claims have been made that they did not matter much, because people with bleeding disorders required frequent treatment, and so – whether cryoprecipitate or factor concentrates were used – they would suffer in any event. Non-A non-B Hepatitis could not be screened out until 1989: so there was simply no way of knowing for sure if any treatment was or was not infective so far as that was concerned. However, this argument ignores a number of factors. First, it does not apply to those who were infrequently treated. Second, those frequently treated would be exposed to a much greater extent to multiple viruses, some of which might not yet be identifiable but were nonetheless potentially threatening. Third, it significantly increased the risk of new viruses taking a hold, as materialised with HIV when infected donations reached many people. Fourth, the received wisdom was that children, or people newly diagnosed with bleeding disorders (“previously untreated patients” or “PUPs”), should receive single-donor cryoprecipitate as a mainstay of therapy, and not concentrate, and yet these classes were as likely to consist of the same proportion of those who needed repeated treatment as other patients: the reason was to avoid the risks of hepatitis which concentrates brought in their wake. Fifth, the claim of inevitable infection would suggest that commercial concentrates were no worse than NHS concentrates or cryoprecipitate, whatever the relative pool sizes: yet the weight of the evidence shows that this is not so.
Though it is apparent on an impressionistic basis that commercial concentrates were riskier, and that treatment regimes using more NHS concentrate or cryoprecipitate seemed to be less infective, it can actually be demonstrated that people with severe haemophilia did not inevitably suffer from hepatitis whatever their form of treatment. For instance, in the Netherlands, where cryoprecipitate was the favoured treatment, the infection rate of those so treated was very considerably lower than those receiving large pool concentrates.[2306] In Norway, people with bleeding disorders were treated with factor products from “a relatively small and stable pool of domestic, non-paid donors” and a study of serum samples taken in 1985 and 1986 found the overall proportion with Hepatitis C was 41%, and for those with severe Haemophilia A or B it was 64% or 67%, respectively.[2307] Dr Brian Colvin and Dr Craske studied a small cohort of patients treated only with cryoprecipitate between October 1982 and July 1984. None developed hepatitis. A retrospective study in the same paper also showed that of 166 patients treated solely with cryoprecipitate only 2 had seroconverted with HIV; of 198 treated with NHS concentrate alone, 20 had.[2308] It is also to be noted that at a meeting at the National Institute for Biological Standards and Control (“NIBSC”) in February 1984 the discussion suggested that “the 100% incidence of non-A, non-B hepatitis is recent and is related to increased pool size since 1978.”[2309]
The thesis that the greater rate of hepatitis shown in the early 1970s to result from using commercial products was not so much because of the pool size used as it was because of the donor population makes little sense. The risk in each case is caused by the chance that a blood product made from that donation contains an infective viral particle. The chance is higher in populations which sell their blood, especially if they come from more dubious environments. It is higher because the recipient is exposed to more viral particles than they would be in the case of a carefully selected, voluntary, donor. The risk from increased pool sizes is the same: it is exposing the recipient to yet more viral particles. In each case, pooling will therefore increase the risk.
In short, if there is an acknowledged risk that treating a patient with a single donation product might transmit hepatitis, why should that risk then be multiplied several times on every occasion the patient needs treatment? Had cryoprecipitate or small pool fractions been more widely available, it is probable that the same extent of infection would not have occurred.
What was described in the introduction to this chapter as a surging rise in pool size was, in itself, responsible for a significant increase in the risk that people with bleeding disorders in the UK would suffer AIDS. It also increased the risk that they might suffer hepatitis – at least up to the point at which pool sizes in any event became so large that most who received product from it would in due course be infected.[2310] The thrust of this chapter, however, is that that position should never have been reached.
(1) The Observer Killer disease alert over gay blood donors 1 May 1983 MDIA0000016
(2) Other measures could have been taken to reduce the risk of transmission but were not. See the chapters on Knowledge of Risk Before 1970, Hepatitis Risks 1970 and After, and Blood Transfusion: Clinical Practice.
(3) The downside of any protective measure would also need to be considered.
(4) Including further risks arising out of the precaution taken.
(5) NHS Blood and Transplant did so in 2015. So, too, have the Joint United Kingdom Blood Transfusion and Tissue Transplantation Services Professional Advisory Committee and the Serious Hazards of Transfusion scheme, which cover every part of the UK, for which see the chapter on Blood Transfusion: Clinical Practice. The Alliance of Blood Operators Risk-Based Decision-Making Framework for Blood Safety is internationally widely agreed as an appropriate approach. Closing Submissions of NHSBT 16 December 2022 paras 17.4-17.9 SUBS0000062
(6) Beneficence (doing more good than harm), fairness, transparency, consultation, evidence and judgement, practicality and proportionality, vigilance, and continuous improvement. NHS Blood and Transplant Closing Submissions to Infected Blood Inquiry para 4.64 SUBS0000062
(7) The evaluation of this depends on a number of factors, principally the degree of risk, eg how severe the transfused disease is, the economics or cost of mitigation and societal and contextual factors – namely: ethical considerations in the distribution of risks and benefits; concerns and priorities associated with a particular risk source, or the approach to risk management, expressed or held by stakeholders and the public. See: NHS Blood and Transplant Closing Submissions to Infected Blood Inquiry paras 4.63-4.91 SUBS0000062
(8) Save in certain well-recognised circumstances, such as an unconscious patient requiring emergency treatment, or the treatment of a patient lacking mental capacity to consent to it.
(9) “not being informed fundamentally undermines your autonomy because you are denied the opportunity of real choice”. Medical Ethics Expert Panel Transcript 26 January 2021 p112 INQY1000090
(10) There is also a legal imperative: treatment of a patient without consent may be an assault, and where a patient suffers adverse consequences from treatment about which they were not sufficiently informed they may have a claim in negligence against the doctor or hospital. This chapter does not trace the progression of the case law regarding negligence claims based on lack of consent. The law has developed over time – see, in particular, the Supreme Court’s decision in Montgomery v Lanarkshire Health Board on 11 March 2015 – but those developments are concerned with the circumstances in which a patient can sue for damages. This Inquiry’s primary concern is with the ethical and moral requirement for informed consent.
(11) Expert Report to the Infected Blood Inquiry: Medical Ethics April 2020 p16 INQY0000241
(12) See further the chapters on People’s Experiences, Treloar’s, Haemophilia Centres: Policies and Practice and Blood Transfusion: Clinical Practice.
(13) Expert Report to the Infected Blood Inquiry: Medical Ethics April 2020 p16 INQY0000241
(14) Expert Report to the Infected Blood Inquiry: Medical Ethics April 2020 pp30-31 INQY0000241
(15) Expert Report to the Infected Blood Inquiry: Medical Ethics April 2020 p31 INQY0000241
(16) Adding that the meaning of respect for autonomy has been strengthened and clarified in ethics, law and clinical practice over the past decades. Expert Report to the Infected Blood Inquiry: Medical Ethics April 2020 p6 INQY0000241
(17) Medical Ethics Expert Panel Transcript 26 January 2021 pp106-108 INQY1000090
(18) Medical Ethics Expert Panel Transcript 26 January 2021 pp110-111 INQY1000090
(19) Medical Ethics Expert Panel Transcript 26 January 2021 pp112 INQY1000090
(20) Beauchamp and Childress’ Principles of Biomedical Ethics. Expert Report to the Infected Blood Inquiry: Medical Ethics April 2020 pp7-8 INQY0000241
(21) The lectures were delivered in 1980 and published in 1981; see in particular lecture 4, If I Were You, Mrs B. Professor Ian Kennedy Reith Lectures Transcript 26 November 1980 RLIT0000620
(22) Professor Ian Kennedy Reith Lectures Transcript 26 November 1980 p3 RLIT0000620
(23) For a more detailed chronology of published guidance and other advice, see: Ethical Guidance Chronology 18 May 2021 INQY0000008, Counsel Presentation on Ethical and Clinical Guidance for Clinicians and Other Healthcare Practitioners May 2021 INQY0000249, Counsel Presentation on Ethical and Clinical Guidance for Clinicians and Other Healthcare Practitioners Transcript 28 May 2021 INQY1000124
(24) The MDU is one of a number of medical defence organisations providing advice to clinicians on medico-legal issues. A purpose of such organisations is to help protect and prevent a doctor from being sued in the course of their practice, and as such their advice and guidance is clinician-focused. Counsel Presentation on Ethical and Clinical Guidance for Clinicians and Other Healthcare Practitioners May 2021 p13 INQY0000249
(25) Medical Defence Union Consent for Examination and Treatment p1 MOJU0000001_014. A further booklet published by the MDU in 1962 focused on consent for operative treatment and emphasised that the patient “should be given a fair and reasonable explanation, in non-technical language, of the effect and nature of the operation … If the operation contemplated carries special risks, which are probably unknown to the patient, he should, as a general rule, be informed of these risks”. Medical Defence Union Consent to Operative Treatment November 1962 p3 DHSC0100081
(26) The case was Bennan v Parsonnet (1912) 83 A. 948. Medical Defence Union Consent to Operative Treatment September 1966 p3 DHSC0103246
(27) Medical Defence Union Consent to Operative Treatment September 1966 p4 DHSC0103246. This guidance from the MDU was regularly updated; see: Counsel Presentation on Ethical and Clinical Guidance for Clinicians and Other Healthcare Practitioners May 2021 p21 INQY0000249
(28) The BMA is a professional association and trade union for doctors in the UK, which has had a medical ethics committee since 1849. The BMA is a founder member of the World Medical Association, which was established in 1947. Counsel Presentation on Ethical and Clinical Guidance for Clinicians and Other Healthcare Practitioners May 2021 p6 INQY0000249
(29) British Medical Association Medical Ethics 1970 BMAL0000085
(30) Except in relation to research; the text of the Declaration of Helsinki was fully set out in the BMA’s publication: British Medical Association Medical Ethics 1970 pp5-7 BMAL0000085
(31) British Medical Association Medical Ethics 1970 p11 BMAL0000085
(32) British Medical Association The Handbook of Medical Ethics 1980 pp10-11 BMAL0000087
(33) British Medical Association The Handbook of Medical Ethics 1981 p15 BMAL0000088
(34) The Declaration of Lisbon also recognised the right of the patient “to expect that his physician will respect the confidential nature of all his medical and personal details.” World Medical Association Declaration of Lisbon on the Rights of the Patients 1981 RLIT0001509
(35) This was the BMA’s “first major redraft” since the 1980 publication of the Handbook of Medical Ethics: “We have sought to set out the arguments and counterarguments which lead either to universally accepted ethical principles of practice or consensus views.” British Medical Association Philosophy and Practice of Medical Ethics 1988 p5 BMAL0000080
(36) British Medical Association Philosophy and Practice of Medical Ethics 1988 p35 BMAL0000080. See also chapter 4 of the handbook generally.
(37) British Medical Association Philosophy and Practice of Medical Ethics 1988 p13 BMAL0000080
(38) NHS Management Executive A Guide to Consent for Examination or Treatment August 1990 NHBT0007444_001, NHS Management Executive Consent form for medical or dental investigation, treatment or operation August 1990 NHBT0007444_002
(39) National Health Service in Scotland Management Executive A Guide to Consent to Examination, Investigation, Treatment or Operation 15 October 1992 PRSE0000713
(40) British Medical Association Medical Ethics Today: Its Practice and Philosophy 1993 p22 BMAL0000089
(41) British Medical Association Medical Ethics Today: Its Practice and Philosophy 1993 p27 BMAL0000089
(42) British Medical Association Medical Ethics Today: Its Practice and Philosophy 1993 p29 BMAL0000089
(43) British Medical Association Medical Ethics Today: Its Practice and Philosophy 1993 p33 BMAL0000089
(44) The amended Declaration of Lisbon was approved by the World Medical Association’s General Assembly in Bali in September 1995. World Medical Association Declaration of Lisbon on the Rights of the Patient September 1995 pp2-3 RLIT0001508
(45) The GMC’s role includes the maintenance of the official register of medical practitioners within the UK, oversight of medical education and training, the setting of professional standards for doctors, and the regulation of the conduct of doctors through fitness to practise procedures.
(46) General Medical Council Good Medical Practice October 1995 p2 RCGP0000533_005
(47) General Medical Council Seeking patients’ consent: the ethical considerations November 1998 p5 GMCO0001728. The GMC has continued to issue guidance on consent, most recently Decision making and consent which was published in November 2020. General Medical Council Decision making and consent effective from 9 November 2020 WITN3365040
(48) In relation to treatment, testing and research.
(49) Expert Report to the Infected Blood Inquiry: Medical Ethics April 2020 p6 INQY0000241
(50) Expert Report to the Infected Blood Inquiry: Medical Ethics April 2020 p10 INQY0000241. As the expert group explained, there are numerous historical examples of once-accepted practice that horrify us today, such as the pelvic examination of women under anaesthetic at training hospitals without their consent, or the retention of organs from children who had died without parental consent. Expert Report to the Infected Blood Inquiry: Medical Ethics April 2020 pp6-7 INQY0000241
(51) Expert Report to the Infected Blood Inquiry: Medical Ethics April 2020 p11 INQY0000241
(52) Mitochondria produce energy: a red blood cell needs little energy to fulfil its functions.
(53) The difference between male and female is because of a combination of the average comparative sizes, and hence circulating fluid, of each sex and because women menstruate. The time is necessary in particular to replace the iron contained in red blood cells. Because iron is toxic in larger amounts, the body does not keep a store of it.
(54) Meaning cells with granules.
(55) Albumin is the most abundant protein in plasma. Fibrinogen is important in the clotting process.
(56) Antigens can be from self or external, but are recognised as foreign (ie “autoimmunity” comes from a response to “autoantigens”).
(57) Antibodies are produced in vast amounts. Some estimates suggest that the body’s immune system can recognise a million or so different antigens and mount an immune attack on them by producing from somewhere between 100,000 to 1,000,000 different antibody molecules. However, despite their number, they are classified into only five major classes. Antibodies are actually immunoglobulins, and the terms “antibody” and “immunoglobulin” can be used interchangeably. The five classes are immunoglobulin G (Ig G), immunoglobulin M (Ig M), immunoglobulin A (Ig A), immunoglobulin D (Ig D) and immunoglobulin E (Ig E). They can be found in blood plasma. Immunoglobulin G is the most common: of the antibodies isolated from plasma it represents around 80%.
(58) There is otherwise a risk that the CD4 activity may start to damage the body it is meant to protect, or prevent responses to other threats.
(59) Expert Report to the Infected Blood Inquiry: HIV January 2020 p3 EXPG0000004
(60) Expert Report to the Infected Blood Inquiry: HIV January 2020 p59 EXPG0000004
(61) HIV infection may not, however, be the only cause of an inverted T-cell ratio.
(62) Pandit Christopher Wren’s Medical Discoveries: The ‘Architect of Human Anatomy’ 17 May 2023 pp3-6 RLIT0002441
(63) The Method Observed in Transfusing the Blood out of One Animal into Another Philosophical Transactions 17 December 1666 RLIT0002313
(64) An extract of a letter written by J. Denis Philosophical Transactions 10 February 1668 RLIT0002442
(65) An Account of the Experiment of Transfusion, Practised Upon a Man in London Philosophical Transactions 9 December 1667 RLIT0002315
(66) Bynum Blood Feud Nature 14 April 2011 p2 RLIT0002358, McLoughlin The British Contribution to Blood Transfusion in the Nineteenth Century The British Journal of Anaesthesia 1959 p1 RLIT0002357
(67) Initially he used a large syringe to draw off blood, and quickly transferred it to the recipient before it had time to coagulate, taking care to expel air from the syringe as he did so. By 1829 he wrote a four-page article in The Lancet describing what was then his process, which involved using apparatus manufactured commercially specially for the purpose and known as a “Gravitator”. Blundell Experiments on the Transfusion of Blood by the Syringe Medico-Chirurgical Transactions 3 February 1818 RLIT0022444, Blundell Observations on Transfusion of Blood The Lancet 13 June 1829 pp1-4 RLIT0002175
(68) Hoyer Hemophilia A New England Journal of Medicine 1994 CGRA0000623, Wellcome symposium Wellcome Witnesses to Twentieth Century Medicine Haemophilia: Recent History of Clinical Management September 1999 p14 RLIT0000022
(69) Lane Haemorrhagic Diathesis: Successful Transfusion of Blood The Lancet 28 September 1840 RLIT0002176
(70) Masson A History of Blood Transfusion in Edinburgh p10 NHBT0000105_007
(71) Giangrande The History of Blood Transfusion British Journal of Haematology 2000 p3 RLIT0001218
(72) The role of Rhesus factor in compatibility of blood groups is acknowledged though not detailed here.
(73) The Voluntary Blood Donor 1975 p3 SBTS0000605_005
(74) Van Hee The Development of Blood Transfusion: the Role of Albert Hustin and the Influence of World War I Acta Chirurgica Belgica 2015 pp5-6 RLIT0002443
(75) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine 1996 p11 NHBT0000028
(76) The Voluntary Blood Donor 1975 p3 SBTS0000605_005
(77) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine 1996 pp12-15 NHBT0000028
(78) Girdwood Fifty Years of an Organised Blood Transfusion Service in Scotland 1990 pp1-2 PRSE0003986
(79) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine 1996 p18 NHBT0000028. The term “blood bank” in fact originated from the work of Bernard Fantus in Chicago who set up the first such bank in the US in 1937 when he preserved, refrigerated and stored donor blood. Giangrande The History of Blood Transfusion British Journal of Haematology 2000 p5 RLIT0001218
(80) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine 1996 pp19-20 NHBT0000028, Dame Janet Vaughan’s Personal Notes of Wartime Experiences pp2-3 RLIT0002314
(81) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine 1996 pp21-22 NHBT0000028. The first regional depots were in Newcastle, Leeds, Nottingham, Cambridge, Birmingham, Oxford, Cardiff, Manchester, Liverpool and later Belfast.
(82) Girdwood Fifty Years of an Organised Blood Transfusion Service in Scotland 1990 pp3-4 PRSE0003986. The regional centres were in Aberdeen, Dundee, Edinburgh, Glasgow and Inverness.
(83) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine 1996 pp72-74 NHBT0000028
(84) Bennett et al Cryoprecipitate and the Plastic Blood-bag System: Provision of Adequate Replacement Therapy for Routine Treatment of Haemophilia British Medical Journal April 1967 p3 RLIT0000682
(85) Forbes The Haemophilias: Clinical and Laboratory Investigations p24 RLIT0002185
(86) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine 1996 pp74-75 NHBT0000028
(87) Scottish National Blood Transfusion Service Plasma Fractionation in Scotland 2008 p1 PRSE0001732
(88) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine 1996 pp46-47 NHBT0000028
(89) Edsall Edwin Joseph Cohn 1892-1953 A Biographical Memoir 1961 pp19-21 RLIT0002317. His team had been systematically studying dividing blood plasma into its constituent protein fractions (“fractionation”) since 1938.
(90) Dr Peter Foster Transcript 24 March 2022 pp10-12 INQY1000197, Cohn et al Preparation and Properties of Serum and Plasma Proteins. IV. A System for the Separation into Fractions of the Protein and Lipoprotein Components of Biological Tissues and Fluids March 1946 pp3-4 PRSE0002176
(91) Expert Report to the Infected Blood Inquiry: Fractionation February 2022 pp25-26 EXPG0000044
(92) Bradley et al An Episode of “Homologous Serum Jaundice” British Medical Journal 26 August 1944 DHSC0100008_148
(93) Letter from Dr Maycock to Dr Alistair Robb-Smith 19 August 1946 DHSC0100008_190
(94) Brightman and Korns Homologous Serum Jaundice in Recipients of Pooled Plasma Journal of American Medical Association 4 October 1947 p5 RLIT0000054
(95) Scottish National Blood Transfusion Association Scottish Hospital Memorandum No 89 16 December 1964 p3 PRSE0000157
(96) Grant Complications of Blood Transfusion The Practitioner August 1965 p8 PRSE0003897
(97) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine 1996 p5 NHBT0000028
(98) The suffix “itis” in medical terminology indicates an inflammation.
(99) The suffix “osis” in medical terminology generally means a state of being.
(100) Alanine aminotransaminase.
(101) Aspartate aminotransferase.
(102) Hepatitis D, or delta virus, is not able to replicate and produce a new virus on its own. It relies on the presence of Hepatitis B and may be characterised as “a subset of hepatitis B overall.” The combination of Hepatitis B and Hepatitis D is associated with a higher risk of cirrhosis, liver failure and liver cancer. Hepatitis Expert Panel Transcript 26 February 2020 p12, pp66-67 INQY1000052
(103) Blumberg et al A “New” Antigen in Leukemia Sera Journal of the American Medical Association 15 February 1965 PRSE0001518
(104) See the chapter Knowledge of Risk Before 1970.
(105) Anti-HBc refers to antibodies that the immune system produces against the core of the Hepatitis B virus, indicating past or present infection. It is detectable around the onset of clinical symptoms and is a reliable and persistent marker that an individual has ever had Hepatitis B infection. Expert Report to the Infected Blood Inquiry: Hepatitis January 2020 p15 EXPG0000001
(106) Expert Report to the Infected Blood Inquiry: Hepatitis January 2020 p3 EXPG0000001
(107) Expert Report to the Infected Blood Inquiry: Hepatitis January 2020 p9, p28, p30 EXPG0000001, Hepatitis Expert Panel Transcript 26 February 2020 pp62-65 INQY1000052
(108) Hepatitis Expert Panel Transcript 26 February 2020 pp26-30 INQY1000052
(109) They could, therefore, require treatment durations of up to 72 weeks, with ongoing risks of toxicity from their treatment. Expert Report to the Infected Blood Inquiry: Hepatitis January 2020 p52 EXPG0000001
(110) Hepatitis Expert Panel Transcript 26 February 2020 pp135-144 INQY1000052. Other possible complications included nervous system disorders (headaches, dizziness, impaired concentration, memory impairment, tremors, nightmares), peripheral neuropathy, tachycardia, hypertension, vascular disorders and pulmonary embolism. Expert Report to the Infected Blood Inquiry: Hepatitis January 2020 pp45-46 EXPG0000001
(111) Very common side-effects included anaemia, neutropaenia, depression, insomnia, headache, dizziness and impaired concentration. Other common side-effects were thyroid disorders, mood alteration, emotional disorders, anxiety, aggression, memory impairment, visual blurring, vomiting, rash, photosensitivity, back pain, impotence and weight loss. Expert Report to the Infected Blood Inquiry: Hepatitis January 2020 p44 EXPG0000001
(112) The Hepatitis Expert Panel explained that “there is quite a significant risk of sexual transmission from hepatitis B and we still see cases particularly in adults of sexual transmission of hepatitis B.” Hepatitis Expert Panel Transcript 26 February 2020 p45 INQY1000052
(113) See the chapter on Viral Inactivation.
(114) Expert Report to the Infected Blood Inquiry: Hepatitis January 2020 pp24-25 EXPG0000001
(115) Expert Report to the Infected Blood Inquiry: Hepatitis January 2020 pp60-61 EXPG0000001
(116) The fluid can be drained off to relieve the symptoms but this does not prevent the fluid from re-forming. Ascites can also include swelling in the lower limbs. Hepatitis Expert Panel Transcript 26 February 2020 pp106-108 INQY1000052
(117) Expert Report to the Infected Blood Inquiry: Hepatitis January 2020 p27 EXPG0000001
(118) Hepatitis Expert Panel Transcript 26 February 2020 pp90-92 INQY1000052
(119) Expert Report to the Infected Blood Inquiry: Hepatitis January 2020 pp60-61 EXPG0000001
(120) Expert Report to the Infected Blood Inquiry: Hepatitis January 2020 p4, p8, pp26-30 EXPG0000001
(121) See the chapter Blood and Transfusion for an explanation of this. Some people do experience a variety of symptoms or conditions during the chronic phase which do not meet the defining criteria for AIDS but are associated with disturbed cellular immunity, such as candidiasis, herpes zoster and constitutional symptoms such as fever, diarrhoea and listeriosis. Expert Report to the Infected Blood Inquiry: HIV January 2020 p6 EXPG0000004
(122) Expert Report to the Infected Blood Inquiry: HIV January 2020 pp7-9, pp35-36 EXPG0000004 . In 1993 the classification was revised to emphasise the importance of a low CD4 T-lymphocyte count and three clinical conditions were added to the definition (pulmonary tuberculosis, recurrent pneumonia and invasive cervical cancer).
(123) See the chapter on Viral Inactivation.
(124) See the chapter about Knowledge of the Risks of AIDS.
(125) The period during which people are asymptomatic following infection is known as clinical latency: Expert Report to the Infected Blood Inquiry: HIV January 2020 p24 EXPG0000004
(126) Expert Report to the Infected Blood Inquiry: HIV January 2020 p6 EXPG0000004
(127) HIV Expert Panel Transcript 27 February 2020 pp93-100 INQY1000053, Expert Report to the Infected Blood Inquiry: HIV January 2020 pp50-51, p53 EXPG0000004
(128) Expert Report to the Infected Blood Inquiry: HIV January 2020 pp41-43 EXPG0000004
(129) The UNAIDS aim worldwide is 90-90-90 (detecting a minimum of 90% of those infected, treating 90% of them, with 90% reduced to undetectable viral loads). In the UK currently 97% of those identified received treatment, and 97% of them have undetectable viral loads. The description U=U is often used to convey the idea that an undetectable level of the virus means that it cannot be transmitted.
(130) Expert Report to the Infected Blood Inquiry: HIV January 2020 pp26-28 EXPG0000004, HIV Expert Panel Transcript 27 February 2020 pp72-73 INQY1000053
(131) Hepatitis Expert Panel Transcript 26 February 2020 pp159-165 INQY1000052, HIV Expert Panel Transcript 27 February 2020 pp88-90 INQY1000053, Expert Report to the Infected Blood Inquiry: Hepatitis January 2020 pp51-54 EXPG0000001, Expert Report to the Infected Blood Inquiry: HIV January 2020 p60 EXPG0000004
(132) This chapter considers the treatments available during the period when infections were transmitted. For information regarding more modern treatments and current treatments see Expert Report to the Infected Blood Inquiry: Bleeding Disorders and Blood Disorders January 2020 EXPG0000002
(133) 100% therefore does not mean the most there can be: it means 100% of the average level.
(134) In some classifications, 2% is adopted instead as the cut-off point between severe (less than 2%) and moderate, but this is less common than the 1% quoted in the text.
(135) Conventionally – until recently – the numeral “8” was represented by the Roman numeral “VIII”, and “9” by “IX”. In the text, the more modern Arabic numerals are adopted except where quoting from a document where the Roman numbering system has been used.
(136) The male pronoun has been used deliberately – it is only rarely the case that someone who suffers from severe Haemophilia A is female, because the gene which expresses itself as an inability to produce sufficient Factor 8 to clot efficiently is sex-linked to the X chromosome, and for a female to suffer, both alleles would have to give rise to a similar deficiency.
(137) Some classifications use 40%, for example the Centers for Disease Control and Prevention (“CDC”).
(138) Expert Report to the Infected Blood Inquiry: Bleeding Disorders and Blood Disorders January 2020 pp23-24 EXPG0000002
(139) Though the treatment differed: Factor 8 concentrates tended to have insufficient von Willebrand factor, such that long after concentrates were in general use for people with haemophilia it remained practice to administer cryoprecipitate or thawed fresh frozen plasma to those who had von Willebrand disorder.
(140) The evidence is that this, mercifully, is rare by comparison with joint and intramuscular bleeds: but it is nonetheless a risk of non-treatment.
(141) A descriptive phrase used by Dr Anthony Aronstam in: Aronstrom Haemophilic Bleeding: Early Management at Home 1985 p27 RLIT0000666
(142) The state of such a joint caused to be arthritic by internal bleeding is known as haemarthrosis.
(143) In 1937, Dr Carroll Birch described 113 patients with haemophilia, of whom 82 died before the age of 15 years, often from a trivial injury. Only 20% of people with severe haemophilia could expect to live beyond the age of 20. Biggs Thirty Years of Haemophilia Treatment in Oxford British Journal of Haematology 1967 RLIT0000043_021
(144) Witness Mr BC for instance told the Inquiry that such were the effects of his haemophilia before he went to Lord Mayor Treloar’s College that: “I think at age six I went to school for three days in the year. And then in the following year, I think I probably went for about nine days.” ANON Transcript 23 June 2021 p3 INQY1000133
(145) Though the level of 25% is not a constant – the activity of Factor 8 declines over time, such that the half-life of Factor 8 in most transfusions was approximately 12 hours. Extended half-life preparations are now often administered.
(146) See the chapter on Blood and Transfusion for further detail.
(147) Now more usually 42 days, an increase achieved through use of different anticoagulants.
(148) Giangrande Porcine factor VIII Haemophilia2012 RLIT0000630. See also Expert Report to the Infected Blood Inquiry: Bleeding Disorders and Blood Disorders January 2020 p18 EXPG0000002 and Dr Ethel Bidwell in Wellcome symposium Wellcome Witnesses to Twentieth Century Medicine Haemophilia: Recent History of Clinical Management September 1999 pp23-24 RLIT0000022
(149) Expert Report to the Infected Blood Inquiry: Bleeding Disorders and Blood Disorders January 2020 p18 EXPG0000002
(150) Cohn et al Preparation and Properties of Serum and Plasma Proteins. IV. A System for the Separation into Fractions of the Protein and Lipoprotein Components of Biological Tissues and Fluids Journal of the American Chemical Society March 1946 PRSE0002176. It had been discovered that every protein has a solubility which is almost unique to it, almost like a fingerprint, so that it will separate out from a solution of other proteins if the conditions are right for it to do so.
(151) Kekwick et al A concentrate of Human Antihaemophilic Factor: Its use in six cases of haemophilia The Lancet 30 March 1957 RLIT0000043_013
(152) Sometimes antihaemophilic globulin (“AHG”).
(153) Dr David Evans, Wellcome symposium. Wellcome Witnesses to Twentieth Century Medicine Haemophilia: Recent History of Clinical Management September 1999 p34 RLIT0000022
(154) Dr Evans, Wellcome symposium. Wellcome Witnesses to Twentieth Century Medicine Haemophilia: Recent History of Clinical Management September 1999 pp34-35, pp43-44 RLIT0000022
(155) Foster The manufacture of blood plasma products in Scotland: a brief history Scottish Medical Journal 2016 p2 WITN3530032
(156) Draft Expert Witness Statement of Dr Terence Snape to the Tribunal of Inquiry into Infections with HIV and Hepatitis C of persons with Haemophilia and Related Matters NHBT0004065_003. See especially page 2.
(157) Pool et al Production of High-Potency Concentrates of Antihemophilic Globulin in a Closed Bag System New England Journal of Medicine 30 December 1965 p1 PRSE0003922
(158) Repeated fractionation, through four or five steps, produced immunoglobulin and albumin, both of central importance to healthcare. Though the focus of the Inquiry has been on Factors 8 and 9, the importance of these products should not be forgotten.
(159) Though it was only slowly phased out in the UK: even in the mid 1970s some regional transfusion centres were still using bottles. Plastic bags were increasingly used for fresh frozen plasma, initially in five-litre packs. A change to single plastic packs was instigated by Dr Richard Lane in an attempt to secure a greater yield of Factor 8 from frozen plasma (they were quicker to freeze and to thaw, at both stages therefore ensuring that the Factor 8 in the plasma had the least time in which to degrade), to ensure greater freedom from bacterial contamination, and to enable easier handling when a wedge-shaped design was used. See the chapter Self-Sufficiency.
(160) This is often, mistakenly, described as the date of discovery of cryoprecipitate. It was not. It was however the date when a way of utilising the precipitate to treat haemophilia was first realised, and soon after Dr Pool reported this advance it came into regular use as something of a game changer. Pool et al Production of High-Potency Concentrates of Antihemophilic Globulin in a Closed Bag System New England Journal of Medicine 30 December 1965 PRSE0003922
(161) Though cryoprecipitate could be administered at home, and some clinicians such as Dr Katharine Dormandy (Royal Free Hospital) were keen on this and on developing it further. A number of the haemophilia centres also arranged for some patients to self-administer at home: see further below and the chapter on Haemophilia Centres: Policies and Practice.
(162) Jones Letters to the Editor discussing the use of Anti-Haemophilic Factor cryoprecipitate infusion 8 April 1967 PJON0000136_001
(163) Jones Answering the Needs of Haemophilic Children and Their Families Community Medicine 28 July 1972 p1 HSOC0022656
(164) He wrote: “The introduction of cryoprecipitate, a FVIII-rich fraction of fresh plasma discovered by Dr Judith Pool and her colleagues working in Stanford, provided the solution to [the problems of having to undergo continuous transfusion, meaning a child had to be admitted to a bed, and the level of Factor 8 that could be obtained without circulatory overload]. Cryoprecipitate can be given by syringe, a full factor VIII dose being contained in a small volume of residual plasma. Within weeks of its introduction in-patient figures had fallen, and without the fear of hospitalization and ‘the drip’ children were presenting earlier and more often for quick out-patient therapy. Cryoprecipitate is now the product of choice in major surgery, allowing the potent but antigenic animal fractions and expensive human concentrate to be reserved for major complications, the emergency treatment of patients with FVIII inhibitors or, in the case of concentrate, for prophylaxis.” Jones Answering the Needs of Haemophilic Children and Their Families Community Medicine 28 July 1972 p1 HSOC0022656. He was dismissive of the risk of adverse reactions.
(165) Optimum Use of Factor VIII Preparations at Present Available in the United Kingdom September 1974 p1 OXUH0000757
(166) See the discussion of his contribution to Seminars in Hematology, October 1977, discussed in: Counsel Presentation on First Cardiff AIDS Patient and Newcastle Haemophilia Centre Transcript 2 February 2021 pp137-140 INQY1000092. Of relevance to assessing the strength of the point made by a number of clinicians that cryoprecipitate might cause a significant number of allergic reactions is his observation that “Although transitory allergic reactions ... are commonly experienced with cryoprecipitate therapy, they are easily controlled with antihistamines. It is our practice to give … [Piriton] ... intravenously with each dose of cryoprecipitate.” Jones Developments and Problems in the Management of Hemophilia Seminars in Hematology October 1977 pp8-9 PJON0000147_001
(167) See her expert report for the HIV litigation: Expert Witness Report regarding HIV Litigation May 1990 pp6-7 CBLA0000072_024
(168) Expert Witness Report regarding HIV Litigation May 1990 pp12-13 CBLA0000072_024
(169) A Profile of the Management of Haemophilia in Northern Ireland 25 March 1988 p2 RHSC0000067_002
(170) See for example Written Statement of Dr Mark Winter para 35.3 WITN3437002. Dr Winter also suggested that cryoprecipitate could not be used in children readily “because of the high volume”. However this is difficult to reconcile with the fact that (as recognised by Professor Arthur Bloom and Dr Charles Rizza in their letter of 24 June 1983 to haemophilia centre directors) cryoprecipitate was used for the treatment of children by many directors; and the evidence before the Inquiry from some clinicians suggests that their policy for the treatment of children under the age of six (or sometimes four) was to use cryoprecipitate (although this was not always adhered to in practice). Letter from Professor Bloom and Dr Rizza to Haemophilia Centre Directors 24 June 1983 HCDO0000270_004
(171) Dr Mark Winter Transcript 1 October 2020 pp93-95 INQY1000059
(172) See the section on Haemophilia B in the chapter Haemophilia Centres: Policies and Practice.
(173) For a detailed examination of how haemophilia centres treated people in the 1970s and 1980s see the chapter Haemophilia Centres: Policies and Practice.
(174) Though by 1975 around 50% of haemophilia centres were using cryoprecipitate for some part of their home therapy programmes. Minutes of Haemophilia Centre Directors meeting 18 September 1975 OXUH0003735. In 1976 a survey by the UK Haemophilia Centre Doctors’ Organisation (“UKHCDO”) showed that 13 centres used it in home therapy, four of them to the exclusion of concentrates; and in 1977 the Home Therapy Working Party of UKHCDO had regard to figures showing an increased use for that year of cryoprecipitate in home therapy. Minutes of UK Haemophilia Centre Directors Home Therapy Working Party meeting 11 October 1978 p3 NTHT0000042, discussed at: Counsel Presentation on First Cardiff AIDS Patient and Newcastle Haemophilia Centre Transcript 2 February 2021 p155 INQY1000092
(175) This shift is examined in more detail in the chapter Haemophilia Centres: Policies and Practice.
(176) See the chapters on Regulation of Commercial Factor Concentrates and Pharmaceutical Companies for more detail.
(177) It was run by the North West Thames Regional Health Authority jointly with the DHSS from 1978 onwards. See the chapter on Self-Sufficiency.
(178) Biggs Jaundice and Antibodies Directed against Factors VIII and IX in Patients Treated for Haemophilia or Christmas Disease in the United Kingdom British Journal of Haematology 1974 p6 HCDO0000581. The paper had first been presented in draft to the Expert Group on the Treatment of Haemophilia on 20 March 1973, so by 1974 even more than in 1973 it may not have represented up-to-the-minute views in the light of greater experience with factor concentrates. Factor VIII Concentrates and the Treatment of Haemophilia PRSE0002553. At the time it was first presented, Oxford had only just started treatment with commercial concentrates, Sheffield treated conservatively, and Scotland first used commercial concentrates in the following year. The report it made was on the incidence of jaundice between 1969 and 1971, when tests for the presence of the Hepatitis B viral antigen were in their infancy. The paper records that one sixth (only) of the patient cohort considered were tested for the presence of the antigen (302 out of 1837 patients) by 7 different centres in different ways. The mean size of the pools was said to be 192, and thus well below the 300-donor threshold adopted shortly after the war as the point beyond which risks of hepatitis increased markedly.
(179) See the chapter on Pool Sizes.
(180) “Purity”, as used in respect of blood products, does not denote freedom from contamination by viruses or bacteria, but the relative absence of any protein other than the protein of interest.
(181) Technically, in the UK this was the result of a shift by 1974 from using a method developed in Sweden by Margareta Blombäck (1958) to one developed in New York by Johnson (Newman et al, 1971).
(182) And also the increased ability to assay the product to determine the amount of Factor 8 activity it contained. To do this required the sacrifice of minimal amounts from the batch being assayed, but gave greater confidence that treatment had used the appropriate amount of concentrate for the recipient and for their bleed than was the case with cryoprecipitate where there was much greater uncertainty about the resultant level of Factor 8 in the bloodstream.
(183) Indeed, “home treatment” meant just that – providing treatment at home, such as that which would have been provided in hospital in response to admission for treatment of a bleed, and is to be distinguished from preventative treatment, known as “prophylactic” treatment, where factor concentrate was injected as a precaution, in advance of, and in order to stave off, a bleed.
(184) Practices differed between different centres: Professor Charles Hay in evidence acknowledged that by contrast with Manchester and Liverpool where there was little prophylaxis during the 1980s, centres such as Newcastle and Treloar’s adopted it much earlier. Professor Charles Hay Transcript 4 November 2020 pp10-12 INQY1000072, Professor Charles Hay Transcript 5 November 2020 pp111-112 INQY1000073
(185) At first exclusively cryoprecipitate, then increasingly factor concentrate.
(186) Dr Biggs noted that the age of death of people severely affected with haemophilia had “more than doubled” as a result of the therapy in her article: Biggs Haemophilia Treatment in the United Kingdom from 1969 to 1974 British Journal of Haematology 1977 p4 DHSC6887729_105. The improvement was maintained, but at a much slower rate, as the effects of previous therapy on the younger cohort began to feed through to demonstrable results, and as a greater emphasis was placed on the home treatment made more easily possible with factor concentrates: see the article by Dr Rizza and Dr Rosemary Spooner, who reported that during that period the average ages of the patients who died were 46.7 years in the Haemophilia A group and 48.3 years in the Haemophilia B group. Comparable figures for 1969-74 were 42.3 years and 33.6 years, respectively. Rizza and Spooner Treatment of haemophilia and related disorders in Britain and Northern Ireland during 1976-80: report on behalf of the directors of haemophilia centres in the United Kingdom British Medical Journal 19 March 1983 p5 HCDO0000586
(187) Except for a short-lived increase in 1983-84, perhaps because it was known to be less likely than factor concentrates to transmit the cause of AIDS or of hepatitis.
(188) The exception was when commercial heat-treated Factor 9 was available before domestic heat-treated Factor 9. See the chapter Haemophilia Centres: Policies and Practice.
(189) Annual Consumption of Factor VIII in UK 23 August 1999 DHSC0006789_046, Pivot Table 5.3.1 showing Annual Consumption of CFC 1976 to 1994 WITN3826017
(190) Expert Report to the Infected Blood Inquiry: Bleeding Disorders and Blood Disorders January 2020 p34 EXPG0000002
(191) An umbrella term which covers both cryoprecipitate and freeze-dried concentrate, but can also extend to fresh frozen plasma or even whole blood.
(192) Termed supply “on a named patient basis”. At Oxford, it is plain from correspondence that commercial concentrate was available for use from before mid 1972, and the review by Dr Biggs of Haemophilia treatment in the UK from 1969 to 1974 records some usage of it in the UK (see Table VII in Biggs Haemophilia Treatment in the United Kingdom from 1969 to 1974 British Journal of Haematology p7 PRSE0004645) but a licence was first granted for the importation of Hemofil in February 1973 (a US product), and Kryobulin in March 1973 (an Austrian product, though it is unclear where the plasma used to make it originated: the probability is that at least a proportion of it derived from US donors or plasma brokers).
(193) The use of prophylactic therapy was increased only patchily through the late 1970s and 1980s. It was by no means as rapid as the seemingly obvious parallel in the use of injectable insulin therapy for those with type 1 diabetes: the reasons for this are speculative, and may include the cost of the therapy which led to prudence rather than profligacy in its use, and concerns that to use it widely may lead to side effects from the overload of the system with a greater number of foreign proteins regularly being injected.
(194) A particularly striking example of increased prophylaxis and its effects on consumption is its enthusiastic adoption by Dr Aronstam at Treloar’s, where although there were in general no treatment policies adopted it became a policy to encourage prophylaxis even where pupils themselves would have preferred not to have it. See chapter on Treloar’s.
(195) Though as late as January 1980 at a meeting of the haemophilia reference centre directors the matter of “cryoprecipitate versus factor VIII concentrates for home therapy had been discussed at considerable length and the Reference Centre Directors had agreed that factor VIII concentrates were preferred for home therapy.” The words are those Professor Bloom used to answer a question raised by Professor Geoffrey Savidge: Minutes of Haemophilia Reference Centre Directors meeting 22 September 1980 p11 HCDO0000406
(196) Expert Report to the Infected Blood Inquiry: Bleeding Disorders and Blood Disorders January 2020 p15 EXPG0000002
(197) Factor Eight Inhibitor Bypassing Activity. Inhibitors can develop in people with Haemophilia B but are much less common than with Haemophilia A.
(198) FEIBA was manufactured by Immuno, Autoplex by Travenol. Both were blood products, with the same or similar risks as concentrates.
(199) Expert Report to the Infected Blood Inquiry: Bleeding Disorders and Blood Disorders January 2020 p20, p24 EXPG0000002
(200) Manucci et al 1-Deamino-8-Arginine Vasopressin: A New Pharmacological Approach to the Management of Haemophilia and Von Willebrand’s Disease The Lancet 23 April 1977 p1 PRSE0000638
(201) For more detail see the section headed Von Willebrand disorder in the chapter Haemophilia Centres: Policies and Practice.
(202) For a moving description of this in the words of a person with haemophilia, see the evidence of an anonymous witness: ANON Transcript 14 June 2019 pp10-12 INQY1000020
(203) Dr Brian Colvin in his evidence described an unwillingness for established clinicians to accept that Factor 8 might be flawed: he called the attitude “wishful thinking”. Dr Brian Colvin Transcript 6 October 2020 pp49-52, p132 INQY1000061, Dr Brian Colvin Transcript 7 October 2020 p20 INQY1000062
(204) Though it is now well recognised that most treatments will carry some risk, and the issue is one of balance. The patient’s assessment of that balance is of critical importance.
(205) For example, the risk that even “white” asbestos may give rise to terminal cancer is of such a magnitude as to lead to its use and importation being banned, despite the extremely useful qualities of asbestos as a building and insulating material and the difficulty of finding an adequate substitute. It is thought to be of lower risk than “brown” or “blue” asbestos, and the risks may not materialise in disease for decades – but the risk is still of sufficient magnitude. See the chapter on Risk.
(206) The Expert Report to the Inquiry on Medical Ethics and the evidence of those experts given orally establishes this. There are exceptions where a patient is incapable of taking such a decision, whether because the patient lacks capacity, or they need emergency treatment and to seek active consent is unrealistic – an example might be a patient who is unconscious. Expert Report to the Infected Blood Inquiry: Medical Ethics April 2020 INQY0000241, Medical Ethics Expert Panel Transcript 26 January 2021 INQY1000090, Medical Ethics Expert Panel Transcript 27 January 2021 pp2-8 INQY1000091. See the chapter on Consent.
(207) A clear liquid containing white blood cells that helps to clean the tissues of the body and helps to prevent infections from spreading.
(208) Ministry of Health Homologous Serum Jaundice: Memorandum Prepared by Medical Officers of the Ministry of Health The Lancet 16 January 1943 p1 NHBT0000091_011
(209) So called because of the yellowing of the skin, itself a consequence of excess bilirubin in the blood, and a clear sign that the liver is not functioning as it should. It indicates at least a transient, and potentially a chronic, inflammation of the liver: hepatitis.
(210) The report in 1923 that a virus was a probable consequence of vaccination was made by Alfred Flaum in Sweden: the outbreak he reported was not following vaccination, but the taking of daily blood tests with lancets. However, the breaking of the skin with a type of needle, used from person to person, was essentially the same process as involved in vaccination. Thomas et al Mortality and Morbidity Among Military Personnel and Civilians During the 1930s and World War II From Transmission of Hepatitis During Yellow Fever Vaccination: Systematic Review American Journal of Public Health March 2013 p7 RLIT0001238. Further, in 1937 Findlay and MacCallum noted 48 cases of jaundice following vaccination for yellow fever: Findlay and MacCallum Note on Acute Hepatitis and Yellow Fever Immunization Transactions of the Royal Society of Tropical Medicine and Hygiene November 1937 RLIT0002331. They were convinced it was not from the yellow fever virus itself. Sawyer et al Jaundice in Army Personnel in the Western Region of the United States and its Relation to Vaccination Against Yellow Fever American Journal of Hygiene 26 November 1943 p5 RLIT0000209. In the same year, “several people … died of acute hepatic necrosis following an injection of pooled plasma for measles prophylaxis.” Dodsworth Blood transfusion services in the UK Journal of the Royal College of Physicians of London September/October 1996 p6 RCPH0000448. See also: Propert Letter to the Editor on Hepatitis after Prophylactic Serum British Medical Journal 1938 RLIT0002221; reporting the development of hepatitis after the injection of measles convalescent serum into children.
(211) Sawyer et al Jaundice in Army Personnel in the Western Region of the United States and its Relation to Vaccination Against Yellow Fever American Journal of Hygiene 26 November 1943 pp69-70 RLIT0000209
(212) Hepatitis Following Injection of Measles Serum (Human) 29 June 1942 DHSC0100008_008
(213) The significance of this phrase is considered in the chapter on Role of Government: Response to Risk.
(214) Letter from Senior Medical Officer to Dr Panton 4 August 1942 DHSC0100008_003
(215) Note on Emergency Blood Transfusion Service meeting 1 December 1942 DHSC0100008_024
(216) ie injection or transfusion.
(217) Homologous Serum Jaundice2 December 1942 p1 DHSC0100008_020. Necrosis is cellular death, leading to the death of tissues.
(218) Because it was mainly carried in the part of the blood – the serum – which was not that part which consisted of red blood cells. It was nonetheless recognised by the World Health Organization (“WHO”) Expert Committee reporting in 1952 that though it was convenient to use the term, the virus is found in whole blood and certain of its derivatives and not merely in the serum. Expert Committee on Hepatitis First Report March 1953 p17 RLIT0000215
(219) Bradley et al An Episode of ‘Homologous Serum Jaundice’ British Medical Journal 26 August 1944 DHSC0100008_148. The risk was regarded as sufficiently serious for the Medical Research Council (“MRC”), which then had responsibility for the blood transfusion service, to set up a sub-committee in 1945 dealing solely with post-transfusion jaundice. Note from Dr Panton to Dr Bradley 15 February 1945 DHSC0100008_082, Minutes of Subcommittee on Post-Transfusion Hepatitis meeting 23 May 1945 DHSC0100008_144. It had already been described in The Lancet of 16 January 1943 as “of major importance”, and that “any doubt as to the reality of the association is removed by the frequency with which hepatitis has followed the injection of human blood products. The probability that further cases will occur, particularly after transfusion, must be faced.” Ministry of Health Homologous Serum Jaundice: Memorandum Prepared by Medical Officers of the Ministry of Health The Lancet 16 January 1943 p6 NHBT0000091_011
(220) In June 1944 a memorandum to the MRC Jaundice Committee on Administration and Field Aspects submitted that hepatitis caused by serum transfusion after long intervals was“beyond doubt”. Memo from W Bradley to MRC Jaundice Committee on Administration and Field Aspects20 June 1944 p1 DHSC0100008_051. It was also reported that it was advisable to restrict the size of pools from which serum was to be drawn and that individuals should preferably be transfused from one pool only.
(221) Truelove et al A Documentary Study of Jaundice Associated with Syphilis Treatment and Blood Transfusion British Journal of Social Medicine January 1947 p10 RLIT0000211
(222) In 1946 the Royal Society of Medicine was told that very large pools of plasma were not considered safe: patients should have no more than two or three sera to reduce the risk of jaundice. MacCallum Homologous Serum Hepatitis Proceedings of the Royal Society of Medicine August 1946 p6 DHSC0100008_254. In 1947, Dr William d’A Maycock (consultant advisor to the Ministry of Health on blood transfusion) was concerned that a legal case – in which relatives of a lady who had died of liver failure 14 weeks after being transfused with plasma were claiming compensation from the Ministry of Health – might cause the production and issue of plasma to be stopped. The medical evidence was that “transfusion of plasma carries a definite risk of jaundice, sometimes fatal” and the coroner had found death to be misadventure. Memo from Dr Maycock 2 December 1947 DHSC0100010_012, Memo from Dr Maycock 19 December 1947 DHSC0100010_021, Copy of Post-Mortem Report 3 August 1946 DHSC0100010_024
(223) Letter from Dr Drummond to Dr Maycock 6 January 1950 DHSC0100010_405, Mollison Blood Transfusion in Clinical Medicine September1951 p179 RLIT0001567
(224) Drummond et al Homologous Serum Jaundice After Transfusion of Whole Blood, Dried Small-Pool Plasma, Dried Irradiated Plasma and Kaolin-Treated Filtered Liquid Plasma The Lancet 26 June 1954 p1 RLIT0000058
(225) Letter from Dr Maycock to Dr Robb-Smith 19 August 1946 DHSC0100008_190. The particular danger he had in mind was that of hepatitis. Note from Dr Maycock to Miss Long 22 August 1946 DHSC0100008_191. The need to tell patients they were at risk was advised by solicitors at the time. Letter from J H Keidan Solicitors to Miss Long 29 August 1946 DHSC0100008_192
(226) This “important hazard of blood transfusion” was said to be “not as widely appreciated as it should be”. Transmission of Disease by Blood Transfusion British Medical Journal 20 August 1966 RLIT0001219. In the days before plastic bags became commonplace for blood, glass bottles were used.
(227) Titmuss The Gift Relationship 1970 pp145-147 HSOC0019917
(228) ie from another human being, as opposed to from some other species.
(229) Memo from Scottish National Blood Transfusion Association regarding Hospital Blood Transfusion Arrangements and the Supply of Blood Products in Clinical Use 16 December 1964 p3 PRSE0000157
(230) This is intended to refer to a marker specific to serum hepatitis: there were some markers which were known to show liver inflammation, but they were not in themselves diagnostic of this cause.
(231) Expert Committee on Hepatitis First Report March 1953 pp8-9 RLIT0000215. The WHO Expert Committee on Hepatitis had as a member Dr Fred MacCallum, director of the Virus Reference Laboratory of the UK’s Public Health Laboratory Service based in London; and it noted the valuable input of Dr Maycock, who was effectively in charge of the blood transfusion service in England and Wales. Given the involvement of these two men, together with the facts that Dr MacCallum was the rapporteur for the discussions, that the initial discussions were mimeographed (ie duplicated by means of a stencil duplicator, a principal form of mass distribution before photocopying) and printed in March 1953, it is to be inferred that those responsible for the blood transfusion service and the production of blood products in the UK were well aware of the Expert Committee’s stance.
(232) Expert Committee on Hepatitis First Report March 1953 pp18-21 RLIT0000215
(233) A and Others v National Blood Authority Judgment 26 March 2001 paras 9-10 PRSE0003333. See the chapter on Hepatitis C Surrogate Screening.
(234) The compelling point was made in the World in Action documentary, Blood Money, screened on 1 December 1975, that the only reason the “down-and-outs” featured in the programme went to a blood centre to give plasma was to get money for doing so: how likely were they to give honest answers to questions about their lifestyle and state of health if the result would be that they were sent away with nothing? World in Action Blood Money Transcript 1 and 8 December 1975 pp4-15 PRSE0004591
(235) Nonetheless, it would still have to be recognised that a voluntary donor might not realise that they carried an infection, or might play it down as being irrelevant to whether their donation was a good one: selection of appropriate donors and screening with appropriate care were both needed, and both were implied by the WHO recommendations. See the chapter on Response to Risk by the Blood Services.
(236) Feinstone et al Hepatitis A: Detection by Immune Electron Microscopy of a Viruslike Antigen Associated with Acute Illness Science 26 February 1973 RLIT0002274
(237) An antigen is a molecular structure on the outside of a pathogen, to which an antibody can bind and neutralise the pathogen. The presence of antigens in the body normally triggers an immune response. It was known as “the Australian antigen” because it was first revealed in the blood of an Aboriginal Australian person. Blumberg et al A “New” Antigen in Leukemia Sera Journal of the American Medical Association 15 February 1965 PRSE0001518
(238) Blumberg et al A Serum Antigen (Australia Antigen) in Down’s Syndrome, Leukemia, and Hepatitis Annals of Internal Medicine May 1967 PRSE0000705
(239) National Health Service Revised Report of the Advisory Group on Testing for the Presence of Australia (Hepatitis Associated) Antigen and Its Antibody pp4-5 CBLA0000869
(240) National Health Service Revised Report of the Advisory Group on Testing for the Presence of Australia (Hepatitis Associated) Antigen and Its Antibody p12 CBLA0000869, Memo from DHSS regarding Australia (Hepatitis Associated) Antigen July 1971 DHSC0100004_230, Hansard written answer on Serum Hepatitis 19 July 1971 DHSC0000947
(241) Minutes of Regional Transfusion Directors meeting 14 July 1971 pp7-8 NHBT0016130
(242) Minutes of Regional Transfusion Directors meeting 10 January 1973 pp7-8 NHBT0016114. Immunoelectrophoresis was followed by counter electrophoresis, which was a slight improvement but no more, and then in around 1975 by radioimmunoassay testing. The accuracy of this test was itself refined over the years which followed. Cash Principles of Effective and Safe Transfusion Proceedings of the Royal Society of Edinburgh 1972 pp6-8 PRSE0002637, Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine 1996 pp37-38 NHBT0000028
(243) Scottish National Blood Transfusion Association Report, Statistical Summary and Accounts for Year ended 31 March 1972 p4 SCGV0000064_046. See also: Advisory Group on Testing for the Presence of Hepatitis Associated Antigen and its Antibody Current Arrangements in the Blood Transfusion Service in Scotland 29 December 1970 BNOR0000450_032
(244) Expert Report to the Infected Blood Inquiry: Virology (Hepatitis Supplementary) December 2022 p6 EXPG0000131
(245) A World Health Organization Scientific Group in 1973 reported: “The present widely employed techniques for detecting hepatitis B antigen in blood are thought to be capable of preventing approximately 30% of cases of post-transfusion hepatitis.” World Health Organization Technical Report Series Viral Hepatitis: Report of a WHO Scientific Group 1973 p17 SCGV0000204_073. In 1975, radioimmunological assay began to be used (“RIA”, or AusRia – the “Aus”’ prefix recognising that it was the “Australia Antigen” which was being searched for) with greater sensitivity, though still missing around one third of infections, and further refinements followed into the early 1980s. Second Report of the Advisory Group on Testing for the Presence of Hepatitis B Surface Antigen and its Antibody September 1975 p6 CBLA0000313. It was not until 1985 that the Blood Products Laboratory noted that for the first year since Hepatitis B testing had first been carried out none of the five-litre plasma pools screened for Hepatitis B at regional transfusion centres and dispatched to the Blood Products Laboratory had tested positive for Hepatitis B. Blood Products Laboratory Background and Current Information for Members of the Central Blood Laboratories Authority June 1985 p202 CBLA0002201
(246) This part of the story is concerned with Hepatitis B. There was further reason to consider ALT testing to reduce the risk of transfusing what later became known as Hepatitis C, during the 1980s. This is dealt with in the chapter on Hepatitis C Surrogate Screening in detail but the headline message is the same: ALT screening of all donations was never adopted in the UK, though it was in Germany and Italy by 1970. A and Others v National Blood Authority Judgment 26 March 2001 paras 9-10 PRSE0003333
(247) Titmuss The Gift Relationship 1970 HSOC0019917, New York Times Seven Books of Special Significance Published in 1971 5 December 1971 RLIT0002391
(248) Lord David Owen Transcript 22 September 2020 p25 INQY1000055. He was, as Dr Owen, Parliamentary Under-Secretary and then Minister of State in the Department of Health and Social Security 1974-1976. If he is right about that then any doctor would be aware of a significantly increased risk of serious disease being transmitted to recipients of blood and blood products, because that subject is addressed centrally in the original Chapter 8 of the book “Is the Gift a Good One?” and no one who read that chapter could have remained unaware of it. Though the observation is almost certainly an overstatement, a substantial number of doctors would have read it or been aware of its central themes: and it led to a view held firmly by almost all relevant clinicians, and by the Haemophilia Society, that domestic product (and domestic blood) was much safer than product supplied commercially from the US. The sole basis for thinking the latter comparatively unsafe is the greater likelihood of it transmitting viruses to any recipient. The central focus was on hepatitis viruses, but it was generally recognised that any “foreign” virus was more likely to be transmitted by a product whose raw material came from that foreign region than it was by a domestic product, made from a population where “foreign” viruses were less in circulation, if not actually absent.
(249) Such as in Germany, Switzerland and Austria.
(250) This is a very general statement. Though accurate in as far as it goes, it must not be thought that what is said holds true for each and every pharmaceutical company viewed separately. It lumps pharmaceutical companies together as though they all operated in the same way. They did not. They were in many respects similar, but some obtained their source plasma from their own plasma centres, not all did so from prisons, and their policies as to sourcing plasma did vary over time. See the chapter on Pharmaceutical Companies for greater detail.
(251) Extract from Hospital Week American Hospital Association 10 March 1972 DHSC0100024_079. The original of a report of this was “returned” to the Chief Medical Officer (“CMO”) (in the UK) on 29 March 1972, so it is clear that those responsible for blood services and health policy in the UK knew of US views.
(252) Titmuss The Gift Relationship 1970 pp142-157 HSOC0019917
(253) Garrott Allen The Epidemiology of Posttransfusion Hepatitis: Basic Blood and Plasma Tabulations 1972PRSE0003483. In the publication, he wrote: “The risk of serum hepatitis from transfusions derived from prison and Skid Row populations is at least 10 times that from the use of volunteer donors. For every 100 patients receiving a single transfusion, the attack rate is 0.3 percent when the donor is the conventional family man or volunteer and 3.2 percent when the donor is from a prison or Skid Row population.”
(254) Together with other authors, he concluded that those who received blood from paid donors had a rate of hepatitis infection of seven to ten times greater than seen in those who had had volunteer blood: Garrott Allen et al Blood Transfusions and Serum Hepatitis Annals of Surgery September 1959 RLIT0000063
(255) Garrott Allen Post-Transfusion Hepatitis: A Serious Clinical Problem California Medicine April 1966 p1 RLIT0000217. In the article, he wrote that: “The risk of serum hepatitis from transfusions derived from prison and Skid row populations is at least 10 times that from the use of volunteer donors.” As supporting his striking “10 times” finding, the article cited: Mirick et al Modification of post-transfusion hepatitis by gamma globulin New England Journal of Medicine 8 July 1965 CGRA0000980 and Mosley The Surveillance of Transfusion-Associated Viral Hepatitis Journal of the American Medical Association 20 September 1965 RLIT0000066. He commented that “the most practical methods of reducing the hazard of serum hepatitis from blood are to limit the use of blood by giving one transfusion instead of two, two instead of three etc., and especially by excluding, if possible, all prison and Skid Row donors.” (p1 RLIT0000217). In September 1966 he said in The Advantages of the Single Transfusion that 90% of post-transfusion hepatitis could be traced to the use of commercial or prison blood. Garrott Allen The Advantages of the Single Transfusion Annals of Surgery September 1966 p5 RLIT0000218. In 1970, in Commercially Obtained Blood and Serum Hepatitis, he showed that the hepatitis risk of commercial blood was markedly higher than that of blood from unpaid donors. Garrott Allen Commercially Obtained Blood and Serum Hepatitis Surgery, Gynecology and Obstetrics August 1970 RLIT0002180. See also: Garrott Allen Our Commercial Blood Program and Serum Hepatitis Annals of Surgery November 1970 RLIT0002197. Nor was he a lone voice; see for example: Walsh et al Posttransfusion Hepatitis After Open-Heart Operations Journal of the American Medical Association January 1970 RLIT0000073
(256) Garrott Allen Post-Transfusion Hepatitis California Medicine April 1971 RLIT0000076
(257) Viral infection is not, of course, the only cause of hepatitis. It was reasonable at that stage to conclude that it was probably one virus – the principle of scientific economy argues that where there is one obvious cause of an event you do not generally need to go looking for an alternative one; and although it was known that what was called “infectious hepatitis” could sometimes be transmitted by blood, it was recognised that it was usually transmitted through the oral-faecal route, and arose as a result of environmental conditions. It was not an obvious cause of “serum hepatitis” which was thought to give rise to post-transfusion hepatitis.
(258) Report of the Advisory Group on Testing for the Presence of Australia (Hepatitis-Associated) Antigen and its Antibody paras 6-8 PRSE0000190, which was distributed to Regional Health Boards in June 1971. Memo from Mr B Gidden to the Secretaries of Regional Hospital Boards 20 June 1971 DHSC0100004_227
(259) This did not in fact happen as a matter of routine across the board in respect of whole blood until 1972. Minutes of Regional Transfusion Directors meeting 10 January 1973 pp7-8 NHBT0016114. A paper by Dr Rosemary Biggs published in 1974 dealt with cases which had occurred between 1969 and 1971. Of over 1,800 patients whose cases were considered, 302 had been tested by a range of different tests, none of which are described more closely, for the presence of Australia antigen. Biggs Jaundice and Antibodies Directed against Factors VIII and IX in Patients Treated for Haemophilia or Christmas Disease in the United Kingdom British Journal of Haematology 1974 HCDO0000581. This indicates the relative lack of testing until around 1972.
(260) They lacked sensitivity. Around two-thirds of viral infections were not identified when first used. A World Health Organization Scientific Group in 1973 reported: “The present widely employed techniques for detecting hepatitis B antigen in blood are thought to be capable of preventing approximately 30% of cases of post-transfusion hepatitis.” World Health Organization Technical Report Series Viral Hepatitis: Report of a WHO Scientific Group 1973 p17 SCGV0000204_073. In 1975, radioimmunological assay began to be used (“RIA”) with greater sensitivity, though still missing around one third of infections, and further refinements followed in the early 1980s. Second Report of the Advisory Group on Testing for the Presence of Hepatitis B Surface Antigen and its Antibody September 1975 p6 CBLA0000313. See also: Alter et al Clinical and serological analysis of transfusion-associated hepatitis The Lancet 1 November 1975 p1 PRSE0001172. Dr Harvey Alter and his colleagues said: “the attainment of hepatitis-free blood-transfusions has been a frustratingly slow, but progressively realistic goal.”
(261) In 1972, Dr Harvey Alter and others in Posttransfusion Hepatitis After Exclusion of Commercial and Hepatitis B Antigen-Positive Donors not only showed that the risk of hepatitis from commercial blood was markedly higher than that from donations by voluntary donors, but also that Hepatitis B did not account for all the post-transfusion hepatitis he had discovered. Alter et al Posttransfusion Hepatitis After Exclusion of Commercial and Hepatitis B Antigen-Positive Donors Annals of Internal Medicine November 1972 PRSE0001521. This article later featured in the citation of Dr Alter when he was awarded the Nobel Prize in 2020 for his work in identifying Hepatitis C. In the same year, Dr George Grady and others in Risk of Posttransfusion Hepatitis in the United States A Prospective Cooperative Study reported on the National Transfusion Hepatitis Study in the US, noting (but not highlighting) that those cases of hepatitis with which Hepatitis B antigen was associated accounted for around 60% of the cases of post-transfusion hepatitis which had occurred. Grady et al Risk of Posttransfusion Hepatitis in the United States: A Prospective Cooperative Study Journal of the American Medical Association 1 May 1972 CGRA0000957
(262) Dr Alter observed that: “Lastly, it is important to emphasize that the impact of HBAg testing on posttransfusion hepatitis is minimal when compared with the potential impact of eliminating the use of commercial blood. By far, thesingle most significant measure for the reduction of posttransfusion hepatitis is the total exclusion of the commercial donor.” Emphasis added. Alter et al The Ausria Test: Critical Evaluation of Sensitivity and Specificity Blood 1973 RLIT0002022
(263) Prince et al Long-Incubation Post-Transfusion Hepatitis without Serological Evidence of Exposure to Hepatitis-B Virus The Lancet 3 August 1974PRSE0001431
(264) See Acute Viral Hepatitis B: CDR Reports 1975-79 9 April 1982 MPNI0000052_002. See also the chapter on Public Health for the Rosenheim Committee’s work in response to hepatitis outbreaks in renal units.
(265) A common school of thought seems to have been that in some way NANBH was new, or newly realised, around 1974/5 and thereafter. In reality, the position was as Dr Jay Hoofnagle and others described it in Transmission of Non-A, Non-B Hepatitis: “Undoubtedly, what was once referred to as ‘serum hepatitis’ included both type B and non-A, non-B hepatitis.” He was plainly right. What was new was that the evidence revealed that serum hepatitis had these two major components, and not just one. It ought to have followed logically that the long-term consequences of serum hepatitis, which were well established, could have been due to either component part, and that NANBH could not be assumed to be the insignificant or mild part in respect of these long-term consequences without clear evidence that such was the case. This evidence could only have come from follow-up studies capable of showing if it truly was. Until that evidence was available, the working assumption ought to have been that it was just as much a cause of these consequences as was the component part of serum hepatitis now known as Hepatitis B. As it happened, that evidence could never have been forthcoming, since the reality is as we now know it. Hoofnagle et al Transmission of Non-A, Non-B Hepatitis Annals of Internal Medicine July 1977 p6 RLIT0000228
(266) Of England. Scotland, Wales and Northern Ireland had their own CMOs.
(267) Letter from Dr Garrott Allen to Dr Maycock 6 January 1975 CBLA0000249
(268) World Health Organization, World Health Assembly Resolution 28.72 Utilization & Supply of Human Blood & Blood Products May 1975 PRSE0003476
(269) World in Action: Blood Money Part 1 1 December 1975 MDIA0000113, World in Action: Blood Money Part 2 8 December 1975 MDIA0000114
(270) She concluded her letter by saying: “In this country we have pioneered this treatment, we have the personnel who know how to make the products, we could easily have enough plasma to serve as starting material. It would seem to me a great pity if we cannot make our own material in this country for lack of the organisation, apparatus and buildings in which to work. The purchase of the finished products in the United States will undoubtedly be very costly … Surely it would be less costly to us to do everything to expedite the manufacture of these fractions in England and in particular to accelerate as much as possible the new fractionation buildings at Elstree and in Edinburgh. I feel that it is perhaps time to try to reassess the quantities of these products that might be needed and to try and work out an emergency plan to try and meet the need.” Letter from Dr Biggs to Dr George Godber 22 August 1967 DHSC0100025_062. Lord Owen in his evidence referred to Dr Biggs as the authoritative voice on haemophilia treatment. Lord David Owen Transcript 22 September 2020 INQY1000055
(271) “Pledge” was the word he used in evidence to describe the commitment made and repeated to Parliament. Lord David Owen Transcript 22 September 2020 pp56-57, p114 INQY1000055
(272) A distinction is to be drawn between Factor 9 products, in which domestic supply was close to achieving self-sufficiency, and Factor 8 products, as to which the Blood Products Laboratory and the Protein Fractionation Centre produced, in general, somewhere between one third and one half of an amount sufficient to meet demand – except in Scotland, where it rapidly became sufficient both for Scotland and Northern Ireland, though some purchasing centres in Scotland (such as Yorkhill, Glasgow, for a while) bought commercial product in preference (see the chapters on Self-Sufficiency and on Haemophilia Centres: Policies and Practice for more detail).
(273) Nearly 20 years after Dr Biggs’ clarion call in 1967.
(274) The distinction between the way in which “acute” and “chronic” are used to characterise infectious disease in medicine – where they denote periods of time since first infection – and in popular understanding – where they denote different levels of suffering – is critical to understanding many of the medical articles referred to in the text.
(275) Dr Brian Colvin Transcript 6 October 2020 p49, p51, pp132-133 INQY1000061
(276) Two liver enzymes, the presence of which at high levels indicates a breakdown of liver cells.
(277) More than one witness recounted having known of a patient who died as a result of biopsy. Though the report is anecdotal, and may well reflect a single case, it nonetheless emphasises the risk of the procedure.
(278) Which there was not.
(279) In extent and prevalence: “major” used here does not attempt to categorise the symptoms and consequences of NANBH which emerged more clearly over time.
(280) In terms of numbers of infections.
(281) Care has to be taken in reading medical articles too casually, and focussing upon descriptions of acute disease, where there is a greater case for thinking Hepatitis B more serious than NANBH, rather than chronicity where it was unknown which was the major cause and it could not be assumed.
(282) Mannucci et al Asymptomatic liver disease in haemophiliacs Journal of Clinical Pathology 1975 p1 PRSE0000240
(283) Purcell et al Non-A, Non-B Hepatitis Yale Journal of Biology and Medicine 26 February 1976 p4 PRSE0000381. The article was drawing attention to the fact that it was recognised that NANBH was likely to be less severe in the first six months after infection (the acute phase), but that did not have any implication for those infections which became chronic (ie lasted for over six months).
(284) Hoofnagle et al The prevalence of hepatitis B surface antigen in commercially prepared plasma products Journal of Laboratory and Clinical Medicine July 1976 p8 DHSC0003621_026
(285) “Seven cases of non-B hepatitis and four of hepatitis B occurred within 6 months of the first use of this product. Two patients contracted both types of hepatitis; thus nine patients became ill out of a total of twenty regularly seen at the centre, eighteen of whom received commercial factor-VIII concentrate.” Craske et al An outbreak of hepatitis associated with intravenous injection of Factor-ViIII concentrate The Lancet 2 August 1975 PRSE0001794. It became a notorious outbreak, and few clinicians in the field would have been unaware of it.
(286) Craske and Kirk Hemofil Associated Hepatitis 1974-75 in the United Kingdom: A Retrospective Survey p3, p7 CBLA0000566
(287) Hoofnagle et al Transmission of Non-A, Non-B Hepatitis Annals of Internal Medicine 1 June 1977 RLIT0000228, Knodell et al Development of Chronic Liver Disease After Acute Non-A, Non-B Post-transfusion Hepatitis Gastroenterology 1977 RLIT0000226, Preston et al Percutaneous Liver Biopsy and Chronic Liver Disease in Haemophiliacs The Lancet 16 September 1978 p3 PRSE0003622. Dr Eric Preston and his colleagues thought it reasonable to conclude that “a large portion of haemophiliacs receiving the treatment with factor VIII have important chronic liver disease” and that NANBH “may well be an important factor” in that, since Hepatitis B could be excluded as a cause. See also: Berman et al The Chronic Sequelae of Non-A Non-B Hepatitis Annals of Internal Medicine July 1979 PRSE0001250, which described the progression of NANBH to cirrhosis over time; and Zuckerman Developments in Viral Hepatitis Journal of Medical Virology 1978 p7 NHBT0082903. Professor Arie Zuckerman reviewed earlier studies and noted that cases of NANBH were commonly reported as a cause of persistent liver damage; he summarised: “it seems that this infection may progress to chronic liver disease.”
(288) Hoofnagle et al Transmission of Non-A, Non-B Hepatitis Annals of Internal Medicine July 1977 p6 RLIT0000228
(289) Alter How Frequent is Postransfusion Hepatitis after the Introduction of 3rd Generation Donor Screening for Hepatitis B? What is its Probable Nature? Vox Sanguinis 1977 NHBT0000092_002
(290) Preston et al Percutaneous Liver Biopsy and Chronic Liver Disease in Haemophiliacs The Lancet 16 September 1978 PRSE0003622. Two of the four had micronodular cirrhosis; one chronic lobular hepatitis; and one chronic aggressive hepatitis.
(291) “Ignore” was the word that first came to his mind, though quickly qualified by “not get excited about.” He went on to say it was clear, after that, that it was a really serious evolving clinical problem. Dr Mark Winter Transcript 1 October 2020 p41, p52 INQY1000059. Preston et al Percutaneous Liver Biopsy and Chronic Liver Disease in Haemophiliacs The Lancet 16 September 1978 PRSE0003622. Dr Brian Colvin agreed that the Sheffield paper meant that clinicians could no longer rely on the absence of overt or acute signs of hepatitis as a reliable indicator that NANBH would not develop. Dr Brian Colvin Transcript 6 October 2020 pp64-65 INQY1000061. It was the Sheffield study that convinced Dr Vivian Mitchell that “for some at least haemophilia patients treated with factor concentrates chronic liver disease could be progressive.” Written Statement of Dr Vivian Mitchell para 21 WITN3174003
(292) A mindset had developed in which the risk of hepatitis amongst people with haemophilia as a result of their treatment was regarded dismissively as something which came as a natural adjunct to the condition. It was regarded as inevitable. Two snapshots from the evidence are examples of this. On 10 February 1975 Professor Arthur Bloom wrote to a local GP to say “A small percentage of these freeze dried preparations contain, unavoidably, the virus of serum hepatitis and therefore potentially dangerous to the patient, his relatives etc.” Letter from Professor Bloom to a local GP 10 February 1975 WITN0047002. The first statement makes it clear that Professor Bloom believed in early 1975 (ie after Hepatitis B could be tested for, and when the central risk was now that of NANBH) first that freeze-dried concentrate was potentially dangerous; second that there was real danger of cross infection from its use; and third that this was “unavoidable” if Factor 8 were to be used. The fact that Professor Bloom had in the back of his mind that the question was whether the risk could be avoided or lessened is shown by the fact that he chose to mention unavoidability. The second snapshot comes from the evidence of Alexander Macpherson, headmaster of Lord Mayor Treloar’s College from 1974 onward where he said he had not thought to question the risk that blood products might cause hepatitis amongst his pupils because it was well known when he first came to the school. The sense of his evidence was that because it was there, it was to be accepted. Alexander Macpherson Transcript 24 June 2021 INQY1000134
(293) Dr Mark Winter Transcript 1 October 2020 p39 INQY1000059. This suggests that in his recollection 1976/77 was the date that serious doubts began to surface as to whether the treatment by freeze-dried factor concentrate was actually as beneficial as it once had seemed: yet this is some two years prior to the article by Preston and others. There is compelling evidence it was earlier: the Nobel Prize for Medicine 2020 was awarded to three doctors for their roles in the identification of Hepatitis C. One was Dr Alter. The citation made reference to his work published in January 1972 in which he showed that post-transfusion hepatitis was caused by a virus or viruses other than Hepatitis B in addition to Hepatitis B virus alone. Alter et al Posttransfusion Hepatitis After Exclusion of Commercial and Hepatitis B Antigen-Positive Donors Annals of Internal Medicine November 1972 PRSE0001521
(294) Letter from Dr Dane to Dr Waiter 8 January 1979 DHSC0002191_026
(295) Letter from the Medical Research Council regarding an ad hoc meeting on non-A non-B Hepatitis 7 February 1979 p1 HSOC0011687, Letter from Middlesex Hospital Medical School discussing non-A non-B Hepatitis 8 January 1979 p2 HSOC0011687. In later litigation (A and Others v National Blood Authority), Mr Justice Burton placed considerable weight on this letter as showing the degree of seriousness with which NANBH was regarded. A and Others v National Blood Authority Judgment 26 March 2001 para 100 PRSE0003333
(296) Minutes of Medical Research Council meeting 12 February 1979 PRSE0001960
(297) Minutes of Haemophilia Reference Centre Directors meeting 6 April 1979 HCDO0000403. Professor Ilsley Ingram is minuted as having told the meeting that Immuno were now selling Kryobulin Factor 8 at two prices, the cheaper being made from US plasma. The implication was that it carried a higher risk of hepatitis. He corrected these minutes by letter afterwards, to say that he had spoken to Norman Berry of Immuno who had said “that the American (‘blue’) material was offered for those who wished to take advantage of the lower American price, whereas the European (‘red’) material was still available for those who felt that it carried a lower risk of conveying hepatitis, although the Company regarded both products as equally safe.” Letter from Professor Ingram to Dr Charles Rizza 8 August 1979 LOTH0000012_136. The “safer” material (European origin) was already available, and internal documentation from Immuno AG, the parent company, suggests that it sought to offer the choice though knowing that US plasma was riskier, because it was cheaper, and it considered that “the British market will accept a higher risk of hepatitis for a lower-priced product.” Memo on meeting with Dr Otto Schwarz 25 November 1976 SHPL0001094. It seems that the licensing authority took the same approach as the market, despite the statutory emphasis on safety as a primary concern under the Medicines Act 1968: an application was made to it by Immuno for a variation of the product licence to permit collection from a number of US urban centres, and the licensing authority granted it. Norman Berry had signed the application seeking the variation to allow the plasma which was thought to be less safe (by company officers in Vienna) to be distributed for use. It should be clear there is no evidence that Norman Berry himself knew of the internal discussion.
(298) Letter from Dr Kernoff to Dr Colvin 27 April 1979 p2 BART0002487. The assumption underlying these last few words was that NHS concentrate was less infective than commercial concentrate. It was emphasised in evidence by Dr Winter, Professor Colvin, Professor Christine Lee and echoed by Professor Edward Tuddenham that it was later to be shown that this might not be the case. In a prospective study of 31 patients at the Royal Free Hospital treated for the first time with concentrates between 1978 and 1983, the results indicated that there was approaching a 100% “attack rate” whichever of NHS or commercial concentrate was used. This fitted with theory: if the prevalence of infection in the donor community was 0.3% then by the time 300 or so donations had been pooled it was highly likely that at least one would be infective, and it was understood that one infected donation could render the whole pool infective. The prevalence amongst (paid) donors in the US was undoubtedly significantly higher than that amongst (voluntary, unremunerated) donors in the UK, but though the threshold of infectivity might be easier to reach with the former, the sheer size of the pools made it more than highly likely that NHS as well as commercial products would carry hepatitis infection. However, by the time the study by Dr Kernoff, Professor Lee and others published the results in 1985 it was too late to have any direct effect on treatment patterns. Lee et al Relationships between blood product exposure and immunological abnormalities in English haemophiliacs British Journal of Haematology 1985 p2 PJON0000116_006. By then, products were being produced which had been manufactured in ways which either inactivated or reduced the threat of contracting hepatitis. The assumption in the letter was however the working assumption which clinicians adopted before then: there is ample evidence of this in contemporaneous documentation, as well as in the notable comment made by Professor Bloom which Dr Winter recalled: “The whole virus story, non-A, non-B, HIV, it was commercial. Terrible donor practices. It was not going to happen to Britain with altruistic voluntary donors. This was an American problem. That was view number one”. Dr Mark Winter Transcript 1 October 2020 p137 INQY1000059
(299) Galbraith et al Non-A Non-B Hepatitis Associated with Chronic Liver Disease in a Haemodialysis Unit The Lancet 5 May 1979 p2 PRSE0002202. In the “Discussion” part of the paper it adds: “More and more data point to this [NANBH] as the cause of a substantial proportion of cases of post-transfusion hepatitis negative for HBsAg” (citing Feinstone et al Transfusion-associated hepatitis not due to viral hepatitis type A or B The New England Journal of Medicine 1975 PRSE0000093 and Dienstag et al Non-A, Non-B Post-Transfusion Hepatitis The Lancet 1977 PRSE0002602) and“to its role in the subsequent development of chronic liver disease” (citing Purcell et al Non-A, non-B hepatitis The Yale Journal of Biology and Medicine 1976 PRSE0000381, Knodell et al Development of Chronic Liver Disease after Acute Non-A, Non-B Post-Transfusion Hepatitis: Role of ɣ-globulin prophylaxis in its prevention Gastroenterology 1977 RLIT0000226, Koretz et al Post-transfusion chronic liver disease Gastroenterology in 1976 RLIT0000085, Alter et al Transmissible agent in non-A, non-B hepatitis The Lancet 1978 PRSE0004515).
(300) Annual Report to the Department of Health and Social Security 1978-1979 p7 WITN2050051
(301) NETR Association of Haematologists: Haemophilia Working Party 16 May 1979 p1 BART0000684
(302) The evidence of the Expert Group on Hepatitis (therefore giving the authoritative view on the most up-to-date material) was that roughly 20% will clear spontaneously, depending on the dose and “perhaps on other factors about the person themselves”. (Professor John Dillon) Hepatitis Expert Panel Transcript 26 February 2020 p62 INQY1000052
(303) McGrath et al Liver disease complicating severe haemophilia in childhood Archives of Disease in Childhood 1980 p3 OXUH0001751_003
(304) Forbes and Lowe Unresolved problems in Haemophilia 1982 pp52-53, p58 RLIT0001242. See the chapter on Haemophilia Centres: Policies and Practice.
(305) Professor Howard Thomas Transcript 24 March 2021 pp113-114 INQY1000112
(306) Professor Bloom, Dr Craske, Dr Kernoff, Dr (later Professor) Christopher Ludlam, Professor MacSween, Dr (later Professor) Reuben Mibashan, Dr (later Professor) Francis Preston, Dr Rizza, Dr (later Professor) Thomas, Dr (later Professor) Triger, and Dr (later Professor Sir) James Underwood. See further the chapter on Haemophilia Centres: Policies and Practice.
(307) She added: “In my view, the Department has a moral obligation to ensure that any collaboration with industry does not increase the health hazards, not only to recipients of blood products, but to the community as a whole.” Memo from Dr Walford to John Harley 15 September 1980 p1 WITN0282008
(308) Hansard extract on Blood Products: Imports 24 February 1981 pp19-20 HSOC0008581. Lord Cullen was a Government Whip 1979-1982. There is no briefing or other paper which explains how this statement came to be made.
(309) Minutes of Haemophilia Centre Directors meeting 30 September 1980 p10 PRSE0003946. Professor Bloom then “wondered whether cryoprecipitate would be a better product to use for mild haemophiliacs and von Willebrand’s disease but pointed out that there was a problem over the amount of factor VIII in these materials.”
(310) The fact that knowledge was not limited to those who had attended the Glasgow symposium is borne out by a thesis submitted for a doctorate in 1980 by Dr Anthony Aronstam (of Treloars). Under the heading “Non-A, Non-B hepatitis” he observed “Whatever the nomenclature, this form of hepatitis is as likely to progress to chronic hepatitis as the hepatitis B variety (Spero et al 1978, Seeff et al 1975) and is therefore at least as important.” He concluded: “It appears therefore that at present about half of all severely affected haemophiliacs have persistently abnormal liver function tests and more than half of these will have histological evidence of serious chronic liver disease. This bleak picture has developed in spite of the use of increasingly sophisticated screening tests for HBsAg and donor blood. We now know that blood containing HBsAg diluted to such an extent that the antigen is no longer detectable by R.I.A. may nevertheless induce hepatitis in laboratory animals (Alter et al 1978). We also know that even if HBsAg could be eliminated non-A, non-B hepatitis would still be capable of inducing chronic liver damage (Spero 1978). The addition of a further chronic disabling disease to the lot of patients already suffering from severe haemophilia is a therapeutic catastrophe and will be a major concern to those concerned with the transfusion therapy of haemophiliacs for some time to come.” Aronstam Bleeding Episodes in Severely Affected Adolescent Haemophiliacs and Management with Replacement Therapy 1981 p77, pp79-80 TREL0000517
(311) After 1975, the HBV virus was tested for by radioimmunoassay (“RIA”) techniques. Previously it had been by immunoelectro-osmophoresis (“IEOP”) which was less sensitive.
(312) We know – now – there could have been no such proof, for we know, now, the true consequences of Hepatitis C infection.
(313) Lord Penrose recorded it in his report as being the view generally expressed to him in the evidence before his Inquiry; and made particular reference to Dame Sheila Sherlock’s textbook current at the time which could be taken to say the same. Interestingly, he did not accept the characterisation of NANBH by Dr Kernoff in his letter of 1979 (see above) as a disease with serious long-term consequences, because he thought that science did not know enough to make any such judgement at the time. If so, then the same might be said of the “consensus view” if indeed it did exist – Professor Hay also said that there was a range of views expressed at the time. There is no sense that the uncertainties in these observations were reflected to patients, who repeatedly gave evidence about being reassured by clinicians at the time of the mild nature of NANBH, or that it “was nothing to worry about”. At the very least, they should have been told that there was evidence of liver damage, and that no one really knew where that might lead. Dame Sheila’s textbook Disease of the Liver and Biliary Systems recognised that studies had “shown that patients with acute non-A, non-B hepatitis progress to chronic liver disease”, and whilst it suggested that in relation to NANBH “Clinical progress is towards improvement” it also recognised that “cirrhosis has been reported”. A further (unreferenced) passage in the textbook suggested that the prognosis for chronic NANBH “is, at the moment, uncertain but probably benign.” Sherlock Diseases of the Liver and Biliary System WITN4032021, Sherlock Diseases of the Liver and Biliary System WITN4032022, Sherlock Diseases of the Liver and Biliary System p5 WITN4032023. Professor Franklin thought this reflected the fact that “even Dame Sheila Sherlock didn’t really know what was going to be happening.” Professor Ian Franklin Transcript 27 October 2020 pp152-153 INQY1000068
(314) Professor Charles Hay Transcript 4 November 2020 pp40-43 INQY1000072
(315) Armour Pharmaceutical Plasma Perspectives No1 July 1981 p3 ARMO0000229
(316) Stevens et al Liver disease in haemophiliacs: an overstated problem? British Journal of Haematology 1983PRSE0002564. Of 12 multi-transfused people with haemophilia with persistently abnormal liver function tests, 1 showed evidence of chronic active hepatitis with progression to cirrhosis, and a further 4 some evidence of mild chronic active hepatitis, which according to the article was a lower incidence of severe histological liver damage than many previous reports. It concluded that “the true incidence of severe histological liver abnormality in multitransfused haemophiliacs may be less than previously reported but similar to the more recent results of 115 liver biopsies carried out world wide (Aledort et al 1981) where the incidence of CAH and cirrhosis was 16%.”
(317) Stirling et al Liver function in Edinburgh haemophiliacs: a five-year follow-up 1981 Journal of Clinical Pathology p5 PRSE0000013
(318) Post-transfusion hepatitis British Medical Journal 4 July 1981 p1 PRSE0003110. Another study published in Vox Sanguinis in September 1981 found that hepatitis NANB infection rates for the first treatment with Factor 8 obtained from large plasma pools including paid donors was 40%, whereas the rate was 8% for treatment from smaller pools from Scandinavian volunteer donors. The study concluded that: “It is evident that the risk of transmitting hepatitis non-A, non-B is high with factor VIII preparations obtained from large plasma pools.” Norkrans et al Acute Hepatitis Non-A, Non-B following Administration of Factor VIII Concentrates Vox Sanguinis September 1981 PRSE0001262
(319) Stirling et al Liver function in Edinburgh haemophiliacs: a five-year follow-up 1981 Journal of Clinical Pathology 1981 p5 PRSE0000013. The summary reads: “Liver function was assessed in 38 Edinburgh haemophiliacs. Results before the introduction of NHS intermediate factor VIII concentrate from 1974 onwards were compared with values in 1979. Measurements of serum bile salts in 16 patients as well as conventional liver function tests gave useful evidence of deranged liver function. Deterioration over the five-year follow-up period was seen only in patients on home treatment using large amounts of factor VIII concentrate, and there was no association between cryoprecipitate usage and derangement of liver function.”
(320) Post-transfusion hepatitis British Medical Journal 4 July 1981 p1 PRSE0003110
(321) Holland and Alter Non-A, Non-B Viral Hepatitis Human Pathology December 1981 p5 BPLL0002571_005. They said that “whenever possible, autologous blood and blood products with the lowest risks of hepatitis transmission should be utilized, e.g., the use of single donor plasma or small pools of cryoprecipitated antihemophilic factor in preference to concentrates of clotting factors made from large pools of donors, some of whom are almost certain to be carriers of non-A, non-B hepatitis virus.” Until tests were available specific to NANBH, “nonspecific means of prevention, such as minimal blood usage, an all volunteer blood donor system, recording of implicated donors, and possibly pretransfusion alanine aminotransferase testing, should be utilized.” Holland and Alter Non-A, Non-B Viral Hepatitis Human Pathology December 1981 p5, p8 BPLL0002571_005
(322) The expert report to the Inquiry suggests that what is now called Hepatitis C first emerged around 3,000 years ago. Expert Report to the Infected Blood Inquiry: Hepatitis January 2020 p9 EXPG0000001
(323) CDC Pneumocystis Pneumonia – Los Angeles Morbidity and Mortality Weekly Report 5 June 1981 CGRA0000242, Curran and Jaffe AIDS: the Early Years and CDC’s Response Morbidity and Mortality Weekly Report 7 October 2011 RLIT0002355
(324) CDC Epidemiologic Notes and Reports: Kaposi’s Sarcoma and Pneumocystis Pneumonia Among Homosexual Men – New York City and California Morbidity and Mortality Weekly Report 3 July 1981 OXUH0002849. The CDC’s MMWR was produced weekly and was read in the UK.
(325) CDC Follow-Up on Kaposi’s Sarcoma and Pneumocystis Pneumonia 28 August 1981 PRSE0002908, Masur et al An Outbreak of Community-Acquired Pneumocystis Carinii Pneumonia New England Journal of Medicine 10 December 1981PRSE0004831
(326) The Krever Report 1997 p195 KREV0000001, Evatt The Tragic History of Aids in the Hemophilia Population 1982-1984 Journal of Thrombosis and Haemostasis December 2007 p4 CVHB0000042. The FDA is the regulatory body in the USA.
(327) CDC Epidemiologic Notes and Reports: Pneumocystis carinii Pneumonia among Persons with Hemophilia A Morbidity and Mortality Weekly Report 16 July 1982 PRSE0000523
(328) Deposition of William Srigley 1 May 1995 p79 MULL0000490. This admission was referred to in a supplemental expert witness report of Dr Donald Francis in US HIV Litigation, in which he wrote: “Between June 1981 and July 1982, the number of cases of the new fatal, immunosuppressive disease continued to grow exponentially, and the existence of this condition received great attention in both the popular press and medical literature, making it impossible for defendants not to be aware of the risk of this disease in urban homosexual men. Indeed, a representative of defendant Cutter has testified that he was aware of both the link between homosexuality and AIDS, and the link between homosexuality and hepatitis, at a ‘very early’ date, before July 1982. (Depo. of William Srigley …). On June 11, 1982, the CDC reported not only 281 cases among homosexual or bisexual men, but also 33 cases among intravenous (IV) drug users. The reports of disease among IV drug users also followed the pattern of Hepatitis B distribution, providing further evidence that the new immunosuppressive disease was blood-borne.” Supplemental Expert Witness Report of Donald Francis 2 October 2002 p4 CGRA0000404
(329) Memo from Dr Kingdon to Sharon Northup 5 January 1983 CGRA0000668
(330) Evatt The Tragic History of Aids in the Hemophilia Population 1982-1984 Journal of Thrombosis and Haemostasis December 2007 p4 CVHB0000042
(331) Memo from Dr William Foege to Haemophilia Treatment Centres 9 July 1982 MULL0000840_009. On the same day he wrote to: Cutter Laboratories Inc: Memo from Dr Foege to L Hershberger 9 July 1982 BAYP0004178_003; Armour Pharmaceutical: Memo from Dr Foege to Robert Johnson 9 July 1982 MULL0000625_003; Alpha Therapeutic Corporation: Memo from Dr Foege to Marietta Carr 9 July 1982 MULL0001226_041; the New York Blood Center: Memo from Dr Foege to Dr Kenneth Woods 9 July 1982 MULL0003423_043; and to the National Hemophilia Foundation: Memo from Dr Foege to Charles Carman 9 July 1982 BAYP0004178_003
(332) Memo from Charles Carman to National Hemophilia Foundation chapter presidents 14 July 1982 BAYP0004186_007
(333) Memo from Stan Godfrey to Dr John Holgate 16 July 1982 DHSC0002219_009
(334) CDC Pneumocystis Pneumonia – Los Angeles Morbidity and Mortality Weekly Report 5 June 1981 CGRA0000242
(335) CDC Special Report: Epidemiologic Aspects of the Current Outbreak of Kaposi’s Sarcoma and Opportunistic Infections New England Journal of Medicine 28 January 1982 p5 OXUH0002850
(336) Marx New Disease Baffles Medical Community Science 13 August 1982p2 RLIT0000200, Desforges AIDS and Preventive Treatment in Hemophilia New England Journal of Medicine 13 January 1983 p1 PRSE0002410, Jones et al Altered Immunology in Haemophilia The Lancet 15 January 1983 DHSC0002351_004
(337) Dr Hann was at the time working at the Royal Free Hospital, where he described AIDS becoming a topic of discussion. In 1983 he became head of the haemophilia centre at the Royal Hospital for Sick Children in Yorkhill, Glasgow. Professor Ian Hann Transcript 8 December 2020 pp64-68 INQY1000082
(338) One paper (presented then but published later, in 1983, in line with the practice of the time in respect of important medico-scientific conferences) referred to “an alarming epidemic”; that nationwide across the US half the patients had died; that treatment was affected by the severity and apparent irreversibility of immunodeficiency; and that a causal role for an infectious agent was suggested by the fact that the disease occurred in people in whom infections were readily spread. Blood or bodily secretions appeared to be potential vehicles of infection. Gold et al Acquired Immunodeficiency Syndrome: Infection and Neoplasia in Homosexual Men and Intravenous Drug Addicts Second International Symposium on Infections in the Immunocompromised Host 1983 pp18-26 PRSE0002220, Comments of Professor Ian Hann on excerpts from the 2nd International Symposium of Infections in the Immunocompromised Host PRSE0001858
(339) Written Statement of Professor Ian Hann to the Penrose Inquiry 13 September 2010 p2 PRSE0003578, Professor Ian Hann Transcript 8 December 2020 pp64-66 INQY1000082
(340) Alpha, Cutter, and Baxter International Inc. Supplemental Expert Witness Report of Donald Francis 2 October 2002 p5 CGRA0000404
(341) Summary Report on Open Meeting of PHS Committee on Opportunistic Infections in Patients with Hemophilia pp2-3 BAYP0004205
(342) Marx New Disease Baffles Medical Community Science 13 August 1982p1 RLIT0000200
(343) The Krever Report 1997 p751 KREV0000001
(344) American Association of Blood Banks Hemophilia Foundation Passes AIDS Resolution News Briefs November/December 1982 CBLA0000056_102. It was reported that six cases of haemophiliacs with the disease had now been confirmed by CDC.
(345) Whichever of the two frontrunners as candidates for the cause of AIDS in people with haemophilia (infectious agent; protein/antigen overload) might be favoured, both implicated factor concentrates as a medium of transmission. To understand how a condition spreads it is helpful, but by no means necessary, to know its precise cause.
(346) There is no doubt that the blood services were, or ought to have been, aware of AIDS for some time: but it was not yet discussed in formal meetings. See the chapter on Response to Risk by the Blood Services.
(347) Emphasis added. Memo from Stan Godfrey to Dr John Holgate 16 July 1982 DHSC0002219_009. It was copied to Dr Petronella Clarke, a senior medical officer in the division providing advice on blood transfusion and blood products among other issues. At the time, the DHSS was divided, so far as health was concerned, into two parallel streams – one which had medical expertise and gave medical input, staffed by those with medical qualifications, and the other, which was concerned with policy. The medical stream reported up to the Chief Medical Officer, and through him to government. Written Statement of Diana Walford para D1, paras 2.23-2.24 WITN4461001
(348) Communicable Disease Report 27 August 1982 pp3-4 RLIT0002181
(349) The Acquired Immune Deficiency Syndrome (AIDS) 5 November 1982 pp2-3 CBLA0001653_003
(350) The Observer No defence against gay disease 11 November 1982 MDIA0000010
(351) The risk to people with haemophilia had been realised internationally by this stage. Thus the US National Hemophilia Foundation’s medical director, Dr Louis Aledort, reported to the Congress of the International Societies of Hematology and of Blood Transfusion in Budapest in August 1982 that it was suspected in the US that Factor 8 had resulted in people with haemophilia dying of AIDS, and it was suspected that an infective agent in blood concentrates was the cause. Report of ISH/ISBT Congress Budapest 1982 p33 PRSE0003247. In November 1982 an epidemiologist from the German national institute for infectious diseases (Professor Joanna L’age-Stehr, of the Robert Koch Institute in Berlin) visited the CDC. She reported in the federal health bulletin – the Bundesgesundheitsblatt – that AIDS appeared to be caused by an unknown infectious agent transmitted through blood and blood products. Her report was widely published, being reprinted in the Deutsches Ärzteblatt (German Medical Gazette), distributed to all physicians, on 18 February 1983. In a report on the “German Blood Scandal” written in English it is said of this that: “Professor Joanna L’age-Stehr, was quoted in 1982 with the warning that the import of contaminated blood products from the USA and negligence in the control of infection would lead to an AIDS epidemic in Germany”. (One followed when these warnings were not acted upon). Hubbard German Blood Scandal: as reported in the German-language press Current AIDS Literature January 1994 p1 DHSC0046990_015
(352) CDC Epidemiologic Notes and Reports: Possible Transfusion-Associated Acquired Immune Deficiency Syndrome (AIDS) Morbidity and Mortality Weekly Report 10 December 1982 pp4-6 PRSE0003276, Ammann et al Acquired Immunodeficiency in an infant: possible transmission by means of blood products The Lancet 30 April 1983 PRSE0000317
(353) There was no evidence of this, and it was discounted as unlikely by the clinicians treating the baby. Ammann et al Acquired Immunodeficiency in An Infant: Possible Transmission by Means of Blood Products The Lancet 30 April 1983 pp2-3 PRSE0000317
(354) CDC Epidemiologic Notes and Reports: Possible Transfusion-Associated Acquired Immune Deficiency Syndrome (AIDS) Morbidity and Mortality Weekly Report 10 December 1982 pp4-6 PRSE0003276. In his evidence, Dr Mark Winter (who regularly read the MMWR) described it in this way: “Any clinician looking at this data would have to believe that AIDS was a transmissible disorder and that it could be transmitted by blood and by blood products. It was the only clinical interpretation of the data that was available … So here is a really critical moment. Doctors everywhere now have to believe that AIDS is a transmissible disorder … So at this moment in time, we’re now really believing that there are two major problems with concentrate therapy. Firstly is, the liver disease is much more significant than we thought. Secondly, we’re at the start of something which we are really very concerned about … this new disease sounds like a transmissible disorder”. He thought that “however many alarm bells a human being has, they should all have been ringing at this stage.” Dr Mark Winter Transcript 1 October 2020 p73, pp76-77, p80 INQY1000059
(355) Memo from Edward Cutter to Jack Ryan and others 29 December 1982 CGRA0000434
(356) Written Statement of Sir Joseph Smith para 3.2 WITN5281001
(357) “By the end of 1982 approximately five months after the first report of AIDS in haemophiliacs in USA all UK Haemophilia Centre Directors had been informed of the problem and efforts were being made to obtain up to date information and to set up a system of surveillance of haemophiliacs in UK”. Health Authority Defendants Report by Dr Charles Rizza p131 HCDO0000394. He was secretary general of the UKHCDO and led the Oxford Haemophilia Centre.
(358) Written Statement of Cees Smit paras 84-85 WITN6411001. Cees Smit was editor of the Netherlands Haemophilia Society’s magazine 1971-1998. The Krever Report 1997 pp922-924 KREV0000001
(359) Professor Willem van Aken Lindsay Tribunal Transcript 3 July 2001 p18 LIND0000308. Two of his colleagues had visited the US to learn about AIDS first hand and he had been asked to review a paper, discussed below, for The New England Journal of Medicine about immune abnormalities in people with haemophilia. Cees Smit wrote that on 29 December 1982 the Central Blood Laboratory informed the Netherlands Haemophilia Society. “The impact of AIDS for the hemophilia community became quite clear.” He recalled that the Netherlands Haemophilia Society were informed first, with the haemophilia doctors being informed on 4 January 1983. Smit Surviving hemophilia: A road trip through the world of healthcare 2020 p2 RLIT0002362
(360) Professor Willem van Aken Lindsay Tribunal Transcript 3 July 2001 p20 LIND0000308
(361) CDC Epidemiologic Notes and Reports: Immunodeficiency among Female Sexual Partners of Males with Acquired Immune Deficiency Syndrome (AIDS) – New York Morbidity and Mortality Weekly Report 7 January 1983 pp1-2 RLIT0000232
(362) Letter from Ian Marshall to Professor Arthur Bloom enclosing Alpha Therapeutic UK Ltd press release 16 March 1983 p2 CBLA0000060_067
(363) Desforges AIDS and Preventive Treatment in Haemophilia New England Journal of Medicine 13 January 1983 p2 PRSE0002410. This periodical had wide circulation in UK medical circles: for instance, Dr Winter makes specific reference to it in his evidence, though citing few other journals. Dr Mark Winter Transcript 1 October 2020 pp33-34 INQY1000059
(364) The second article showed that whatever caused AIDS appeared to reduce the number of T4 helper cells in the patient’s immune system. Lederman et al Impaired Cell-Mediated Immunity in Patients with Classic Hemophilia New England Journal of Medicine 13 January 1983 PRSE0004470
(365) Minutes of UK Haemophilia Centre Directors Hepatitis Working Party meeting 19 January 1983 pp3-4 HCDO0000558. Haemophilia doctors – Dr Rizza, Professor Francis Preston from Sheffield, Dr Christopher Ludlam from Edinburgh, Dr Peter Kernoff from the Royal Free and Professor Bloom from Cardiff who chaired the UKHCDO – were present, as was Dr Richard Lane of the Blood Products Laboratory (“BPL”), and Dr Joan Trowell, a hepatologist who worked closely with the Oxford Haemophilia Centre.
(366) Professor Zuckerman was professor of virology at the London School of Hygiene & Tropical Medicine and specialised in viral hepatitis. There are two records of this meeting. The more detailed notes are extensive, and seem to record much of what was said. The notes devote over a page of closely typed A4, consisting of ten paragraphs, to AIDS. Notes of Meeting with Immuno 24 January 1983 PRSE0002647. The other record is written by an attendee from Immuno. It is terse, and does not include much of the same discussion: possibly because Immuno’s main concern was establishing a market for their product which was “hepatitis reduced”. The inference is that the person who compiled the Immuno record chose not to minute the discussion and information about AIDS. Letter from Norman Berry to Dr Kernoff enclosing the minutes of Excelsior Hotel meeting 24 January 1983 RFLT0000050
(367) Notes of Meeting with Immuno 24 January 1983 pp3-4 PRSE0002647. The Immuno record asserts that “it is not known if AIDS is caused by a virus or an attacker inimical to T cells” and says very little more about AIDS. Letter from Norman Berry to Dr Kernoff enclosing the minutes of Excelsior Hotel meeting 24 January 1983 p4 RFLT0000050
(368) Notes of Meeting with Immuno 24 January 1983 pp3-4 PRSE0002647
(369) Notes of Meeting with Immuno 24 January 1983 p4 PRSE0002647, Menitove et al T-Lymphocyte Subpopulations in Patients with Classic Hemophilia Treated with Cryoprecipitate and Lyophilized Concentrates New England Journal of Medicine 13 January 1983 p1 PRSE0001320. This could be suggestive of a developing failure of their immune systems.
(370) Ragni et al Acquired-Immunodeficiency-like Syndrome in Two Haemophiliacs The Lancet 29 January 1983 RLIT0000201
(371) Sattaur AIDS: transfusion patients may be at risk New Scientist 3 February 1983 PRSE0000726
(372) William Check Preventing AIDS transmission: should blood donors be screened? Journal of the American Medical Association 4 February 1983 p1, p3 BAYP0000028_024. The source for the information about the pending licences was Dr Aledort. The implication was that the risk of factor concentrates transmitting the cause of AIDS was sufficiently serious that all the major pharmaceutical companies were prepared to spend significant sums in an attempt to avoid it.
(373) The Krever Report 1997 p855 KREV0000001. Professor L’age-Stehr of the Institute had already reported in the Bundesgesundheitsblatt (the federal health bulletin) that this was the case, following a November 1982 visit to the CDC.
(374) Professor Willem van Aken Lindsay Tribunal Transcript 3 July 2001 pp32-33 LIND0000308. He was reading from advice from January 1983.
(375) The Krever Report 1997 pp922-933 KREV0000001, Cees Smit Contaminated Blood: What did the Netherlands do differently? Factor 8 11 May 2020 JEVA0000279. Cees Smit noted that about 15% of people with severe haemophilia in the Netherlands were infected with HIV (mostly those who had used US factor products), a much lower proportion than in the UK, though higher than in countries which did not import US factor concentrates.
(376) CDC Current Trends Prevention of Acquired Immune Deficiency Syndrome (AIDS): Report of Inter-Agency Recommendations Morbidity and Mortality Weekly Report 4 March 1983 pp1-2 PRSE0001115
(377) Canadian HaemophiliaSociety Medical and Scientific Advisory Committee Reduction of AIDS Risk: Recommendations for Physicians Treating Hemophiliac Patients Canada Diseases Weekly Report 26 March 1983 p1 DHSC0002225_040. The Committee acknowledged that most patients would continue taking factor products, but advised avoiding large doses and prolonged treatment and using immobilisation and splinting.
(378) Professor Willem van Aken Lindsay Tribunal Transcript 3 July 2001 p20 LIND0000308
(379) Memo from Dr John Petricciani to all licensed manufacturers of plasma derivatives 24 March 1983 DHSC0001203. It applied to blood products which were “already known to have a risk of transmitting infectious diseases.” The pharmaceutical companies were requested to inform the Office of Biologics in writing of the procedures they had instituted to comply with the notice. It is plain that the FDA recognised a risk that Factors 8 and 9 might transmit AIDS. This recommendation is sometimes mislabelled a “regulation”, but nonetheless gained prominence in the UK, since it could be seen as giving rise to two classes of blood product – those made from plasma collected before 24 March 1983 (“pre-March plasma”) and those made from plasma collected afterwards. Blood products such as freeze-dried Factor 8 had a long shelf life, and so could be warehoused long before distribution and use – and this gave rise to fears that some of the product made from pre-March plasma might be sold or distributed for use in the UK, despite the fact that there was a greater risk that people selling their plasma at that time carried infections transmissible through blood because of their lifestyles or personal history. See the chapter on Regulation of Commercial Factor Concentrates.
(380) For instance, Lee Stay was investigated at Lord Mayor Treloar Hospital and College where Dr Anthony Aronstam was the lead clinician for signs of AIDS on 10 March 1983: he had had three different commercial concentrates as well as some NHS product. He was not then infected, but did seroconvert after 7 June 1983 and before 6 September 1983. Written Statement of Lee Stay para 20 WITN1541001, Patient annual treatment record of Lee Stay pp3-4 WITN1541004, Patient medical records of Lee Stay pp2-3 WITN1541005. The medical records available from Treloar’s show that testing was a general pattern there. It involved a clinical examination (for evidence of any enlarged lymph nodes, persistent cough, signs of oral thrush, etc) and a biochemical one – blood was tested to determine the T4/T8 cell ratio, in particular, as well as for any hormonal indications. Counsel Presentation on Lord Mayor Treloar’s School and Haemophilia Centre June 2021 p43 INQY0000281. See also: Jones et al Altered Immunology in Haemophilia The Lancet 15 January 1983 DHSC0002351_004, Ludlam et al Disordered Immune Regulation in Haemophiliacs Not Exposed to Commercial Factor VIII The Lancet 28 May 1983 PRSE0001303, Froebel et al Immunological abnormalities in haemophilia: are they caused by American factor VIII concentrate? British Medical Journal 15 October 1983 PRSE0001121, Daly et al AIDS surveillance in haemophilia British Journal of Haematology 1985 GLEW0000677. See also the chapter on Treloar’s.
(381) Dr James Smith commented in a written statement to the Penrose Inquiry that: “I believe that most fractionators thought it likely that AIDS was caused by a blood-borne virus, even before the seminal publication by Montagnier’s group … [which] was taken by transfusionists as strong support for their working hypothesis.” Written Statement of Dr James Smith to the Penrose Inquiry 22 June 2011 p9 PRSE0004045. Dr Luc Montagnier at the Pasteur Institute in Paris reported on 20 May 1983 that he had isolated a virus which was associated with AIDS. He named it LAV (lymphadenopathy-associated virus). Barré-Sinoussi et al Isolation of a T-Lymphotropic Retrovirus from a Patient at Risk for Acquired Immune Deficiency Syndrome (AIDS) Science 20 May 1983 PRSE0004469. Though he was later to be awarded the Nobel Prize for this work, it had limited recognition until after Dr Robert Gallo’s team in the US identified the same virus as the presumptive cause, a year later, and named it HTLV-3. Gallo et al Frequent Detection and Isolation of Cytopathic Retroviruses (HTLV-III) from Patients with AIDS and at Risk for AIDS Science 4 May 1984 PRSE0001131
(382) Letter from Dr Evatt to Professor Bloom 7 March 1983 DHSC0001175
(383) Memo from Dr Lane to Gilbert Mallory 24 March 1983 CBLA0001691, Minutes of Central Blood Laboratories Authority meeting 23 March 1983 p4 CBLA0007769. The action for the DHSS from the Central Blood Laboratories Authority (“CBLA”) meeting was to supply information on the meetings between the DHSS and the US authorities about AIDS but the Inquiry has seen no evidence that this happened.
(384) Memo from Dr Lane to Gilbert Mallory 24 March 1983 CBLA0001691
(385) Acquired Immune Deficiency Syndrome (AIDS) 22 April 1983 p1 CBLA0001697. See the chapter on Viral Inactivation for more detail.
(386) CDC Current Trends Update on Immune Deficiency Syndrome (AIDS) – United States Morbidity and Mortality Weekly Report 24 September 1982 p1 OXUH0002848
(387) Terrence Higgins Trust How it all began p1 RLIT0002227, Letter from Hunter, Burns and Ogg solicitors to Dr Anne Smith 14 June 1983 PRSE0000987
(388) By 31 July 1983, five deaths had been reported to the CDSC. CDSC Surveillance of the acquired immune deficiency syndrome in the United Kingdom January 1982-July 1983 British Medical Journal 6 August 1983 DHSC0002231_019
(389) Horizon – Killer in the Village Transcript 25 April 1983 MDIA0000158. The CBLA had their next meeting two days later and the only action on AIDS was for the DHSS to try to ascertain how many telephone calls had been made to the number given at the end of the Horizon programme. Professor Bloom reported that he had spoken at the Haemophilia Society annual general meeting: “His impression was that haemophiliacs were not greatly concerned about AIDS.” And Dr Gunson reported that the regional transfusion directors had considered “all the American literature” on the subject but did not recommend action – even though high-risk donors had still not been asked to refrain from donating. Minutes of Central Blood Laboratories Authority meeting 27 April 1983 pp3-4 BPLL0003987_002
(390) The Observer Killer disease alert over gay blood donors 1 May 1983 MDIA0000016
(391) Mail on Sunday Hospitals using killer blood 1 May 1983 p1 PRSE0000199. It also quoted Dr (later Professor) Anthony Pinching, an immunologist, as saying “It seems madness that our blood supplies are coming from a country suffering from an epidemic”. Professor Pinching told the Inquiry “I think that this ‘quote’ was a paraphrase of views which I expressed during a much wider, long (c. 1-2 hours) interview about AIDS.” Written Statement of Professor Anthony Pinching para 6.1 WITN7652001
(392) The Guardian US blood products face ban in Aids scare and Killer Disease Baffles Doctors 2 May 1983 DHSC0002351_010. The second article pointed out that the number of known cases doubled every six months. It was “officially an epidemic and the deadliest since swine fever ravaged the US at the end of the First World War.”
(393) Newspaper clippings: Daily Mail Probe on imports of ‘killer blood’ 2 May 1983, Daily Express The tragic disease shrouded in mystery 2 May 1983 MACK0002666_009
(394) Letter from Reverend Alan Tanner to members of the Haemophilia Society 4 May 1983 DHSC0001228. Professor Bloom’s words, in the context of a letter urging that there was little or no risk of contracting AIDS from blood products were, “In addition the importation of licensed blood products has always been strictly monitored and controlled.” The inference the letter invites a reader to draw is that set out in the text: no other interpretation can reasonably be drawn.
(395) The number doubled roughly every six months. CDC Current Trends Update on Immune Deficiency Syndrome (AIDS) – United States Morbidity and Mortality Weekly Report 24 September 1982 p1 OXUH0002848
(396) Unless there was a clear basis to distinguish the general population from people with haemophilia in this.
(397) There is no evidence that there was a live issue whether it was a “proven” or “confirmed” case or not: but if there had been, the choice of words is economical with the truth. If reliance was to be placed on whether every test for AIDS had yet been met, and it was to be suggested that the syndrome had not unequivocally been confirmed, this should at the very least immediately have been followed by recognition that it was strongly suspected that it had, and that such a case had developed in Professor Bloom’s very own unit of a person who had received commercial concentrate. The CDSC reported on 6 May that there was a case of a person with haemophilia in Cardiff who had received factor products and who had AIDS. The report to the CDSC must have come from Professor Bloom’s unit. There is no qualification in the CDSC report – such as use of the words “suspected case”. It is recorded as an actual case. Communicable Disease Report 6 May 1983 PRSE0000353. The information is less clear about the second case, though later it became apparent that there had been a case in Bristol which had not been reported to the Public Health Laboratory Service. The Bristol patient died later that year. Daly and Scott Fatal AIDS in a Haemophiliac in the UK The Lancet 19 November 1983 PRSE0004509, Minutes of Haemophilia Reference Centre Directors meeting 19 September 1983 p4 PRSE0003196. At least two further cases were strongly suspected before 13 July 1983. Treloar’s kept the closest study on people with haemophilia in the UK and their reports to home clinicians at the end of the summer term 1983 included a section on AIDS investigations. Dr Frank Hill at Birmingham Children’s Hospital was told of Joseph Peaty on 29 June 1983: “Clinically he exhibits some of the stigmata of AIDS”, going on to give details. Letter from Dr Mouneer Wassef to Dr Hill 29 June 1983 p1 TREL0000335_020. Joseph Peaty told the Inquiry that it would not be until the next spring, by which time he was 18 years old and had been in a romantic relationship for some months, that he was told in a group of boys that AIDS was a risk and the boys’ blood was going to be tested. He told his mother who rang one of the doctors who reassured her that there was nothing to be concerned about. Joseph Peaty told the Inquiry: “My mother and myself find these events bewildering.” Written Statement of Joseph Peaty paras 268-273, paras 278-279, paras 284-287, para 289 WITN4607001. Dr Morag Chisholm at Southampton Hospital was similarly informed that a pupil exhibited some of the stigmata of AIDS. Letter from Dr Wassef to Dr Chisholm 28 June 1983 TREL0000233_043. Another pupil’s home clinician was told: “Clinically he exhibits one of the stigmata of AIDS in that he has lost 3kg. in body weight.” Letter from Dr Wassef to Dr C Cheetham 7 July 1983 TREL0000240_185. Another boy’s end of term report to his home clinician said: “Clinically he exhibits none of the stigmata of AIDS apart from 5 kg. body weight loss this term” and a palpable lymph node. Letter from Dr Wassef to Dr David Evans 27 June 1983 TREL0000308_065. Another boy’s report said: “Clinically he exhibits none of the stigmata of AIDS apart from 2kg. loss in body weight this term.” Letter from Dr Wassef to Dr Donald Chalmers 27 June 1983 TREL0000317_015. Although Treloar’s was within the Oxford Haemophilia Centre’s supra-region, and Oxford was both its reference centre and where the UKHCDO national database was then located, it does not seem that these findings came to the attention of anyone at Oxford or the CDSC, nor were they explained to the boys and their parents.
(398) There is no direct evidence that Professor Bloom knew of this: but he did attend, or see reports of, international gatherings, and his offering a view as to the German position suggests that he thought others would give credence to what he said, no doubt because he was thought to have a wide understanding of what was happening in Europe. L’Age-Stehr et al AIDS in West Germany The Lancet 10 December 1983 RLIT0000279, The Krever Report 1997 p856 KREV0000001
(399) Though Professor Bloom would not necessarily have known this at the time, ten people in Germany had died of AIDS by this point, and two people in Germany with haemophilia had AIDS. Council of Europe Committee of Experts on Blood Transfusion and Immunohaematology report on AIDS 28 April 1983 p4 DHSC0000717
(400) The Observer had expressed in simple language one of the critical principles of protection of the public from risk – that “incidence” (the number of cases) should not be conflated with “risk” (the number of cases that might yet emerge from the pipeline), and that where a disease takes a long while to show itself it is thus all the more important to take protective steps early. It said (as quoted above in the text): “The disease, characterised by a collapse in the body’s ability to fight infection, is a medical time-bomb for Britain. Although only 15 cases have been reported since it crossed the Atlantic in December 1981, many more people could be harbouring it, for the incubation period is up to three years.” They show that no public health expertise was required to understand the principle – a principle which tragically was never recognised by Professor Bloom in what he had to say in public about AIDS over the coming year, whatever may have been his private views. The Observer Killer disease alert over gay blood donors 1 May 1983 MDIA0000016
(401) Letter from Dr Evatt to Professor Bloom 7 March 1983 DHSC0001175
(402) Notes of meeting with Immuno 24 January 1983 pp3-4 PRSE0002647, Desforges AIDS and Preventative Treatment in Haemophilia New England Journal of Medicine 13 January 1983 PRSE0002410
(403) Minutes of UK Haemophilia Centre Directors Hepatitis Working Party meeting 19 January 1983 p1, pp3-4 HCDO0000558
(404) Letter from Dr Malcolm Liddell to Anon 28 January 1983 WITN0047004, Mrs AT Transcript 30 October 2019 pp84-86 INQY1000047
(405) Haemophilia Treatment Policy Guidelines May 1983 p1 WITN4029002. There is no suggestion that there might be any problem with supplies of cryoprecipitate, nor that it might be inappropriate to use it, the contrary is to be inferred.
(406) Thus in the middle of a period when Professor Bloom was saying publicly that there was no need for any change to therapy, the unit of which he was in charge at Cardiff had changed its approach to what was used for whom and in what circumstances. It is to be inferred that Professor Bloom authorised this and it is difficult to avoid a conclusion that his approach was hypocritical. Haemophilia Treatment Policy Guidelines May 1983 p1 WITN4029002
(407) Letter from Professor Bloom 18 February 1983 CVHB0000002_003. The action was asking patients to take a simple blood test and skin prick test “to identify any predisposing factors to this type of illness in patients suffering from blood coagulation disorders.”
(408) Letter from Reverend Tanner to members of the Haemophilia Society 4 May 1983 DHSC0001228. “Proven” can be a slippery word. As Professor Bloom used it, it may suggest certainty: but it all depends on the standard applied. In all except a few cases proof in our courts is established on the balance of probabilities. Applying this generally applicable standard, the Cardiff case was proved. In any event, even if one puts legalities and common approaches to one side, it must be recognised that the answer to any question as to what standard of proof to apply is that it is that which is appropriate in the context. Where the context is the protection of the public against disease, then to demand proof that a disease is caused by a certain agent (even on a balance of probabilities) is to set too high a bar. Proof that there is a risk at such a level as to require preventative or precautionary action requires less in terms of evidence: and proof that there is a risk at such a level to require at the very least consideration of taking action less still again. Here it is plain that on any standard, apart from proof beyond any doubt, it was proved that AIDS could be caused to a person with haemophilia in the UK as a result of his being given commercial concentrate.
(409) Minutes of Association of Scientific, Technical and Managerial Staffs National Executive Council and Parliamentary Committee meeting 4 May 1983 WITN6914016. It is clear from internal DHSS memos that arguments to this effect were circulating, and the response was to resist them. Memo from John Parker to Janet Walden 3 May 1983 p1 DHSC0001651, Memo from Dr Walford to Dr Ian Field 13 May 1983 DHSC0002227_047
(410) This date appears to be chosen because it was already thought that the incubation period for the first cases to develop AIDS in the US began then, five years earlier. CDC Epidemiologic Notes and Reports Update on Kaposi’s Sarcoma and Opportunistic Infections in Previously Healthy Persons – United States Morbidity and Mortality Weekly Report 11 June 1982 p2 MULL0003761
(411) Letter from Dr Galbraith to Dr Field 9 May 1983 p1 CBLA0000043_040
(412) Then David Watters. The title of his role changed to “general secretary” in 1986.
(413) Letter from David Watters to all members of the Medical Advisory Panel 9 May 1983 BPLL0001351_076. Geoffrey Finsberg was then Parliamentary Under-Secretary at the DHSS.
(414) Minutes of Haemophilia Reference Centre Directors special meeting 13 May 1983 pp2-3 HCDO0000003_008. The word “immense” appears in the final version of the minutes, presumably approved by the chair (Professor Bloom). It does not feature in a record of the meeting made on the same day by Dr Walford of the DHSS, who was present. Memo from Dr Walford to Dr Field 13 May 1983 DHSC0002227_047. Since it adds nothing but hyperbole and emphasis to the conclusion, it was presumably inserted in order to do so.
(415) Memo from Dr Walford to Dr Field 13 May 1983 DHSC0002227_047
(416) People with haemophilia were of course very unlikely to become blood donors: the FDA request was in relation to the first three groups named. As to the “4 Hs”, in a DHSS paper they became six. Dr Keith Fowler of the DHSS, in wording which displays the attitudes of the early 1980s, added “5. ‘Hookers’ (Prostitutes) 6. ‘Housewives’ (Female consorts of [homosexuals and bisexuals and heroin, iv drug abusers]”). Acquired Immune Deficiency Syndrome (AIDS); A New Hazard for Haemophiliacs? July 1983 p2 DHSC0002229_059. The contribution, despite the language used, recognised that anyone – male or female – who had sexual relations with a person in one of the other better recognised risk groups might also unwittingly transmit the cause of AIDS through their blood to others. The DHSS internally thus did not subscribe to what was still a popular view in society, that AIDS was a problem centred on male homosexuality.
(417) Memo from Dr John Petricciani to all licensed manufacturers of plasma derivatives 24 March 1983 DHSC0001203
(418) Leveton et al HIV and the Blood Supply: An Analysis of Crisis Decisionmaking 1995 p106 JREE0000019
(419) Council of Europe Committee of Experts on Blood Transfusion and Immunohaematology report on AIDS 28 April 1983 DHSC0000717
(420) Informal report of Committee of Experts on Blood Transfusion and Immunohaematology meeting 16-19 May 19 May 1983 pp1-2 NHBT0017430
(421) Scottish National Blood Transfusion Service AIDS and Blood Transfusion 24 May 1983 PRSE0000984
(422) Council of Europe Recommendation No R(83)8 23 June 1983 MACK0000307
(423) Leikola AIDS - New Concern for Blood Transfusionists Transfusion International July 1983 p2 PRSE0002301. Professor Juhani Leikola was editor-in-chief of Transfusion International and head of the Blood Programme Department of the League of Red Cross and Red Crescent Societies.
(424) Acquired Immune Deficiency Syndrome (AIDS); A New Hazard For Haemophiliacs? July 1983 pp1-3 DHSC0002229_059
(425) Minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 13 July 1983 p2 ARCH0001710. The first sentence recognised what was now orthodoxy: the second is probably a reference to the thesis advanced by Dr Fowler. It added, considering other possibilities or contributory factors: “Heightened susceptibility may be an important factor, e.g. immunological deficiencies induced by unusual sexual practices or exposure to blood products. Based on the clinical evidence, transmissibility of the supposed agent(s) appears to be low, requiring intimate contact or introduction into the tissues.”
(426) Minutes of Blood Products Advisory Committee meeting 19 July 1983 pp3-4 BAYP0004674. The meeting at which he did so, in Bethesda, Maryland, postdated the meeting of the sub-committee in London which took the decision to recommend that the importation of foreign concentrates should not be suspended. The precise words could not therefore have been in the mind of the members of that sub-committee.
(427) Report of Blood Products Advisory Committee on the Safety and Purity of Plasma Derivatives meeting 19 July 1983 p8 CBLA0000056_215. See also: The Krever Report 1997 p379 KREV0000001
(428) Dr Rodell’s contribution seems startling. (At least one reasonable, if not the only reasonable, way of reading it is to see it as saying “given the size of the pools used to manufacture concentrate, they are all highly likely to be infected with the cause of AIDS, assuming it to be viral: but you can’t ban them all/recall them all, because you’d have nothing left with which to treat people with haemophilia”: or, in other words, “we have allowed the pools to become so big that as a result they have become too big to be allowed to fail – you must just accept the risks of AIDS that comes with them if you want your haemophilia to be treated at all.”) The importance of this for the purposes of analysing whether the decision of the Sub-Committee on 13 July 1983 (see the chapter on Regulation of Commercial Factor Concentrates) was appropriate is firstly that it shows what logic was being adopted by major influencers at the relevant time and secondly makes it surprising both that it was not the source of more substantial contemporaneous public, clinical, administrative and governmental comment at the time. It is surprising that it did not require a speedy rethink of the decision of the Sub-Committee, or its review before it was too late. Given the scale of contact between the US and UK, and the close attention being paid by the DHSS to decisions made by the FDA, what Dr Rodell was saying ought to have been appreciated. Given his position within the pharmaceutical industry, the major pharmaceutical companies must have drawn the conclusion he expressed some time before he did so.
(429) Barré-Sinoussi et al Isolation of a T-Lymphotropic Retrovirus from a Patient at Risk for Acquired Immune Deficiency Syndrome (AIDS) Science 20 May 1983 PRSE0004469. LAV stood for lymphadenopathy-associated virus, later to be shown to be identical to HTLV-3 which was isolated by Dr Gallo a year later, and now known as HIV.
(430) Written Statement of Dr Joseph Smith para 3.2 WITN5281001
(431) Appendix of Medical Research Council Brief on AIDS 24 August 1983 DHSC0002231_031. The document references the San Francisco baby case and adds further evidence. It notes that “the potential for widespread transmission occurs in the large donor pools used in production of fractionated blood products.”
(432) Surveillance of AIDS cases in patients with blood coagulation disorders 10 September 1983 CBLA0001758, Daly and Scott Fatal AIDS in a Haemophiliac in the UK The Lancet 19 November 1983 PRSE0004509, Daly and Scott Fatal AIDS in a Haemophiliac in the UK The Lancet 7 January 1984 MACK0000604_002
(433) The Mail on Sunday The Scandal of Peter Palmer’s Death 2 October 1983 HSOC0016112
(434) Minutes of UKHCDO meeting 17 October 1983 p10 PRSE0004440
(435) Jones Acquired immunodeficiency syndrome, hepatitis, and haemophilia British Medical Journal10 December 1983 p2 HSOC0001285
(436) Curran et al Acquired Immunodeficiency Syndrome (AIDS) Associated with Transfusions New England Journal of Medicine12 January 1984 p5 PRSE0001931
(437) The Krever Report 1997 p204 KREV0000001
(438) See the chapter on Pharmaceutical Companies.
(439) This is how a causal link is often expressed by a scientist taking care to recognise that there may be other causes (eg where one cause masks another), and that where A occurs on occasions where B is seen to happen it does not necessarily mean that A actually causes B: the strength of association, the consistency of one study showing it with another, its specificity, whether there is a temporal connection, and the biological plausibility have also to be considered. Barré-Sinoussi et al Isolation of a T-Lymphotropic Retrovirus from a Patient at Risk for Acquired Immune Deficiency Syndrome (AIDS) Science 20 May 1983 PRSE0004469
(440) Gallo et al Frequent Detection and Isolation of Cytopathic Retroviruses (HTLV-III) from Patients with AIDS and at Risk for AIDS Science 4 May 1984 PRSE0001131
(441) Letter from Dr J McGinnis to colleagues 9 May 1984 p3 DHSC0000583
(442) Weiss Retroviruses linked with AIDS Nature 3 May 1984 BAYP0000026_107
(443) See the chapter on HIV Screening.
(444) Newcastle, Leeds, Nottingham, Cambridge, Birmingham, Oxford, Manchester, Liverpool, Cardiff and (later) Belfast. Hepatitis C: A review of events leading up to the introduction of routine tests for anti-HCV in the UK p21 NHBT0017232
(445) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine Vol 6 1996 p11 NHBT0000028
(446) Hepatitis C: A review of events leading up to the introduction of routine tests for anti-HCV in the UK p22 NHBT0017232
(447) The initial four had been reduced to two.
(448) Pursuant to Sections 11 and 14, and Schedule 3.2, of the 1946 National Health Services Act and the National Health Service (Determination of Regional Hospital Areas) Order 1946 (SI 1946 No 2158).
(449) The Ministry of Health continued to have a role, since meetings of the regional transfusion directors were chaired by the consultant adviser to the Minister of Health and later the Chief Medical Officer (for many years Dr Maycock) and attended by the Ministry of Health. Updated NHSBT Family Tree 6 September 2021 p3 WITN0672007
(450) For most of the period under scrutiny, at Elstree – to which the Cambridge operation was moved, known as “Lister” and then “Blood Products Laboratory” (“BPL”) – and at Oxford, in that case as a small production facility attached to a research unit and known as the Plasma Fractionation Laboratory (“PFL”) in England, and in Edinburgh, first at the Royal Infirmary in central Edinburgh and then at Liberton in the south of the city, known as the Protein Fractionation Centre (“PFC”).
(451) Minutes of Regional Transfusion Directors meeting 17 November 1954 pp2-3 NHBT0018394
(452) Minutes of Regional Transfusion Directors meeting 14 June 1961 p3 NHBT0018370_001. Of note is the contribution from Dr Wallace, of Scottish National Blood Transfusion Service (“SNBTS”), who described how in Scotland it had been decided that central control of the service was preferable to regional control.
(453) Minutes of Regional Transfusion Directors meeting 14 June 1961 pp3-6 NHBT0018370_001. One of the conclusions in this report – see the chapter on Viral Inactivation – is that research should have occurred in the 1970s, when it could have done so with beneficial results, if it had been adequately resourced. This minute shows that the lack of funding for research had been a long-standing sore. That in turn supports a conclusion that more not only could but should have been done.
(454) Hepatitis C: A review of events leading up to the introduction of routine tests for anti-HCV in the UK p25 NHBT0017232
(455) Minutes of Regional Transfusion Directors Special Meeting 16 April 1970 p3 NHBT0017065
(456) One of four advisory committees dating back to the start of the NHS.
(457) It complained about the reaction their stance had thus far had: “This document presents the unanimous opinion of all the Directors ... submitted to the Chief Medical Officer by the Minister’s Consultant Adviser on Blood Transfusion, in September 1971. Thirteen months later, in October 72, a spokesman for the Department informed the Directors that these comments and proposals were unacceptable. Although it was stated that careful consideration had been given to the future of the N.B.T.S. it was admitted that no expert opinion had been obtained contrary to that of the Regional Transfusion Directors’ and that the intention to allot responsibility for Transfusion Centres to Regional Health Authorities was purely in pursuit of the principle of devolution ... Directors of Regional Transfusion Centres (RTC) have been grappling since 1948 with problems, arising directly from the fragmented structure of the National Blood Transfusion Service (NBTS).” Organisation of the National Blood Transfusion Service January 1973 pp1-3 NHBT0017076_001
(458) Which followed the green paper.
(459) Appendix to Composition and Structure of Committees Report 1973 to 1990 p9 BPLL0004826
(460) Minutes of Central Committee for the National Blood Transfusion Service meeting 19 June 1975 MRCO0000060_023. The history of the Blood Group Reference Laboratory is described in Dr Gunson’s history. Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine Vol 6 1996 pp66-71 NHBT0000028
(461) Minutes of Regional Transfusion Directors meeting 24 April 1974 p5 PRSE0002186, Minutes of Regional Transfusion Directors meeting 9 October 1974 p8 NHBT0016494
(462) Blood Donors and the Transfusion Service British Medical Journal 27 July 1974 DHSC0100024_126
(463) Blood Donors and the Transfusion Service British Medical Journal 27 July 1974 DHSC0100024_126
(464) Blood Donors and the Transfusion Service British Medical Journal 27 July 1974 DHSC0100024_126
(465) Blood Products and Plasma Fractionation Laboratories 8 September 1978 p1 CBLA0000840. This was a report of the Central Committee of the National Blood Transfusion Service to the Advisory Sub-Committee on Blood Products and Blood Group Reference Laboratories for the year ending July 1978. In it he also said: “The writer’s view for many years has been that a separate health authority should be responsible for NBTS; perhaps to begin with the authority could manage the central laboratories and later extend its interest to the regional transfusion centres.” Although this was some four years after the editorial, the wording is clear that Dr Maycock had the “British Medical Journal view” at the time of its publication. This is particularly noteworthy given that it might appear that it was an organisation for which he was responsible that was being criticised, yet he endorsed rather than resisted the criticism.
(466) Hansard Written Answers on Haemophilia 8 July 1974 p2 LDOW0000032
(467) This necessarily involved some expense, and implied a need to ensure that regional transfusion centres were adequately equipped and staffed to provide the increased supply needed.
(468) So far as the Inquiry can determine it, having examined in detail the documents and available individual evidence in respect of each of the regional transfusion centres.
(469) When a need to increase the number of blood donations to ensure there was enough plasma to fractionate for blood products was under discussion in 1976, regional transfusions directors did not think that there would be any problem in achieving an increased rate of donations, given the willingness of people to donate their blood. See for example Minutes of Regional Transfusion Directors meeting 8 December 1976 p5 DHSC0105496_010. Subsequent evidence shows that if a real need were perceived, as during the Gulf War, this proportion would rise markedly. Moore Promoting blood donation: a study of the social profile, attitudes, motivation and experience of donors Transfusion Medicine 30 April 1991 p7 RLIT0000793, Dr Lorna Williamson Transcript 8 December 2021 pp31-32 INQY1000169, Dr Brian McClelland Transcript 27 January 2022 p92 INQY1000177
(470) The director of BPL and his deputy were party to these submissions. Memo from Dr Gunson to the Secretary of the Royal Commission on the National Health Service 20 May 1977 p1 CBLA0000612
(471) Memo from Dr Gunson to the Secretary of the Royal Commission on the National Health Service 20 May 1977 p5 CBLA0000612
(472) Royal Commission on the NHS 21 June 1979 p34 RLIT0001955
(473) In Dr Maycock’s report of September 1978 he complained that NBTS lacked a central research laboratory, and compared unfavourably in that respect with France, Switzerland, the Netherlands and the American Red Cross: “Of two Medical Research Council laboratories concerned with blood transfusion, one has closed and one is likely to close within a year or so.” (He may well have had in mind Lister’s operations since its site at Chelsea had closed and its continuing at Elstree was tenuous, and ended a few months later.) He added “DHSS, in order to be able to carry with confidence its responsibility for providing the transfusion service in England and Wales, should consider fostering the development of a central transfusion research laboratory. Without a basis of research and development, a modern effective transfusion service cannot be maintained … It should be an accepted principle that research and development will not be sacrificed to growing demands for products.” Blood Products and Plasma Fractionation Laboratories 8 September 1978 pp11-12 CBLA0000840
(474) Though without executive control.
(475) Before that, he had been superintendent of the Lister Institute’s laboratory in Elstree.
(476) Obituary of Sir William Maycock British Medical Journal 11 April 1987 RLIT0002212
(477) See Dr Maycock’s valedictory reflections which make this point very clearly. Blood Products and Plasma Fractionation Laboratories 8 September 1978 p11 CBLA0000840
(478) The former was responsible for policy and long-term planning; the latter for staffing and much of the administration.
(479) Though the regions were responsible for the provision of plasma to BPL, and they differed in the quality of their responses to this. See below.
(480) In 1965 a formal agreement between DHSS and Scottish Home and Health Department (“SHHD”) was reached that PFC (to be developed within the first part of the new Royal Infirmary, Edinburgh then being planned) would fractionate plasma from Newcastle, Leeds, Manchester and Liverpool regions, to the extent of 30,000 bottles of plasma protein fraction, plus antihaemophilic globulin produced from 10,000 bottles of blood (in total processing circa 23,000-24,000 litres of plasma). Protein Fractionation Centre Liberton and the arrangements with the NBTS p1 DHSC0003715_171. In the summer of 1966 the location of the blood products unit in Edinburgh was changed to a separate, new site in Liberton (close to but not part of the Royal Infirmary). Letter from John Watt to R N Roberts 22 September 1977 p2 SBTS0000284_041. Between October and November that year planning progressed in the expectation that the new BPU at Liberton (which became known as the PFC) would receive plasma from the five northern regions of England. Letter from John Watt to R N Roberts 22 September 1977 p3 SBTS0000284_041. John Watt was then appointed to head up the new unit: later documents suggest strongly that he did not enjoy the best of relations with Dr Lane.
(481) At a meeting in Edinburgh on 22 August 1977 he is minuted as saying that “it was his intention to concentrate on the production of Factor VIII at the BPL. The latter and the laboratory at Oxford were both funded by DHSS and it would be wrong, in his view, to send plasma from Regional Transfusion Centres in England to the PFC, if this had the effect of leaving spare capacity at Elstree and meant service charges having to be paid. In his view this would have the effect of duplicating costs. He envisaged that only time expired plasma would be sent to the PFC and was unwilling to enter into any long term agreement to have regular quantities of plasma fractionated in Edinburgh.” Note of Joint DHSS/SHHD meeting 22 August 1977 p1 SBTS0000283_006
(482) Proposed Plan for Reorganisation of the NBTS28 February 1980p1 DHSC0002197_089
(483) Proposed Plan for Reorganisation of the NBTS 28 February 1980 p1 DHSC0002197_089
(484) Proposed Plan for Reorganisation of the NBTS28 February 1980p1 DHSC0002197_089. This was diametrically opposite to the view expressed by Dr Lane insofar as blood product production from plasma obtained by NBTS and SNBTS was concerned. He saw no role for PFC in producing coagulation concentrates for England and Wales. It adds force to the observation earlier in the text that, whereas Dr Maycock spoke for both BPL and NBTS, after he retired there were two separate voices. Now, it seems, they advised very different approaches.
(485) ie English and Welsh.
(486) It was proposed that “Officials from the Health Departments, Welsh Office and possibly Northern Ireland would attend as observers.” Minutes of Regional Transfusion Directors meeting 15 October 1980 p4 DHSC0002365_021
(487) Again, in the sense of English and Welsh.
(488) Hepatitis C: A review of events leading up to the introduction of routine tests for anti-HCV in the UKp29 NHBT0017232. It is to be noted that NHS Blood and Transplant (“NHSBT”) in its final submissions to the Inquiry listed expressions of the desire of regional transfusion directors over the years since 1948 for there to be a unitary single service, and their regular rejection until the 1990s. NHSBT said: “Throughout the remainder of these submissions there are various cases where express problems arising from the decentralised structure and funding of the blood service are explored. One example of this is the work of the blood service in trying to achieve self-sufficiency. However, there are also the intangible negatives of delay and confusion which come with a lack of central coordination, executive authority, and funding. These issues, arising at a time before the quick communication of information, are an ever-present factor when one considers the ability and performance of the blood service in responding to issues.” NHSBT Closing Submissions to Infected Blood Inquiry pp49-50 SUBS0000062. These were real problems, and the blood service itself was not the party at fault in failing to put them right.
(489) Central Blood Laboratories Authority (Establishment and Constitution) Order 1982 SI No. 1515.
(490) Professor Cash had been a member: he told the Penrose Inquiry that he was “dismayed, astonished and alarmed” by this – there had been no consultation with the UK blood transfusion services before it happened. Written Statement of Professor John Cash Penrose Inquiry pp2-3 PRSE0002836
(491) These too lacked full coordination, though were more cohesive than their English counterparts.
(492) Memo from Dr Alison Smithies to Dr M A Harris (Deputy Chief Medical Officer), July 1985 DHSC0002323_038
(493) Reorganisation of the Blood Transfusion Service p11 DHSC0003593_052
(494) Reorganisation of the Blood Transfusion Service p3 DHSC0003593_052
(495) Hepatitis C: A review of events leading up to the introduction of routine tests for anti-HCV in the UK p29 NHBT0017232
(496) These services did not include the manufacture of blood products. BPL, PFL and the Blood Group Reference Laboratory remained under separate control. Thus the system remained one in which regional transfusion centres had control over the amount of plasma they could harvest, and once harvested the amount of that plasma they chose to send to BPL, and BPL had control over what was made from that plasma, and how, and the nature and quantities of the blood products supplied to the regions. For BPL to obtain the amounts of plasma it required from England and Wales as a whole depended on the extent to which the National Directorate could coordinate supplies of plasma to it effectively. The chain of supply from regions to the central BPL, and vice versa, thus involved coordination by what was in effect a third party. The merits of this may be thought doubtful, especially in view of the developments reported next in the text, which presumably were in the pipeline when the Directorate was formed. It seems surprising in hindsight that the DHSS preferred this option.
(497) Hepatitis C: A review of events leading up to the introduction of routine tests for anti-HCV in the UK p30 NHBT0017232
(498) Hepatitis C: A review of events leading up to the introduction of routine tests for anti-HCV in the UKp31 NHBT0017232
(499) Letter from Dr Roger Moore to S Edwards 20 March 1991 NHBT0001781
(500) Cash Supply of blood products British Medical Journal 6 April 1991 p1 PRSE0002443
(501) Cash Supply of blood products British Medical Journal 6 April 1991 p2 PRSE0002443
(502) Structural Review of the National Blood Transfusion Service May 1991 NHBT0001799
(503) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine Vol 6 1996 p85 NHBT0000028, Operational Aspects of the National Blood Authority July 1992 p4 SBTS0000466_008
(504) National Blood Authority (Establishment and Constitution) Order 1993 SI no 585. The Order was significantly amended by the National Blood Authority (Establishment and Constitution) Amendment Order 1994 SI no 589.
(505) The Cardiff RTC did not join the NBA, but the Liverpool RTC continued to supply hospitals in North Wales. The History of the Blood Services in the UK 9 November 2021 para 112 INQY0000307
(506) See the statement from the CEO of Bio Products Laboratory Holdings Ltd. He asks that the modern entity be known as BPL Ltd. Written Statement of David Gao paras 4-7 WITN2954001
(507) Fifty Years of an Organized Blood Transfusion Service in Scotland pp1-2 PRSE0003986
(508) Boog Watson The Scottish National Blood Transfusion Association 1940-1965 1965 pp6-8 PRSE0003971
(509) Boog Watson The Scottish National Blood Transfusion Association 1940-1965 1965 p10 PRSE0003971
(510) Boog Watson The Scottish National Blood Transfusion Association 1940-1965 1965 p17 PRSE0003971
(511) Written Statement of Dr Peter Foster pp22-24 WITN6914001
(512) Written Statement of Dr Peter Foster p24 WITN6914001
(513) The “Common Services” comprised a range of disparate services related to health provided across Scotland on a national rather than local basis. Written Statement of Duncan MacNiven para 9.5 WITN7064001
(514) Memo on Common Services Agency from I L Sharp 26 October 1973 LOTH0000249_002
(515) Minutes of Management Committee of the Common Services Agency special meeting 26 April 1978 PRSE0000108
(516) Appendix to Composition and Structure of Committees Report 1973 to 1990 pp35-37 BPLL0004826
(517) Appendix to Composition and Structure of Committees Report 1973 to 1990 p20 BPLL0004826, Minutes of Advisory Committee meeting 1 December 1980 p1 CBLA0001207
(518) Written Statement of Professor Marc Turner para 38 WITN3530007
(519) NHS (Functions of the Common Services Agency) (Scotland) Order 2008.
(520) Now commonly referred to as National Services Scotland.
(521) Written Statement of Professor Marc Turner paras 41-42 WITN3530007
(522) Written Statement of Professor Marc Turner para 42 WITN3530007
(523) Written Statement of Duncan Macniven para 16.1 WITN7064001
(524) It later became the Belfast Regional Transfusion Centre.
(525) Counsel Presentation on History of the Blood Services in the UK 9 November 2021 pp50-53 INQY0000307
(526) Written Statement of Dr Morris McClelland paras 4-6, para 10 WITN0892001
(527) The Health and Personal Social Services (Special Agencies) (Northern Ireland) Order 1990 p1 WITN2681028, Written Statement of Karin Jackson para 12 WITN2681026
(528) The Health and Personal Social Services (Special Agencies) (Northern Ireland) Order 1990 p2 WITN2681028, Written Statement of Karin Jackson para 12 WITN2681026
(529) Written Statement of Dr Morris McClelland para 54, para 166 WITN0892001
(530) He was also the regional transfusion director of the Belfast RTC.
(531) Written Statement of Dr Morris McClelland para 4 WITN0892001
(532) Eastern Health and Social Services Board Northern Ireland Ninth Annual Report 31 December 1982 p34 RHSC0000076, Dr Morris McClelland Transcript 1 February 2022 pp10-20 INQY1000179. See also the chapter on Self-Sufficiency.
(533) A Brief History of the Establishment and Management of the Welsh Blood Service p1 WITN6876002
(534) A Brief History of the Establishment and Management of the Welsh Blood Service p1 WITN6876002
(535) There was one further change during this period. The Secretary of State for Wales set up district health authorities such that the South Glamorgan Health Authority became the South Glamorgan District Health Authority in 1982. In South and Mid Wales, the regional transfusion director of NBTS (Wales) reported to the Welsh Office until 1982, when line management was handed over to the South Glamorgan District Health Authority, this in turn reporting to the Welsh Office.
(536) A Brief History of the Establishment and Management of the Welsh Blood Service p2 WITN6876002
(537) A Brief History of the Establishment and Management of the Welsh Blood Service p2 WITN6876002
(538) A Brief History of the Establishment and Management of the Welsh Blood Service p2 WITN6876002
(539) Dr John (Tony) Napier Transcript 30 November 2021 pp24-25 INQY1000163
(540) Dr John (Tony) Napier Transcript 30 November 2021 pp177-178 INQY1000163
(541) BPL (Elstree), PFL (Oxford) and PFC (Edinburgh).
(542) See the chapter of Self-Sufficiency where it discusses the change in role decided upon for PFC, to the detriment both of PFC in lacking efficiency of production and of the UK in creating a greater shortfall between the domestic production of factor concentrates and total usage of concentrate, leaving a bigger gap to be filled by commercial products. This chapter also has drawn attention to the fact that Professor Cash saw advantages in more effective integration of the services. SHHD tended to follow DHSS on many matters when SNBTS might have moderated decisions if its view had had more than observer status, eg on questions of surrogate screening for HCV, screening for HCV, the drafting of donor leaflets for HIV and the practice of screening donors.
(543) This resonates with Dr Napier’s “Spitfire” observation.
(544) Royal Commission on the NHS 21 June 1979 p34 RLIT0001955
(545) As pointed out elsewhere in this Report, a principle that every part of a blood donation should be used if possible is honoured by separating plasma from red blood cells where both parts are usable.
(546) North East Thames (Brentwood), North West Thames (North London/Edgware), South London (Tooting and Sutton), North Western (Manchester with a sub-centre in Lancaster), Trent (Sheffield), West Midlands (Birmingham), Wessex (Southampton), South Western (Bristol), Mersey (Liverpool), Yorkshire (Leeds), East Anglia (Cambridge), Oxford, Cardiff and Northern (Newcastle). The Mersey RTC also covered North Wales.
(547) For a rather more detailed summary see the 1984 report from Dr Harold Gunson Organisation of the Blood Transfusion Service 3 July 1984 pp5-7 DHSC0001677
(548) As at 1987, that was HIV, Hepatitis B and Syphilis.
(549) Many RTCs offered this as an out of hours service to hospitals. For example Dr Colin Entwistle described how when he was deputy director for the Cambridge RTC between 1968 and 1974 they offered a telephone service so that products could be released from the RTC to hospitals during the night if required. Dr Colin Entwistle Transcript 6 December 2021 p7 INQY1000167
(550) The National Blood Transfusion Service in England and Wales: An Organisational Study October 1987 p14 CBLA0002392
(551) Although some RTCs were based in hospitals, none of the RTCs in England and Wales (unlike in Scotland), acted as a blood bank.
(552) RHAs provided annual funding for the RTCs, as well as capital funding for redevelopment from the regional capital programme. For example £2 million was given to the RTC at Southampton during Dr Frank Boulton’s tenure. Written Statement of Dr Frank Boulton para 266 WITN3456002
(553) North East Thames RTC, for example, did not have a new building until 1987. North East Thames Regional Transfusion Centre: A brief guide July 1987 p5 NHBT0010587. For some RTCs, it was not until the formal inspection regime came into play in the 1980s, that money was found by the RHAs or health boards to upgrade the accommodation. This is because the inspection regime exposed the inadequate buildings and acted as a catalyst for some RTCs to receive the funding they so desperately needed to modernise and expand. By 1990, the National Blood Transfusion Service (“NBTS”) had accepted the case for a medical audit of each RTC. In practice this was carried out by two regional transfusion directors from different centres. For example in 1992 Dr Angela Robinson and Dr Patricia Hewitt audited the Oxford RTC. Medical Audit Visit – Oxford RTC 20 January 1992 NHBT0009748_001
(554) For example the Northern Centre, which, until Dr Huw Lloyd joined in 1987, had only one full-time consultant. Dr Huw Lloyd Transcript 8 February 2022 p89 INQY1000182. Dr John Jenkins described resources at Brentwood in September 1973 as being so stretched “that we have no margin for holidays, sickness, failure of apparatus”. Letter from Dr Jenkins to Dr William d’A Maycock 24 September 1973 DHSC0002175_043. Dr Jean Harrison in her statement makes it clear that when she joined Brentwood in 1981 there was no other consultant and so she had to get cover from other centres when she went on holiday. Written Statement of Dr Jean Harrison para 17 WITN7046001. In August 1984, Dr Ian Fraser at South West RTC said: “there is no way that we can expand our plasma output with a diminishing establishment and a reduced budget” and that they did not have the staff to carry out the work that the introduction of SAG-M (a mixture of saline, adenine, glucose and mannitol) would incur. Letter from Dr Fraser to Winston Tayler 22 August 1984 NHBT0098683_001
(555) For example the Trent RTC based in Sheffield also acted as a reference laboratory for hospital blood banks in the area and provided regional services for antenatal blood groups, serology and for histocompatibility. Dr William Wagstaff Transcript 25 January 2022 p23 INQY1000175
(556) An example is the Cardiff RTC, though the service did not continue for long, which Dr Napier thought was because interest in it waned. Dr John (Tony) Napier Transcript 1 December 2021 pp109-111 INQY1000164
(557) The South Thames RTC was funded by two RHAs, the South West Thames RHA and the South East Thames RHA. In the case of Cardiff RTC, accountability was to the South Glamorgan Health Authority. Dr John (Tony) Napier Transcript 30 November 2021 pp12-13 INQY1000163
(558) See the oral evidence to this effect. Dr William Wagstaff Transcript 25 January 2022 pp24-25, p30 INQY1000175 and Written Statement of Professor Brian Edwards para 15 WITN7641001. See also Written Statement of Robert Nicholls paras 4.3, 5.1 WITN7522001
(559) Minutes of Regional Transfusion Directors meeting 5 October 1977 p6 NHBT0016470, Letter from Dr Walford to Dr Wagstaff 18 May 1981 CBLA0001354
(560) Dr John (Tony) Napier Transcript 30 November 2021 pp23-24 INQY1000163
(561) Dr John (Tony) Napier Transcript 30 November 2021 p12 INQY1000163, A Brief History of the Establishment and Management of the Welsh Blood Service p1 WITN6876002
(562) The South East Scotland Transfusion Centre in Edinburgh, the North East Transfusion Centre in Aberdeen, the West of Scotland Transfusion Centre in Glasgow, the North of Scotland Transfusion Centre in Inverness and the East of Scotland Transfusion Centre in Dundee.
(563) His role changed after 1988 when he became the medical and scientific director. Curriculum Vitae of Professor Cash p1 PRSE0003376
(564) Dr Brian McClelland Transcript 27 January 2022 p13 INQY1000177
(565) Dr Brian McClelland Transcript 27 January 2022 pp53-54 INQY1000177
(566) The RTC in Glasgow (in the grounds of the Law Hospital) was unusual in having a freeze-drying plant (which had originally been commissioned shortly after the Second World War) that produced small amounts of freeze-dried plasma. This eventually had to be decommissioned as it did not meet Good Manufacturing Practice requirements. Dr Brian McClelland Transcript 27 January 2022 pp152-153 INQY1000177
(567) For example in 1970 a new donor centre was commissioned for the RTC in Inverness, which was thought even before it was built to be inadequate in terms of the size of the office and donor accommodation, and to have inadequate plasmapheresis and storage facilities. Stated case for extension to Inverness Regional Transfusion Centre February 1982 p2 SBTS0000136_047. The RTC needed extending again in 1982 as it could only cope with a maximum of seven donors at a time. Stated case for extension to Inverness Regional Transfusion Centre February 1982 p5 SBTS0000136_047. Dr Gamal Gabra gave oral evidence about the inadequate facilities in Glasgow during his time there. Dr Gamal Gabra Transcript 3 February 2022 pp15-20 INQY1000180. Aberdeen’s facilities were also inadequate. Report, Statistical Summary and Accounts for Year ended 31 March 1968 p5 SBTS0000554, Memo from Dr Alexander Moir to Dr Geoffrey Scott 14 June 1977 SCGV0000125_071, Report on informal visit to blood transfusion service facilities at Aberdeen and Edinburgh 9 May 1977 p1 SCGV0000125_072. In 1982 the Medicines Inspectorate stated that serious consideration must be given to having a new centre by June 1987. Visit to Aberdeen and North East Scotland Blood Transfusion Service 24 March 1982 p7 PRSE0003178. However a new centre was not built until 1993. SNBTS Annual Report 1992/93p12 NHBT0002938. In March 1982 the Medicines Inspectorate report on the RTC in Edinburgh described the existing facilities for the processing and handling of blood as “grossly deficient”. Visit to Edinburgh and SE Scotland Blood Transfusion Service 10-11 March and 10-12 May 1982 p1SBTS0000407_007. In Edinburgh and South East Scotland, Dr McClelland would have wished to use a comprehensive donor questionnaire to help avoid the risk of transmitting AIDS through blood, and (if it could be done) to introduce direct donor interviews, but the staffing and resources for this proved lacking. Dr Brian McClelland Transcript 27 January 2022 pp34-38 INQY1000177
(568) A general response by the Common Services Agency of the Scottish Health Service to the inspection of SNBTS RTCs by Officers of the Medicines Division (DHSS) March 1982 pp2-3 SCGV0000270_032, The regulation of the manufacture of medicinal products derived from blood plasma and the preparation of blood and blood components by the Scottish Blood Transfusion Service October 2011 p8 PRSE0002556
(569) A general response by the Common Services Agency of the Scottish Health Service to the inspection of SNBTS RTCs by Officers of the Medicines Division (DHSS) March 1982 p2 SCGV0000270_032
(570) Written Statement of Dr Morris McClelland p10 WITN0892001 and Fractionation for the Northern Ireland Blood Transfusion Service September 1981 SCGV0000104_117
(571) Written Statement of Dr Morris McClelland p10 WITN0892001
(572) Written Statement of Dr Morris McClelland pp10-11 WITN0892001
(573) See below.
(574) Oxford RTC was the exception to this. This was because all their plasma for fractionation was sent to the Plasma Fractionation Laboratory (“PFL”) in Oxford, which sent the fractionated products directly to the Oxford Haemophilia Centre. Dr Colin Entwistle Transcript 6 December 2021 p39 INQY1000167
(575) For example: South East Thames RTC kept a quarter of the product received from BPL for emergencies, distributing the remaining three quarters to the haemophilia centres in the areas in proportion to the number of people with bleeding disorders treated at those centres. Letter from Professor Ilsley Ingram to Dr Maycock 24 November 1976 p1 CBLA0000503. The North London RTC used Dr Simon Ardeman, a consultant haematologist at Edgware General Hospital, who did not receive any Factor 8 himself, to act as the “arbitrator” between the various hospitals who received their Factor 8 from the North London RTC, to determine their allocation of Factor 8. Dr Patricia Hewitt Transcript 9 December 2021 pp52-53 INQY1000170, Note of meeting with Dr Hewitt p20 NHBT0019621. In the 1970s North East Thames RTC received BPL products for onward transmission to haemophilia centres. Each haemophilia centre was provided with a “free allocation” of BPL products. Anything they wanted over and above that they would have to purchase from the North East Thames RTC if it was available. Letter from Jean Harrison to Lorne Williamson 28 November 1990 p1 RLHO0000001_017. By 1990, BPL was providing its products directly to the hospitals. Memo from Dr Ernie Gascoigne to H Evans and others 19 January 1999 BPLL0016082_024. The Northern RTC had no role in the allocation of the product, they simply acted as an intermediary between BPL and the end user. Dr Huw Lloyd Transcript 8 February 2022 paras 129-131 INQY1000182, Letter from Dr Lloyd to Richard Slack 1 September 1989 p7 TYWE0000064
(576) For example the Oxford, Liverpool and North Wales, Trent and North London RTCs.
(577) Dr John (Tony) Napier Transcript 30 November 2021 pp68-69 INQY1000163. In East Anglia, Dr Jack Darnborough did not at first consider it appropriate for the RTC to be distributing BPL material but having discovered that a haematologist in his area was purchasing a large amount of commercial Factor 8, he agreed to do so. Letter from Dr Darnborough to Dr Maycock 3 August 1976 CBLA0000410, Letter from Dr Darnborough to Dr Maycock 26 August 1976 CBLA0000431, Letter from Dr Maycock to Dr Darnborough 6 September 1976 CBLA0000435. It seems that by 1 April 1977 the RTC held all the supplies of Factor 8 for the area. Letter from Stanley Godfrey to All Regional Transfusion Directors in England and Wales 10 July 1981 DHSC0002209_037, Letter from Dr Darnborough to Stan Godfrey 3 August 1981 DHSC0002211_012
(578) For example in East Anglia by 1982/83 there was a regional contract for the supply of Factor 8. Letter from Barry Barber to Dr Darnborough 15 February 1983 BAYP0000028_034. Dr Darnborough appears to have been involved in meeting commercial suppliers. Letter from Linda Frith to Dr Darnborough 6 November 1984 BAYP0000025_071. In Yorkshire prior to 1981, the RTC had no role in the purchase, storing or distribution of commercial Factor 8. Letter from Dr Derrick Tovey to Stan Godfrey 21 July 1981 DHSC0002209_076. This changed in 1981, and Yorkshire began to purchase all blood products for the region including the Yorkshire Haemophilia Units. Regional Purchase of Commercial Blood Products October 1983 p2 CBLA0001761 and Letter from Dr Angela Robinson to Dr Gunson 4 December 1989 p1 NHBT0019148. In the West Midlands by January 1981, the RTC held all the region’s commercial and BPL Factor 8. The purchase of commercial products was arranged by the RTC in consultation with the RHA and Treasurer. Letter from Stan Godfrey to Dr George Bird 30 January 1981 DHSC0002203_017 and Letter from Dr Bird to Stan Godfrey 5 February 1981 NHBT0010095. Dr Fereydoun Ala (the regional transfusion director) met with representatives from the pharmaceutical companies. Letter from Linda Frith to Dr Ala 24 August 1987 BAYP0000010_151. In the North West, decisions appeared to be made on a regional basis. On 18 January 1985 Dr Gunson (in his regional transfusion director role) wrote to BPL to say that regionally they had decided to use only heat-treated commercial Factor 8. He therefore cancelled all orders for non-heat-treated products for January to March 1985. Letter from Dr Gunson to Norman Pettet 18 January 1985 CBLA0001989
(579) For example Manchester. Proposal from Dr Gunson for the Chairman to Consider 23 October 1987 NHBT0096598_012
(580) For example East Anglia. Letter from Stan Godfrey to All Regional Directors in England & Wales 10 July 1981 DHSC0002209_037 and Letter from Dr Darnborough to Stan Godfrey 3 August 1981 DHSC0002211_012
(581) 8Y was an NHS Factor 8 concentrate produced at BPL, which did not transmit either hepatitis or HIV viruses.
(582) Dr Kernoff at a meeting of regional haemophilia centre directors, in which there appears to have been general concern about the system from other haemophilia centre directors. Minutes of UK Regional Haemophilia Centre Directors Committee meeting 11 September 1989 p3 HCDO0000436
(583) For example the RTC in Aberdeen had an arrangement with the Chief Administrative Medical Officer (“CAMO”) of the Grampian Health Board that the haemophilia director at the Aberdeen Haemophilia Centre would order the commercial products required, the Health Board would pay for them, and the North East Scotland Blood Transfusion Centre would store and issue them as required. Written Statement of Professor Stanislaw Urbaniak para 86 WITN6960001. Accordingly, the North East Scotland Blood Transfusion Centre held all stocks for the region. However, it did not get involved in decisions about allocation of product: this was decided between the PFC and the haemophilia centre directors. Written Statement of Professor Stanislaw Urbaniak para 92 WITN6960001. The RTC for Edinburgh and the South East of Scotland lost its role in the purchase or storing of commercial products after 1980. This was then done by Professor Ludlam. Dr Brian McClelland Transcript 27 January 2022 pp74-75 INQY1000177
(584) Dr Morris McClelland Transcript 1 February 2022 pp35-36 INQY1000179
(585) Blood Transfusion Service Financial Position on Baseline Funding February 1989 RHSC0000066_024
(586) See the chapter on Self-Sufficiency.
(587) For example red cell concentrates and cryoprecipitate.
(588) Minutes of Regional Transfusion Directors meeting (incomplete) 28 October 1964 p2 NHBT0018361. The issue was raised at the regional transfusion directors’ meeting on 28 October 1964, although the minutes for that meeting are incomplete. An account of what was discussed regarding recruitment can be found in the minutes of the next meeting on 9 December 1964. Minutes of Regional Transfusion Directors meeting 9 December 1964 pp2-3 NHBT0018360
(589) Minutes of Regional Transfusion Directors meeting 9 December 1964 p2 NHBT0018360
(590) Minutes of Regional Transfusion Directors meeting 9 December 1964 p2 NHBT0018360
(591) Minutes of Regional Transfusion Directors meeting 30 June 1965 pp6-7 NHBT0018356
(592) Written Statement of Dr William Wagstaff para 64 WITN6988001
(593) The only support that was provided centrally was the preparation of leaflets and posters for the regions to use. Dr Vanessa Martlew, describing donor recruitment at the Manchester RTC, recalled that posters with babies on them seemed to be the most successful in recruiting new donors. Written Statement of Dr Vanessa Martlew para 87 WITN4034001
(594) For example in Cardiff they made radio and press appeals. Dr John (Tony) Napier Transcript 30 November 2021 p93 INQY1000163
(595) For example on 25 May 1988, Dr Contreras wrote to Dr Wagstaff to say that “In light of the need to provide more and more plasma for BPL, as well as increasing demands for platelets and other fresh products by hospitals, the cut in the Publicity Budget is particularly serious and could not be worse timed.” Letter from Dr Contreras to Dr Wagstaff 25 May 1988 p1 NHBT0118872_004. By June 1988 the publicity budget had been increased by £150,000 to £400,000. Minutes of Regional Transfusion Directors meeting 29 June 1988 p5 NHBT0018190. Dr Contreras still considered that an “insufficient publicity budget in the current climate, eg the cost of television advertising”. Minutes of Regional Transfusion Directors meeting 4 October 1988 p3 NHBT0018189. See also Written Statement of Dr Roger Moore para 9 WITN6919001
(596) Minutes of Central Blood Laboratories Authority meeting 20 November 1985 p3 BPLL0011017. This was not universally so, with a continuing fall in donors recorded in Brentwood in 1986: “The blood collection programme at Brentwood has steadily and consistently declined since 1981. Figures were not available for 1985 but it can be assumed that the impact of AIDS will cause a further fall (estimated to be as high as 20% in the London area by colleagues in Tooting).”NETHRA Blood Transfusion Services with Special Reference to Hampstead, Bloomsbury and Islington 19 March 1986 p6 SBTS0000618_160
(597) Yorkshire Regional Blood Transfusion Service Press Release It is safe and we are asking you 24 January 1990 NHBT0000077_104
(598) Dr Entwistle recalled problems with collection from some ethnic groups and even sought assistance from the local MP in Leicester. He said that this made little difference and that it remains a problem to this day. Written Statement of Dr William Wagstaff para 50 WITN6988001. Dr Harrison recalled issues at the North East Thames RTC. Written Statement of Dr Jean Harrison paras 78-79 WITN7046001
(599) Its remit was “To consider and advise the National Director on measures to ensure that sufficient donors are recruited and retained to reach and maintain the targets for blood and plasma collection in the most economical manner”and to “advise on the effective disposition of the central publicity budget.”Minutes of National Provision of Donors Committee meeting 1 February 1989 p1 NHBT0004016_006
(600) Minutes of National Provision of Donors Committee meeting 10 October 1990 p2 NHBT0097472_052
(601) Written Statement of Dr Colin Entwistle para 15 WITN6917001. Thus donors were handed leaflets and pamphlets at the sessions to encourage others to give blood. Minutes of Regional Transfusion Directors meeting 6 July 1977 p2 DHSC0200019_002
(602) For example in the Edgware North London Centre, they had a donor association which organised awards ceremonies every month to celebrate donors who had reached milestone numbers of donations. Professor Dame Marcela Contreras Transcript 2 December 2021 pp41-42 INQY1000165
(603) See, for example, the evidence of Professor Dame Marcela Contreras Transcript 2 December 2021 pp42-43 INQY1000165
(604) Professor Dame Marcela Contreras Transcript 2 December 2021 pp71-72 INQY1000165. The South Thames RTC was another centre which often experienced shortages. For example in December 1985, October 1987 and June 1990 surgical lists had to be cancelled. Memo from Alun Williams to Mr Langsdon 20 December 1985 DHSC0002163, Memo from Dr Edmund Harris to Graham Hart 2 October 1987 DHSC0002382_106, Letter from Dr Keith Rogers to Dr Gunson 18 June 1990 NHBT0008837 and Letter from Dr Gunson to Dr Rogers 19 June 1990 NHBT0008836. The London RTCs were not, however, alone. For example the South West RTC also had a shortage in 1990 causing operations to be cancelled. Letter from Dr Fraser to Dr Gunson 9 May 1990 NHBT0097017_003
(605) Oxford had a similar agreement with North East Thames RTC. Written Statement of Dr Jean Harrison para 21 WITN7046001, The Independent Transfusion centre to pay £150,000 for blood 10 May 1988 DHSC0003993_022. North East Thames RTC also entered into discussions with the East Anglian RTC to explore whether they could collaborate to ensure sufficient blood was collected to supply hospitals in both regions. Minutes of Medical Consultants and Business Managers from North East Thames BTS meeting 3 November 1992 p2 NHBT0002534
(606) Dr Rogers of South London discussed his concerns in January 1986. Note of discussions with Dr Rogers (Tooting) January 1986 SBTS0000673_141
(607) See for example Dr Fraser of South West RTC in August 1984. Letter from Dr Fraser to Winston Tayler 22 August 1984 NHBT0098683_001
(608) Professor Dame Marcela Contreras Transcript 2 December 2021 pp37-38 INQY1000165
(609) NETRHA Blood Transfusion Services with Special Reference to Hampstead, Bloomsbury and Islington 19 March 1986 p3 SBTS0000618_160
(610) NETRHA Blood Transfusion Services with Special Reference to Hampstead, Bloomsbury and Islington 19 March 1986 p19 SBTS0000618_160
(611) Oxford RTC for example could have collected more donations than they did, despite being able to meet the needs of their own population, as well as supply blood to the North East Thames RTC and the North West Thames RTC. Dr Colin Entwistle Transcript 6 December 2021 pp31-32 INQY1000167
(612) The Northern RTC for example had some periods which were particularly difficult in terms of donor numbers around 1987-88 as a result of shipyards and steelworks closing down in the North East and the loss of those donors who had donated at workplace sessions there. Dr Huw Lloyd Transcript 8 February 2022 p176 INQY1000182. See also Graph showing Northern Region Blood Transfusion Service Donors Bled 1947 to 1994 WITN6935006, Chart showing number of registered donors WITN6935008, Graph showing Northern Region Blood Transfusion Service industrial donations as percentage of all donors bled and unemployment rate WITN6935009
(613) He was referring here in part to the Oxford RTC in an article he wrote for the British Medical Journal in September 1987. Cash The blood transfusion service and the National Health Service British Medical Journal 12 September 1987 p1 PRSE0000598, The Daily Telegraph Blood service shambles denied by Minister and The Guardian Minister denies blood ‘shambles’ 12 September 1987 DHSC0038579_016. Dr Entwistle said he was not aware of the shortage and said this underlined the need for a rationalisation of the service. Dr Colin Entwistle Transcript 6 December 2021 p38 INQY1000167
(614) Her experience was that when she had “appealed to my colleagues in neighbouring areas for help with supplies they have always responded promptly and we have had blood here in no time at all” and that “no patient has ever been put at risk because of a lack of blood supplies.” The Daily Telegraph Blood service shambles denied by Minister 12 September 1987 DHSC0038579_016
(615) Dr Colin Entwistle Transcript 6 December 2021 p38 INQY1000167. At the East Anglia RTC management meeting on 8 April 1991, Dr Williamson reported concern that the stock holding of blood continued to be at a very high level and felt that steps could be taken to reduce the intake. Providing assistance overseas had been considered but was not possible and so the meeting focused on cancelling donor sessions, in particular some of the industrial or service sessions. Notes of Management Group Meeting 8 April 1991 p2 NHBT0041282_003
(616) NETHRA Blood Transfusion Services with Special Reference to Hampstead, Bloomsbury and Islington 19 March 1986 p5 SBTS0000618_160. Apart from some plasma being imported after the Second World War from Canada, for an unknown but short period following the cessation of hostilities, this is the only evidence the Inquiry has found which reliably records that the UK received blood to use in the NHS which did not come from voluntary non-remunerated donors living within the UK.
(617) Dr Vanessa Martlew Transcript 20 January 2022 p51 INQY1000174
(618) With supplies of red blood cells being sourced from as far away as Manchester and Scotland for the South Thames RTCs in January 1992 and Glasgow for the South West RTC in October 1992. Letter from David McIntosh to Belinda Phipps 23 January 1992 SBTS0000467_018 and Letter from Nick Tandy to Professor Cash 16 October 1992 SBTS0000027_046
(619) Dr Colin Entwistle Transcript 6 December 2021 p32 INQY1000167
(620) See the chapter on Self-Sufficiency.
(621) Dr William Wagstaff Transcript 25 January 2022 pp36-46 INQY1000175. The evidence of Dr Harrison is that initially the targets were based on the capacity of each RTC, only later being based on its population. Written Statement of Dr Jean Harrison 23 March 2022 para 97 WITN7046001. See also the evidence of Dr Roger Moore: Written Statement of Dr Roger Moore 5 December 2021 para 38.2 WITN6919001. There is evidence that in 1976-77 BPL allocated product based on the number of people with bleeding disorders based on a haemophilia centre’s figures. This led to correspondence between Dr Geoffrey Tovey (director, South West RTC) and Dr Rosemary Biggs at Oxford Haemophilia Centre, who was asking for a larger allocation of product, since the Exeter and Bristol centres were allocated a supply in proportion to the number of patients treated there, but half the patients in the region were treated at associate centres. Letter from Dr Biggs to Dr Tovey 14 October 1976 OXUH0000686_004, Letter from Dr Tovey to Dr Biggs 8 October 1976 CBLA0000467, Letter from Dr Biggs to Dr Tovey 25 October 1976 OXUH0000686_002, Letter from Dr Tovey to Dr Biggs 9 February 1977 HCDO0000023_005, Letter from Dr Maycock to Dr Biggs 21 September 1976 DHSC0100006_179
(622) This is what happened to the NETRHA in 1978. Letter from Dr Jenkins to Dr Hill 11 July 1978 DHSC0002187_117. See also Unconfirmed Minutes of Haemophilia/Associate Haemophilia Centres and Blood Transfusion Centres, RHAs 15 December 1976 CBLA0000533
(623) See for example the minutes of the meeting of the regional transfusion directors on 26 September 1979. Note of an Ad Hoc Group of Regional Transfusion Directors meeting 26 September 1979 DHSC0002195_044. A further example is when Dr Wagstaff wrote to Dr Maycock in September 1977 explaining that he was keen to harvest more plasma from donations in Trent than was then being achieved, but in order to do so he needed to persuade the RHA to invest in more double packs. Dr Wagstaff thought he would be able to persuade the RHA to make this investment if BPL were able to guarantee that they would receive more than their current allocation of BPL product, so as to reduce the area spend on commercial products. Letter from Dr Wagstaff to Dr Maycock 27 September 1977 CBLA0000660
(624) Initially the Oxford RTC was excluded from this system as all its plasma was fractionated at PFL, but from the second half of 1981 the system was applied to Oxford as well. Dr Colin Entwistle Transcript 6 December 2021 pp147-150 INQY1000167. See also the correspondence between Dr Richard Lane (BPL) and Dr Entwistle: Letter from Dr Lane to Dr Entwistle 12 June 1981 CBLA0001380 and Letter from Dr Entwistle to Dr Lane 23 June 1981 CBLA0001389. Equally, the Wessex RTC was also initially excluded from it because it supplied the Lord Mayor Treloar School and so special provisions applied.
(625) Report to CBLA: Plasma Supply for Self-Sufficiency January 1984 p2 CBLA0001800. This was the regional health authority’s position in 1990 as well. Letter from Dr Wagstaff to Dr Moore 2 March 1990 NHBT0097035_070
(626) Dr Huw Lloyd Transcript 8 February 2022 pp146-147 INQY1000182
(627) For example in 1981 the South Western RHA refused to fund South West RTC to provide 30,000 kg to BPL stating that the plasma target for the region was “inflated to an unreasonable degree by the expectations of the directors of the haemophilia centres” and that a more appropriate target was 20,000 kg. In fact the South Western RHA did agree to fund 30,000 kgs of plasma, but by 1987/1988. Counsel Presentation on Six English Regional Transfusion Centres 9 December 2022 p27 INQY0000414. See also Written Statement of Robert Nicholls para 6.12 WITN7522001 and Letter from Winston Tayler to John Parker 27 September 1984 WITN7522004
(628) See for example the attempts made by Dr Gunson in 1984/85 to get the RHAs to fund the RTCs’ plasma targets. Report to CBLA: Plasma Supply for Self-Sufficiency January 1984 CBLA0001800, Supplement to Report: Plasma Supply for Self-Sufficiency in Blood Products 13 February 1984 DHSC0001967
(629) Minutes of Central Blood Laboratories Authority meeting 28 November 1984 DHSC0001101. By September of 1984 Dr Gunson was of the view that only the Trent and NE Thames regions’ plasma supply were progressing at a satisfactory rate. Minutes of Central Blood Laboratories Authority meeting 26 September 1984 p4 CBLA0001896. By 18 February 1985 only six RHAs had agreed to a plan to meet the self-sufficiency timescales, three agreed but without timescale, two actively opposed it, and one had not responded. This was insufficient to achieve the aim of self-sufficiency. Minutes of Regional Transfusion Directors meeting 23 January 1985 p8 CBLA0001995. However, while the pro rata system was in place, the region served by the Yorkshire RTC was self-sufficient in Factor 8. It had made use of plasmapheresis to produce sufficient plasma to justify this. Written Statement of Dr Angela Robinson paras 33, 776 WITN6926001
(630) In the first months, different RHAs/RTCs adopted different approaches to charging. In some areas charges were passed on to the district health authorities and in some they were not. Minutes of NBTS/CBLA Liaison Committee meeting 17 May 1989 NHBT0007355
(631) Letter from Peter Ward to Roger Schofield 31 March 1992 NHBT0003299
(632) In Trent, it was said by Dr Richard Alderslade to Dr Jeremy Metters in March 1992 that this subsidy was to the tune of £1.2m in 1991/92. Letter from Dr Alderslade to Dr Metters 9 March 1992 DHSC0002411_023. This was also the case in North East Thames RTC. Letter from Mansel Chamberlain to Dr Bernard Crowley 4 May 1990 NHBT0097035_023. Yorkshire estimated that in 1991 it cost them £15 more per kg to supply plasma to BPL than they received. Minutes of NBTS/CBLA Liaison Committee meeting 10 April 1991 NHBT0000077_056. In 1992-93 this was £18.50 per litre. Letter from Peter Ward to Roger Schofield 31 March 1992 NHBT0003299. Dr Robinson noted that the “price for a unit of apheresis plasma proved to be insufficient to cover the cost of producing it at the YRTC.” Written Statement of Dr Angela Robinson para 33 WITN6926001
(633) Gunson Trends in blood transfusion practice in England and Wales Health Trends November 1986 p2 NHBT0017097
(634) See the chapter on Response to Risk by the Blood Services.
(635) Dr Huw Lloyd Transcript 8 February 2022 pp90-94 INQY1000182. This was not helped by the fact that the Northern area could not get funding for SAG-M. Report to CBLA: Plasma Supply for Self-Sufficiency January 1984 p2 CBLA0001800
(636) Ouwehand The East Anglian BTS: Towards the Year 2000 25 January 1990 p8 NHBT0010585_002
(637) A mixture of saline, adenine, glucose and mannitol.
(638) For example the Welsh RTC target had been 11,800 kg but it reported that it was unlikely to receive finance to cover SAG-M, so would probably only reach 9,000 kg. Report to CBLA: Plasma Supply for Self-Sufficiency January 1984 p5 CBLA0001800. In March 1985, a letter from Oxford RTC stated that its proposal to use 45,000 SAG-M packs had been severely cut by their RHA and as a result there were no realistic proposals as to when Oxford RTC could ever achieve its plasma supply targets. Letter from Dr Entwistle to Alun Williams 29 March 1985 DHSC0002265_018
(639) Report to CBLA: Plasma Supply for Self-Sufficiency January 1984 p1 CBLA0001800
(640) North London RTC was a pioneer in plasmapheresis, beginning with manual in 1967, later moving to automatic. North London RTC had three plasmapheresis clinics. By October 1987 the number of regular attenders exceeded 2,500, and over 80% of these donors attended for donation once a fortnight. Professor Dame Marcela Contreras Transcript 2 December 2021 pp142-146 INQY1000165, Letter from Dr Contreras, Dr Hewitt and Dr Mahes de Silva to the Editor of the Economist Newspaper 12 October 1987 NHBT0086659. Yorkshire was also an early adopter of automated plasmapheresis, opening a centre in Bradford in 1982, by August 1983 there were 22 automated machines operating in Yorkshire RTC spread across three sites. Dr Gunson Notes on Visit to Yorkshire RTC 24 August 1989 p1 NHBT0003366. Dr Harrison (Director, North East Thames RTC) did not consider plasmapheresis an efficient way to collect plasma. Dr Moore Visit Note: North East Thames RTC 14 August 1989 NHBT0003370. Dr Harrison preferred to use recovered plasma because this was in her view a much cheaper way to reach her targets. Written Statement of Dr Jean Harrison paras 142-163, 221 WITN7046001. At Newcastle, Dr Lloyd explained that initially he thought “the only way to get a major change in plasma production was to go full force into plasmapheresis … But once I got into the job … I realised that we had a terrific opportunity to separate a lot more blood.” His RTC had a small plasmapheresis unit but mostly plasma was recovered from whole blood donations and by 1992/3 the Northern Centre was producing the third highest amount of plasma in England and Wales, behind North London and Yorkshire. Dr Huw Lloyd Transcript 8 February 2022 pp147-154 INQY1000182, Written Statement of Dr Huw Lloyd p34 WITN6935001
(641) Letter from Dr Scott to Dr Maycock 2 July 1975 CBLA0005695, Letter from Dr Maycock to Dr Tovey 14 July 1975 CBLA0009058, Letter from Dr Tovey to Dr Maycock 18 July 1975 CBLA0009063, Letter from Dr Maycock to Dr Tovey 22 July 1975 BPLL0003754. Since part of the purpose of supplying BPL was to enable the UK to avoid having to rely on imported concentrates this approach seems counter-productive. Cryoprecipitate generally provided a higher yield of Factor 8 activity than concentrate, for some activity was lost in the process of fractionation.
(642) Letter from Dr Angela Robinson to Dr Gunson 22 March 1989 NHBT0027512
(643) Dr Gunson Notes on Visit to Yorkshire RTC 24 August 1989 p1 NHBT0003366
(644) Written Statement of Dr Huw Lloyd para 29 WITN6935001, Dr Huw Lloyd Transcript 8 February 2022 pp145-154 INQY1000182
(645) Compare with the section on Newcastle in the chapter on Haemophilia Centres: Policies and Practice. Dr Jones maintained that the reason the Centre he directed used as much commercial concentrate as it did was because he could not get sufficient supplies of NHS product. The view of the RTC and regional transfusion director was that that was what he preferred to use.
(646) Letter from Dr Lloyd to Richard Slack 1 September 1989 p9 TYWE0000064
(647) Written Statement of Dr Morris McClelland p14 WITN0892001
(648) Dr Morris McClelland Transcript 1 February 2022 pp9-11 INQY1000179. See also for 1980:
“This was a difficult year for the Northern Ireland Blood Transfusion Service and for the first time in recent years the number of units of blood collected was actually less than in the previous year. This was the case in spite of the fact that the total number of donation sessions was increased. The reduction was undoubtedly due to the effects of the recession with resulting factory closures and pay-offs. In spite of this the needs of all hospitals in Northern Ireland for blood and blood products were met.” Eastern Health and Social Services Board Northern Ireland: Seventh Annual Report 31 December 1980 p41 RHSC0000078
(649) Written Statement of Dr Morris McClelland para 14 WITN0892001
(650) Written Statement of Dr Morris McClelland para 28(d) WITN0892001
(651) Dr Morris McClelland Transcript 1 February 2022 p82 INQY1000179
(652) It remained suitable for producing plasma protein fraction.
(653) Dr Morris McClelland Transcript 1 February 2022 p39 INQY1000179
(654) Eastern Health and Social Services Board Northern Ireland: Ninth Annual Report 31 December 1982 p34 RHSC0000076
(655) Written Statement of Dr Morris McClelland para 32 WITN0892001, Dr Morris McClelland Transcript 1 February 2022 p82 INQY1000179
(656) Professor Urbaniak was the director for Aberdeen and North East Scotland. Written Statement of Professor Stanislaw Urbaniak para 32 WITN6960001
(657) Dr McClelland was the director for Edinburgh and South East Scotland. Written Statement of Dr Brian McClelland paras 57-58 WITN6666001
(658) Dr Gillon was the consultant in charge of the donor programme for Edinburgh and South East Scotland. Written Statement of Dr Jack Gillon paras 35-57 WITN6987001
(659) Edinburgh and South East Scotland Blood Transfusion Service: Forty-Ninth Annual Report 31 March 1985 p26 LOTH0000181
(660) Dr Brian McClelland Transcript 27 January 2022 p94 INQY1000177, Dr Gillon Transcript 19 January 2022 pp23-24 INQY1000173. See also Dr Gillon’s evidence to Penrose that (a) donor attendances dropped from nearly 340,000 in 1984/85 to 315,000 in 1987/1988 (a drop of about 8%), which he ascribed to donors first being asked to sign a declaration that they had not engaged in risky behaviours and (b) a drop in new donor numbers from 47,269 in 1983/84 to 34,073 in 1987/88 (a drop of about 20%). Written Statement of Dr John Gillon pp9-10 PRSE0002853. See also a graph of SNBTS national donor attendances. Letter from Professor Cash to James Donald 29 October 1987 p4 SCGV0000269_156
(661) Letter from Professor Cash to James Donald 29 October 1987 p1 SCGV0000269_156
(662) Note of Scottish Home and Health Department and Common Services Agency/SNBTS meeting 18 April 1988 p1 SBTS0000687_089
(663) Scottish National Blood Transfusion Service Annual Report 1988-1989 p4 NHBT0002934
(664) Informal notes of the Northern Division of the SNBTS meeting 14 December 1989 p1 NHBT0203704_007
(665) Dr Brian McClelland Transcript 27 January 2022 p59 INQY1000177
(666) Written Statement of Professor Stanislaw Urbaniak para 113 WITN6960001
(667) Dr A E Bell reminded participants in a meeting he was chairing in February 1984 of SNBTS and haemophilia directors that “the aim of the SNBTS and of national policy was for Scotland to be self sufficient”. Minutes of Directors of the Scottish National Blood Transfusion Service and Haemophilia Directors meeting 2 February 1984 p3 PRSE0001556. Dr Brian McClelland said that he understood self-sufficiency to be a national objective when he became a director in 1979. Dr Brian McClelland Transcript 27 January 2022 p64 INQY1000177
(668) Dr Brian McClelland Transcript 27 January 2022 pp65-66 INQY1000177
(669) Dr Brian McClelland Transcript 27 January 2022 pp66-67 INQY1000177
(670) Letter from B O B Gidden to Regional Administrators 24 December 1974 p1 CBLA0000239, Scottish National Blood Transfusion Service Annual Report 31 March 1976 p29 PRSE0002133, Clinical Trials of Crystalloid Suspended Human Red Cells for Transfusion June 1982 p2 SBTS0000231_024
(671) Cash Principles of Effective and Safe Transfusion PROC Royal Society of Edinburgh 1971 PRSE0002637
(672) Cash Factor VIII supply and demand British Medical Journal 23 August 1980 PRSE0000110. Part of it reads: “Although there are several outstanding exceptions, there is little doubt that unless those in charge of hospital blood banks are more successful in persuading clinical colleagues to use red-cell concentrates rather than whole blood in the management of the majority of routine hospital transfusions, the creation of major new plasma fractionations facilities will not be the salvation Dr Aronstam seeks.”
(673) Written Statement of Professor Stanislaw Urbaniak para 67 WITN6960001
(674) Dr Brian McClelland Transcript 27 January 2022 pp81-90 INQY1000177
(675) The uses of “almost” in these sentences refer to rare exceptions: the use of some foreign blood in London when the NHS was short and private hospitals in surplus (see above, and NETHRA Blood Transfusion Services with Special Reference to Hampstead, Bloomsbury and Islington 19 March 1986 SBTS0000618_160), and the very rare importation of blood of a very rare blood group which was simply not available within the UK.
(676) The need for it was apparent long before that – the failure to have a national oversight was for instance reflected by Professor Cash’s report into the particular problems of the main London blood transfusion centres; it resulted, as the chapter notes, in regions which were short of blood supplies borrowing from their neighbours in an ad hoc way.
(677) Note by the Joint Secretaries of the Central Committee for the National Blood Transfusion Service: Requirement for blood products and their availability October 1976 p3 DHSC0002181_045
(678) Gallo et al Detention, Isolation and Continuous Production of Cytopathic Retroviruses (HTLV-III) from Patients with AIDS and Pre-AIDS Science 4 May 1984 DHSC0000457
(679) Even today there is a risk that a unit of blood for transfusion will carry with it one of the hepatitis viruses, or even HIV but, thankfully, that risk is now so vanishingly small that it can routinely be ignored for all practical purposes.
(680) This was a response to impending war. The Scottish Blood Transfusion Service formally began on 11 January 1940, funded independently of England and Wales. Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine Vol 6 1996 pp11-24 NHBT0000028
(681) 1952 was the date of the report, which was mimeographed on 4 August 1952 (an early form of mass reproduction) and later published in March 1953. Dr MacCallum of the UK Virus Reference Laboratory, Public Health Laboratory Service was one of the experts (indeed, the rapporteur), and it can be presumed therefore that the UK knew of the conclusions. The other experts came from Sweden, the US, and the Netherlands. World Health Organization Expert Committee on Hepatitis Report March 1953 pp1-2 RLIT0000215
(682) World Health Organization Expert Committee on Hepatitis Report March 1952 p17 RLIT0000215
(683) This recommendation was prompted by the Committee’s concern that the dangers of serum hepatitis were not appreciated by many sections of the medical profession, and that many non-essential transfusions of blood and plasma were given. World Health Organization Expert Committee on Hepatitis Report March 1952 p17 RLIT0000215
(684) World Health Organization Expert Committee on Hepatitis Report March 1952 p18 RLIT0000215
(685) World Health Organization Expert Committee on Hepatitis Report March 1952 pp18-19 RLIT0000215
(686) World Health Organization Expert Committee on Hepatitis Report March 1952 p19 RLIT0000215. See the chapter on Pool Sizes.
(687) Of particular interest is footnote 10 which recognises the difficulty of avoiding large pool sizes when producing dried plasma and notes that if they are to be used “the committee stresses the need for special care in selecting donors and the introduction of effective inactivating techniques immediately they become available.” World Health Organization Expert Committee on Hepatitis Report March 1953 p19 RLIT0000215. See the chapter on Viral Inactivation.
(688) World Health Organization Expert Committee on Hepatitis Report March 1952 p20 RLIT0000215
(689) World Health Organization Expert Committee on Hepatitis Report March 1953 pp20-21 RLIT0000215. Reporting also helps to identify problems such as new or previously unsuspected infections. More recently identification of risks to health from transfusions has become organised as a system of haemovigilance, which is discussed further in the chapter on Blood Transfusion: Clinical Practice.
(690) For some such “donors” it was their only regular income: in effect, their livelihood.
(691) London transfusion centres were often hard pressed to obtain sufficient donations for the needs of the NHS, and for private hospitals in London (of which there were a significant number). This led to private hospitals often obtaining whole blood from abroad (probably in Europe, which were probably originally purchased from the donor). On occasion, the private hospitals were in surplus – blood has a short shelf life – and so transferred some to the NHS if it, the NHS, was then experiencing a temporary shortfall. The Inquiry has no more information about this than what comes from a report by Professor John Cash, though this is clearly a reliable source for this point. NETRHA Blood Transfusion Services with Special Reference to Hampstead Bloomsbury and Islington 19 March 1986 SBTS0000618_160. There is no suggestion that any similar practices arose outside London, and did so in London only because of its particular nature as a centre for private medical care, and it having an urban population which for demographic reasons was probably less inclined than elsewhere to give donations.
(692) There are three particular matters to mention. First, one participant remembered seeing a room in which there were blood bags which had markings on them showing that they came from the US and concluded that the blood was American. This is likely to have been an understandable misinterpretation. Blood bags were manufactured and marketed by Travenol (a US pharmaceutical company) and replaced bottles as containers for blood and plasma during the late 1960s to early 1970s. Without those, or blood bags made to the Fenwall system (again American), cryoprecipitate could not have been produced easily in a sterile manner. These bags had markings on them showing they were US produced; and it is possible that this led to misunderstanding that the label applied to the contents too. Second, in hospitals sited close to American military bases it is possible that the use by a nurse of the description “American blood” was accurate, but that what was being described was where the donor had come from rather than where the blood had been drawn. It is also unlikely for blood (as opposed to plasma) to have been imported, since until the 1980s anti-coagulants were such that they had to be used within 21 days of donation (later this became 35). Blood is a natural material, and like most such materials deteriorates over time so as to be past its useful date quite quickly. Third, plasma was imported on occasion. Shortly after the Second World War, Canadian plasma was imported for general use. This was, however, short-lived. When blood products made by the NHS were in short supply, attempts were made by commercial interests such as Speywood (for a while) to import plasma from abroad, but regulatory control stopped them (see the chapter on Regulation of Commercial Factor Concentrates).
(693) He became a Nobel prize-winner for his work in respect of hepatitis in blood. Alter et al The Ausria Test: Critical Evaluation of Sensitivity and Specificity Blood 6 December 1973 p11 RLIT0002022
(694) The text deals with surrogate testing which by definition implies that at the time of the test there is no test which will directly identify the presence of the virus of interest.
(695) Transaminases (ALT or AST) are indicative of some damage to liver cells, since they are released when liver cells break down.
(696) Unless the plasma is frozen fresh, though, the Factor 8 activity it contains will degrade relatively quickly. Although time-expired plasma has its uses, it is thus not something from which coagulation concentrates can be made.
(697) Written Statement of Professor Richard Tedder para 29 WITN3436003
(698) Professor Richard Tedder Transcript 13 October 2022 pp26 INQY1000255
(699) Bowley et al Blood Transfusion: A Guide to the Formation and Operation of a Transfusion Service 1971 p13 PRSE0002035. Edited by Drs Charles Bowley, Kenneth Goldsmith and William d’A Maycock in 1971. Dr Bowley was director of the Sheffield Regional Transfusion Centre; Dr Goldsmith was at the Medical Research Council (“MRC”) Blood Group Reference Laboratory and Dr Maycock was the Blood Products Laboratory (“BPL”) director and consultant adviser on blood transfusion to the Secretary of State.
(700) Bowley et al Blood Transfusion: A Guide to the Formation and Operation of a Transfusion Service 1971 p14 PRSE0002035
(701) Between January 1971 and December 1971, the Hepatitis B surface antigen (“HBsAg”) rate in prisons and borstals was 19 times higher than in donors overall and 5.7 times higher between January 1972 and June 1972. Letter from Dr John Barbara to Dr Angus Bird 31 August 1994 p2 JPAC0000002_039
(702) Minutes of Regional Transfusion Directors meeting 6 October 1971 pp4-5 NHBT0015758_001
(703) Dr Jack Darnborough of the East Anglia RTC and Dr John Wallace of the Glasgow and West RTC reported a greater incidence of hepatitis among prisoners. Minutes of Regional Transfusion Directors meeting 6 October 1971 pp4-5 NHBT0015758. An example of both knowledge of the likely source of hepatitis antigen discovered in blood, and concern about its prevalence, was expressed in a letter of 22 June 1972 from Dr Maycock to Dr Donald Smith of Wessex RTC. He noted “a fairly high incidence” of Hepatitis B [in donated blood which had been screened], unless Wessex had “an unusually high prison population”. Letter from Dr Maycock to Dr Donald Smith 22 June 1972 NHBT0108717_003
(704) Dr Wagstaff of the Trent RTC stopped the practice of collecting blood from prisoners shortly after he became director in July 1974. Written Statement of Dr William Wagstaff paras 53-54 WITN6988001
(705) The North London Blood Transfusion Centre stopped collecting blood from prisoners in 1973, having noted “HBsAg detection rates up to tenfold higher in donor sessions at prisons, compared with rates elsewhere.” Letter from Dr Barbara to Dr Angus Bird 31 August 1994 p1 JPAC0000002_039
(706) A survey in 1983 noted that prisons had not been used as a donor source in Cambridge for many years; however during an acute blood shortage in 1982 there had been a donor session in an open prison. The centre “discovered” many inmates were drug addicts and so did not go back for further sessions. Its policy in 1983 was not to use prisons but to reserve the right to do so in an emergency. Survey on the use of prisons as a source of donor blood at English and Welsh Regional Transfusion Centres p1 NHBT0008628_001
(707) Though the survey in 1983 noted that sessions were held in prisons by Tooting until 1979. Survey on the use of prisons as a source of donor blood at English and Welsh Regional Transfusion Centres p1 NHBT0008628_001
(708) Though the survey in 1983 noted that sessions were still being held in Cardiff prison in mid 1983. Survey on the use of prisons as a source of donor blood at English and Welsh Regional Transfusion Centres p1 NHBT0008628_001
(709) Though the survey in 1983 noted that sessions had been held in prisons by the Birmingham RTC until 1983. Survey on the use of prisons as a source of donor blood at English and Welsh Regional Transfusion Centres p1 NHBT0008628_001
(710) This seems unduly complacent, given that it was well known that the screening tests for Hepatitis B then in use traced only some 30-40% of infections.
(711) Minutes of Regional Transfusion Directors meeting 26 September 1973 pp7-8 NHBT0000086_002
(712) Reverse passive haemagglutination (“RPHA”) or radioimmunoassay (“RIA”). Letter from Dr Yellowlees to all regional medical officers 1 May 1975 p2 PRSE0000009
(713) Letter from Dr Yellowlees to all regional medical officers 1 May 1975 p2 PRSE0000009
(714) The International Society of Blood Transfusion criteria for the selection of blood donors advised against collection of blood from “inmates of a correctional institution” as one of nine general precautions to reduce the risk of viral hepatitis. Guidance on criteria for the selection of blood donors by International Society of Blood Transfusion 1976 p13 DHSC0002179_067. In 1978, the WHO Expert Committee on Biological Standardization produced requirements for the quality control of blood and blood products and recommended: “Donor populations showing a prevalence of acute or chronic hepatitis higher than that found in the general population should be avoided for collection both of single donor products (whole blood and its components) and of plasma for pooling for the manufacture of plasma fractions known to be capable of transmitting hepatitis, such as clotting factor concentrates.” WHO Expert Committee on Biological Standardization 1978 p26 PRSE0001264
(715) A small study testing Hepatitis B surface antibody and Hepatitis B core antigen identified six times as many donors testing positive in prisons compared to general donors. Barr et al Hepatitis B virus markers in blood donors in the west of Scotland Medical Laboratory Sciences 1981 p1, p3 PRSE0001035
(716) Memo from Paul Winstanley to J Brown 23 August 1983 p1 PRSE0004729. This was corroborated by Dr Tony Napier of the South Wales RTC who told the Inquiry that prior to the time it was decided to discontinue prison donations “it had been understood that encouraging prisoners to donate was helpful to them, it was, in a way, part of their rehabilitation in society, and it was a valuable practice to undertake.” Dr Tony Napier Transcript 30 November 2021 pp122-123 INQY1000163. Equally in Leeds the region had tried to “withdraw prison sessions, and got a very active response from the prisons, which asked that the sessions should continue.” Survey on the use of prisons as a source of donor blood at English and Welsh Regional Transfusion Centres p2 NHBT0008628_001
(717) Survey on the use of prisons as a source of donor blood at English and Welsh Regional Transfusion Centres pp1-2 NHBT0008628_001
(718) The South West RTC stopped collecting donations from prisons in January 1984. The reasons given to the prison governors for this was the “extremely high incidence of hepatitis carrier status” amongst the prison population and the relationship between a high hepatitis carrier status and AIDS. Letter from Dr Ian Fraser to Governor 11 November 1983 NHBT0091997. According to Dr Napier, prison donations ceased shortly after recognition of HIV in the UK when it became inadvisable to collect blood donations from prisoners. Written Statement of Dr Tony Napier para 74 WITN6915001
(719) Extract from Hansard written answer by Edwina Currie to question from Alf Dubs 11 February 1987 NHBT0057149_087
(720) Subject to statistical significance being demonstrated.
(721) In Professor Cash’s evidence to the Penrose Inquiry, he said that “Dr Anne Welsh (SNBTS) has kindly advised me that the following dates are the occasions of the last prison donors sessions: Aberdeen: 28/7/83 … Dundee: 2/8/83, Edinburgh: 7/4/80, Glasgow: 25/3/84, Inverness: 24/2/83”. Written Statement of Professor John Cash p2 PRSE0004484. In fact, the last prison donor session at Edinburgh was in December 1981. Dr Brian McClelland Penrose Inquiry Transcript 22 March 2011 p30 PRSE0006009
(722) Written Statement of Dr Robert Perry to the Penrose Inquiry 25 January 2011 pp5-6 PRSE0001823. What he did not deal with was the risk of NANBH.
(723) Minutes of SNBTS Directors meeting 29 March 1983 p5 PRSE0000193
(724) Minutes of SNBTS Directors meeting 8 December 1983 p4 PRSE0002899
(725) Written Statement of Professor John Cash to the Penrose Inquiry 25 January 2011 p2 PRSE0004484
(726) Penrose Inquiry Collection of Blood in Prisons 15 March 2011 p8 PRSE0002164
(727) Dr Morris McClelland Transcript 1 February 2022 pp110-111 INQY1000179
(728) Dr Colin Entwistle described the military sessions as “incredibly beneficial to the Service.” Dr Colin Entwistle Transcript 6 December 2021 p12 INQY1000167. Dr Patricia Hewitt of the North London Regional Transfusion Centre wrote to Dr Roger Moore in 1985 and said “we do … collect a large number of donations from MOD establishments.” Letter from Dr Hewitt to Dr Moore 6 August 1990 NHBT0002981
(729) Dr Donald Smith (Wessex RTC) observed in 1971 that: “The crews of many ships are volunteering as blood donors” and three years later asked his staff: “Please could you ask the team clerks, particularly at Naval sessions to enquire if there is any history of jaundice even if the donor has previously donated. Anyone with a history of jaundice will not be accepted but I will always write to them and explain that they can go on our research panel.” Minutes of Haemophilia Society Executive Committee meeting 9 December 1971 p5 HSOC0029691_142, Memo from Dr Donald Smith to Mr Duddridge 27 June 1974 NHBT0108948. It must be remembered that homosexual men, one of the principal groups told to self-exclude from giving blood, could not openly serve in the armed forces until 2000. Equally, anybody found guilty of intravenous drug use would also have been expelled.
(730) Dr Entwistle explained that, at the time, military sessions were not perceived to impose particular extra risks, whatever people might have thought subsequently. Dr Colin Entwistle Transcript 6 December 2021 p12 INQY1000167. This was a view shared by Professor Dame Marcela Contreras in her oral evidence. She was nonetheless able to and did design sessions to avoid military personnel being lined up to give donations by their senior officer, in common with her approach of finding effective ways to overcome what elsewhere could be problematic. Professor Dame Marcela Contreras Transcript 2 December 2021 pp100-101 INQY1000165
(731) Written submission of National Services Scotland Scottish National Blood Transfusion Service para 67 SUBS0000044
(732) Dr Jack Gillon Transcript 19 January 2022 pp20-22 INQY1000173
(733) Dr Morris McClelland Transcript 1 February 2022 pp111-112 INQY1000179
(734) Dr Morris McClelland Transcript 1 February 2022 pp111-112 INQY1000179
(735) For some centres, workplace sessions were an extremely important source of donations. For example in Northern Ireland. For the North London Centre in the 1980s half their donations came from such sessions. Dr Patricia Hewitt Transcript 9 December 2021 p22 INQY1000170
(736) Written Statement of Dr Tony Napier para 52 WITN6915001
(737) The North East Regional Transfusion Centre’s Clinical Service and Business Plan for 1991-92 showed that the number of registered donors at the Northern RTC fell from just below 150,000 in 1979/80 to just over 120,000 in 1989/90. In the same period, donors donating at their place of work reduced from around 52,500 to below 35,000. Written Statement of Dr Huw Lloyd para 16 WITN6935001, Chart showing number of registered donors WITN6935008. Dr Huw Lloyd also provided a chart showing a fall of 5% in the industrial donations as a percentage of all donors bled between 1985/86 and 1993/94, as well the unemployment rate. Graph showing Northern Region Blood Transfusion Service Industrial Donations as Percentage of All Donors Bled and Unemployment Rate WITN6935009
(738) Written Statement of Dr Morris McClelland para 14 WITN0892001
(739) A working assumption would probably be that if anything the rate was lower, for employers in industries requiring a large manual workforce would be unwilling to tolerate the weakening effects of any persistent viral infection. The “healthy worker” effect is recognised as a potentially distorting consideration when analysing epidemiological studies.
(740) Dr Brian McClelland Transcript 27 January 2022 p97 INQY1000177. NHSBT submission 16 December 2022 paras 5.36-5.39 SUBS0000062
(741) For example, the North London Blood Transfusion Centre by 1984 had two static clinics, one at the RTC in Edgware itself, and one in the West End. A third clinic in Luton was added later in 1988. Written Statement of Dr Patricia Hewitt para 26 WITN3101009
(742) Dr Vanessa Martlew recalled the opening of a sub-centre in Lancaster: “Plasma components are best prepared as soon as possible after donation. As the journey from Barrow in Furness to Manchester could take up to 4 hours, the location of a Blood Centre in Lancaster enhanced the quality of the plasma components produced in the region.” Written Statement of Dr Vanessa Martlew para 68 WITN4034001, Written Statement of Dr Huw Lloyd p24 WITN6935001. Dr Lloyd described a similar situation in the North East where “a new team was recruited in Cumbria with a small facility in Cockermouth rented for use as a base for the manager, and equipment storage. All new staff lived in the area.” Written Statement of Dr Huw Lloyd para 17(e) WITN6935001
(743) These machines first came significantly into service in the UK in the early 1980s. Initially there were debates about the respective merits of manual and machine plasmapheresis, the former having been the method more widely adopted prior to the early to mid 1980s.
(744) See for example: Dr Tony Napier Transcript 30 November 2021 p63 INQY1000163
(745) Dr Tony Napier Transcript 30 November 2021 p91 INQY1000163
(746) See for example: Written Statement of Dr William Wagstaff para 51 WITN6988001
(747) Note of meeting with Dr Patricia Hewitt Deputy Director of North London Blood Transfusion Centre p1 NHBT0019621
(748) Professor Dame Marcela Contreras Transcript 2 December 2021 p177 INQY1000165
(749) The Northern Region Blood Transfusion Service started to do this in 1990. See for example: Letter from Dr Lloyd to donors WITN6935020
(750) An example of “circumstances” was having travelled recently to a tropical country.
(751) Dr Entwistle said that at Oxford they would generally call 200 donors to a session and get a 50% response rate plus about 10% walk-ins. In Cambridge at a military session they may have had as many as 240 donors. Dr Colin Entwistle Transcript 6 December 2021 p29, p12, INQY1000167. Dr Morris McClelland explained that if a session was held at a factory or a workplace, they would have many more donors than if it were held in other community locations. Dr Morris McClelland Transcript 1 February 2022 p9 INQY1000179. Dr Brian McClelland estimated that the proportion of new donors was always around 20%. Dr Brian McClelland Transcript 27 January 2022 p91 INQY1000177
(752) Dr Napier’s expectation was that the guidelines would be at every session to guide staff on the selection criteria. Dr Tony Napier Transcript 30 November 2021 pp96-97 INQY1000163
(753) This was the evidence given by Dr Napier and Dr Entwistle. Dr Tony Napier Transcript 30 November 2021 pp98-102 INQY1000163, Dr Colin Entwistle Transcript 6 December 2021 pp10-11, pp55-63, p83 INQY1000167. From 1946, the guidance issued to the RTCs was to the effect that donors presenting for the first time (only) should be asked specific questions about a number of infectious diseases which included hepatitis and jaundice. The responses given by the donor were to be committed to paper and signed by the donor. Medical Examination and Care of Donors p1 DHSC0100027_069. By 1951, the procedure had been changed so that at subsequent donation sessions donors were to be provided with a leaflet setting out a list of diseases and health conditions that rendered a donor ineligible, and another list of diseases and health conditions which the donor was asked to disclose so that a decision about eligibility could be made by the doctor. Donors were then asked to sign the NBTS 110 form affirming that they had read this information. The Selection, Medical Examination, and Care of Blood Donors p1 DHSC0100027_146. This remained the procedure until the Red Book was published in 1989, which stated that donors should be questioned about these matters at all donor sessions. Department of Health Guidelines for the Blood Transfusion Services in the United Kingdom September 1989 p25 NHBT0000027_030
(754) It was Dr Hewitt’s evidence that the clerk would “point out to the donor the conditions listed on the form and ask whether any of those applied, and if they did, then the clerk would refer the donor to the medical officer.” Dr Patricia Hewitt Transcript 9 December 2021 p57 INQY1000170
(755) Dr Gamal Gabra Transcript 3 February 2022 pp39-40 INQY1000180. Face-to-face donor interviews had been trialled in the Edinburgh and South East Scotland Centre in 1982 for all donors, but there were insufficient staff and it did not work. They were reintroduced in 1992 by Dr Gillon for new donors. Dr Brian McClelland Transcript 27 January 2022 pp34-37 INQY1000177. This was then rolled out to the rest of the Scottish centres over the next five years. It required a private area for the interviews to take place. It was Dr Gillon’s oral evidence that it was a lack of resources which had meant that these were not introduced earlier. Dr Jack Gillon Transcript 19 January 2022 pp62-66 INQY1000173
(756) Dr Jack Gillon Transcript 19 January 2022 p41 INQY1000173
(757) At a meeting of regional transfusion directors in October 1984 it was noted that: “Much of the screening at present is done by the clerical officers and donor attendants according to the set Guidelines before the donor sees the doctor, whose time is amost [sic] entirely occupied in performing venepunctures.” Minutes of Regional Transfusion Directors meeting 10 October 1984 p4 CBLA0001905
(758) The 1985 version: NBTS 110 Form 1985 DHSC0002277_068. The 1979 version did not contain this anomaly, asking about both jaundice and hepatitis. Memo on the Selection, Medical Examination and Care of Blood Donors December 1977 p11 DHSC0003734_066. “Jaundice” was not a universal sign of hepatitis infections, for many were “anicteric” (ie there was no yellowing of the skin).
(759) A qualified doctor. From 1985 the North East Thames Regional Transfusion Centre began to replace medical officers with clinical nurse specialists. This was taken up by other RTCs so that by the early 1990s, the medical officer had been replaced by clinical nurse specialists. Written Statement of Dr Jean Harrison paras 38-45 WITN7046001. See also: Harrison Nurses in the Transfusion Service The Lancet 14 November 1987SBTS0004256_114, Dr Patricia Hewitt Transcript 9 December 2021 p24 INQY1000170
(760) Dr Entwistle in his oral evidence accepted that these discussions would be taking place in an “open forum”. Dr Colin Entwistle Transcript 6 December 2021 p59 INQY1000167
(761) See for example the evidence of Dr Lloyd that the Northern RTC took screens to their community sessions. Dr Huw Lloyd Transcript 8 February 2022 pp173-174 INQY1000182, Dr Gamal Gabra Transcript 3 February 2022 pp40-41 INQY1000180
(762) Dr Lorna Williamson Transcript 8 December 2021 p34 INQY1000169
(763) Written Statement of Professor Dame Marcela Contreras paras 254-256 WITN571101, Professor Dame Marcela Contreras Transcript 2 December 2021 pp75-78 INQY1000165
(764) “If a donor reports having had a recent illness or course of medication, brief notes of this are written onto a page of a duplicate notebook, alongside the donation number, and at the end of this session, this sheet, known as the ‘Illness Sheet’, accompanies the blood to the Blood Components section, where it is used to identify unsuitable donations.” Medicines Inspectorate Inspector’s Summary 22 November 1989 p4 NHBT0006234. Those illness sheets were passed to one of the medical staff whose job it was to go through them, compare it to the known criteria for donation, and in some cases to put the donation on hold while further enquiries were made of the donor’s general practitioner. Dr Huw Lloyd Transcript 8 February 2022 pp101-103 INQY1000182. Later on in 1993 this procedure was changed as the view was taken that it was unethical to take a donation from a donor that may not be used. Northern Region Blood Transfusion Service Selection of Donors Booklet December 1993 p5 NHBT0007498
(765) Memo from Jean MacDonald to all donor staff 21 November 1984 p1 PRSE0003001. Dr Gillon explained that he stopped that practice in April 1985. Dr Jack Gillon Transcript 19 January 2022 pp45-48 INQY1000173. See his memo: Memo from Dr Gillon to Jean MacDonald 10 April 1985 PRSE0001092
(766) By July 1985 North London Blood Transfusion Centre had implemented an additional confidential questionnaire for donors to fill in about the risk of HIV/AIDS. Donors were also informed that they could speak confidentially to the medical officer if they had any questions or concerns. The medical officer would send a confidential note back to the North London Blood Transfusion Centre medical team, who would follow up any issues with the individual and offer appropriate advice. Dr Patricia Hewitt Transcript 9 December 2021 pp71-72 INQY1000170. In addition, by 1989, the North London Blood Transfusion Centre had private booths for donors to complete questionnaires about risk factors.
(767) Professor Dame Marcela Contreras Transcript 2 December 2021 pp75-78 INQY1000165, Dr Patricia Hewitt Transcript 9 December 2021 pp76-85 INQY1000170. See also a letter from Dr T Davies to staff setting out the procedure in May 1983: Letter from Dr Davies to all medical officers 23 May 1973 NHBT0109173
(768) Medical Examination and Care of Donors DHSC0100027_069
(769) Minutes of National Directorate of the NBTS National Provision of Donors Committee meeting 10 October 1990 p6 NHBT0097472_052, Boralessa and Harrison Senior citizens donors: a valuable group Transfusion Today October 1991 WITN7046005
(770) National Blood Authority Medical Assessment of Donors December 1993 p4 NHBT0059480_077
(771) Minutes of Regional Transfusion Directors meeting 18 January 1989 p5 NHBT0018188
(772) Minutes of National Regional Transfusion Service Donor Organisers and Donor Services Managers meeting 1 June 1990 p1 NHBT0118157_012
(773) Written Statement of Dr Morris McClelland para 14 WITN0892001
(774) Written Statement of Dr Huw Lloyd para 17(c) WITN6935001
(775) Letter from Dr Lloyd to donors p1 WITN6935020
(776) Minutes of the National Directorate of the NBTS National Management Committee meeting 16 April 1991 p7 NHBT0000191_144. The standard is now 12 weeks for men and 16 for women. This difference is because men generally have higher iron levels than women (they do not lose blood naturally as women of child-bearing age do).
(777) Medical Examination and Care of Donors p1 DHSC0100027_069
(778) See above.
(779) Medical Examination and Care of Donors p2 DHSC0100027_069
(780) “The experienced doctor can detect at a glance the potentially unsuitable donor” is in the editions from 1946: Medical Examination and Care of Donors p1 DHSC0100027_069, 1951: The Selection, Medical Examination, and Care of Blood Donors p2 DHSC0100027_146, 1960: Memorandum on the Selection, Medical Examination, and Care of Blood Donors April 1960 p2 DHSC0100027_008, 1963: Memorandum on the Selection, Medical Examination, and Care of Blood Donors December 1963 p3 DHSC0003734_110, and 1977: Memorandum on the Selection, Medical Examination and Care of Blood Donors December 1977 p4 PRSE0004358. The 1983 edition has the modified text: “The experienced doctor can detect many potentially unsuitable donors at a glance.” Guidance for the Selection, Medical Examination and Care of Blood Donors 1983 p7 NHBT0053225. This was retained in the 1985 edition. Guidance for the Selection, Medical Examination and Care of Blood Donors 1985 p8 DHSC0046337
(781) See for example Dr Brian McClelland Transcript 27 January 2022 pp99-100 INQY1000177. The claim that one can tell suitability for donation simply by looking may be true if there are obvious needle marks on an arm, but otherwise it is apt to give rise to a wide range of unreliable socio-economic prejudices.
(782) No specific donor selection criteria were published in Northern Ireland. Dr Morris McClelland explained that Northern Ireland used the English and then the UK-wide selection criteria (albeit he thought in the mid to late 1980s Northern Ireland had started producing their own donor questionnaires and their own alphabetic guidelines). In fact he stated that as a result of direct rule, “the policies adopted in London, almost invariably, I would say, certainly anything that affected NIBTS [Northern Ireland Blood Transfusion Service] followed the policy in London.” Dr Morris McClelland Transcript 1 February 2022 pp30-31 INQY1000179
(783) Medical Examination and Care of Donors p1 DHSC0100027_069. This was modified in 1951 to 12 months. The Selection, Medical Examination, and Care of Blood Donors p1 DHSC0100027_146
(784) Dr Maycock understood that the Expert Committee’s recommendation would be that blood from donors with a history of jaundice “at any time” should not be included in plasma pools, and that blood from such donors should only be used for emergency whole blood transfusions if the results of the serum bilirubin tests fell within normal limits. Letter from Dr Maycock to unknown 6 August 1952 DHSC0100011_222. The final text of the recommendation was: “the committee advises that, when circumstances permit, no person should be accepted as a blood-donor if there is a history of hepatitis (jaundice) at any time. However, circumstances will arise in which it may be necessary to accept as a blood-donor a person with hepatitis (jaundice). Under these circumstances, the committee recommends that (1) no donor should be accepted, except in case of life-saving emergency for a single transfusion, if he has a history of hepatitis (jaundice) within one year; (2) if the donor has a history of hepatitis (jaundice) more than one year before, liver-function tests should be performed; (3) the blood from a donor with a history of hepatitis (jaundice) should not be used in the preparation of large plasma pools until methods of sterilization are available.” World Health Organization Expert Committee on Hepatitis Report March 1953 pp18-19 RLIT0000215
(785) Minutes of the Regional Transfusion Directors meeting 1 October 1952 pp1-2 NHBT0017683
(786) Albeit at the meeting of RTDs of 8 July 1959 it was agreed that those with a history of jaundice at birth or obstructive jaundice (not viral) could be accepted as donors. Minutes of Regional Transfusion Directors meeting 8 July 1959 p4 NHBT0018374. This change is reflected in the April 1960 publication of Memorandum on the Selection, Medical Examination, and Care of Donors April 1960 p2 DHSC0100027_278, Memorandum on the Selection, Medical Examination and Care of Blood Donors April 1960 p1 DHSC0100027_009. The 1963 version also excluded those who had “been in contact with a case of hepatitis” in the previous six months, as well as those who had received transfusions of blood or plasma in the preceding six months. Memorandum on the Selection, Medical Examination, and Care of Blood Donors December 1963 p6 DHSC0003734_110
(787) Letter from Department of Health and Social Security to regional health authorities November 1976 p1 DHSC0002181_051. The rationale for the change is explored in a report dated July 1976 from the Advisory Group on Testing for the Presence of Hepatitis B Surface Antigen and did not stand in isolation since it was consistent with a recommendation in a WHO Technical Report on Viral Hepatitis. Second Report of the Advisory Group on Testing for the Presence of Hepatitis B Surface Antigen July 1976 PRSE0001579, WHO Technical Report Series Viral Hepatitis Report of a WHO Meeting 1975 DHSC0100002_015
(788) Memorandum on the Selection, Medical Examination and Care of Blood Donors December 1977 p3 DHSC0003734_066. It is worth noting that the material provided to the blood donors (by way of the leaflet NBTS 110A and the form to fill in and sign, NBTS 110) asked the donor who had suffered from jaundice or hepatitis in the preceding year or had contact with it in the preceding six months only to declare it so a decision could be made about donating. In other words, a donor who had suffered from jaundice or hepatitis more than a year ago did not have to make any declaration and so would automatically be bled. Memorandum on the Selection, Medical Examination and Care of Blood Donors December 1977 pp11-12 DHSC0003734_066. An example of this criteria in action is the letter to a donor sent in March 1979. Letter from Anon to Dr Donald Smith 3 April 1979 NHBT0112218
(789) In 1983 and again in 1985: Guidance for the Selection, Medical Examination and Care of Blood Donors 1983 p11 NHBT0053225, Guidance for the Selection Medical Examination and Care of Blood Donors 1985 p12 DHSC0046337
(790) Although the wording of the 1987 version differed from the previous two iterations, making it clear that a donor with a history of childhood jaundice could be accepted, but a donor with a history of jaundice or hepatitis that was not Hepatitis B could be accepted one year after recovery. Guidance for the Selection, Medical Examination and Care of Blood Donors November 1987 p9 PRSE0004115
(791) At the meeting on 22 May 1989 the Advisory Committee on the Virological Safety Blood advised the NBTS to reconsider its acceptance of donors who had had jaundice 12 months ago and that anti-HBc testing was recommended before acceptance. Minutes of Advisory Committee on the Virological Safety of Blood meeting 22 May 1989 p3 NHBT0005019. Despite this, the first edition of the Guidelines for the Blood Transfusion Services in the UK published in September 1989 (also known as the “Red Book”) did not include this provision. Department of Health Guidelines for the Blood Transfusion Services in the United Kingdom September 1989 p28 NHBT0000027_030. The second edition published in 1994 had a revised procedure, though not as recommended. Guidelines for the Blood Transfusion Service 1994 p29 NHBT0054484_003
(792) Letter from Department of Health and Social Security to regional health authorities November 1976 p1 DHSC0002181_051
(793) See the chapter on Hepatitis C Surrogate Screening.
(794) From March 1981. Dr Colin Entwistle Transcript 6 December 2021 p4 INQY1000167
(795) Dr Colin Entwistle Transcript 6 December 2021 pp60-67 INQY1000167. In their submission NBTS concluded: “It may well be that the memorandum did not keep track with the practice on the ground … insofar as the failure to update the guideline document in line with developing knowledge led to infection the blood service apologises.” The Infected Blood Inquiry NHSBT: Closing Submissions para 5.30 SUBS0000062
(796) There may be a place for such an approach where the intention is to improve matters by a series of steps, each building upon the basis that no one would now disagree that the next step was one which should not be taken, so as progressively to raise the floor by consent: elsewhere in this Report there are examples of this being successfully achieved, especially in respect of the better use of blood. However, it seems doubtful that such an approach is appropriate where the safety of blood itself is in issue. Then best practice, so far as safety is concerned, should always be the only practice to be sought.
(797) Guidance for the Selection, Medical Examination and Care of Blood Donors 1983 p11 NHBT0053225, Guidance for the Selection, Medical Examination and Care of Blood Donors 1985 p12 DHSC0046337
(798) Guidance on criteria for the selection of blood donors by International Society of Blood Transfusion 1976 p12 DHSC0002179_067
(799) Recommendations of the Committee of Ministers to Member States R (83) 8 23 June 1983 p3 NHBT0010651_004
(800) Memorandum on the Selection, Medical Examination, and Care of Blood Donors April 1960 p1 DHSC0100027_008. This recognised that transfusions risked transmitting disease, but the six-month exclusion would not lead to the rejection of those who had chronic infection as a result of previous transfusion, where there had been no symptoms that had called for liver function tests in the six-month period, nor would it lead to excluding those who were in a carrier state so far as their virus was concerned.
(801) Dr Tony Napier Transcript 30 November 2021 pp102-103 INQY1000163
(802) Memorandum on the Selection, Medical Examination and Care of Blood Donors December 1977 p5 PRSE0004358. This also found its way into the 1983 and 1985 guidelines: Guidance for the Selection, Medical Examination and Care of Blood Donors 1983 p8 NHBT0053225, Guidance for the Selection, Medical Examination and Care of Blood Donors 1985 p9 DHSC0046337
(803) See below.
(804) Dr Patricia Hewitt Transcript 9 December 2021 p92 INQY1000170
(805) Dr Morris McClelland Transcript 1 February 2022 pp112-113 INQY1000179
(806) A letter in The Lancet dated March 1980 authored by (among others) Dr Brian McClelland recorded the findings of a study of the prevalence of HBsAg in 9,257 new donors. HBsAg was detected in 1 of 792 with a history of jaundice. The letter noted “the viruses of ‘non-A, non-B hepatitis’ may be a significant cause of jaundice in this population.” McClelland et al Viral hepatitis markers in blood donors with history of jaundice The Lancet 15 March 1980 p2 NHBT0096823
(807) Dr Brian McClelland Transcript 27 January 2022 pp97-107 INQY1000177
(808) Responses to Medicines Inspectors Report South East Scotland Blood Transfusion Service 12 January 1983 pp31-65 WITN6666017
(809) Responses to Medicines Inspectors Report South East Scotland Blood Transfusion Service 12 January 1983 p47 WITN6666017
(810) Dr Brian McClelland Transcript 27 January 2022 p42 INQY1000177
(811) Responses to Medicines Inspectors Report South East Scotland Blood Transfusion Service 12 January 1983 p43 WITN6666017
(812) Responses to Medicines Inspectors Report South East Scotland Blood Transfusion Service 12 January 1983 p43 WITN6666017
(813) Dr Brian McClelland Transcript 27 January 2022 pp45-47, pp112-113 INQY1000177
(814) Minutes of Scottish National Blood Transfusion Service meeting 30 April 1986 p1 PRSE0001653
(815) Guidance for the Selection, Medical Examination and Care of Blood Donors November 1987 PRSE0004115
(816) The guidelines were updated in November 1988 and August 1990 but these parts did not change materially. Guidance for the Selection of Blood Donors November 1988 PRSE0001327, Guidance for the Selection of Blood Donors August 1990 PRSE0002677
(817) Its full title is “Guidelines for the Blood Transfusion Services in the United Kingdom”.
(818) Department of Health Guidelines for the Blood Transfusion Services in the United Kingdom September 1989 p28 NHBT0000027_030
(819) Guidelines for the Blood Transfusion Service 1994 pp40-234 NHBT0054484_003. Published in 1993, but with a foreword written in October 1992.
(820) Guidelines for the Blood Transfusion Service 1994 p72 NHBT0054484_003
(821) There is no evidence it was put this way to any would-be donor.
(822) Dr Brian McClelland Transcript 27 January 2022 pp34-38 INQY1000177
(823) In what could be a confidential manner, eg the “polling booth” approach adopted at the North West Thames RTC by Dr Contreras.
(824) The submissions made on behalf of core participants represented by Collins Solicitors include that “the transfusion services were remiss in delaying screening of donors by direct confidential questioning of their private lives. Such was a simple, effective precaution, that could have been easily implemented earl;y [sic] on, without causing offence if delivered appropriately.” Submissions on behalf of the Core Participants represented by Collins Solicitors para 636 SUBS0000063. In the light of Dr Brian McClelland’s evidence the implementation of direct confidential questioning would not necessarily have been easy, and needed resourcing, but this submission is a powerful argument that there should have been at least greater consideration of taking such a step, probably by the funding authorities, given that it was a major part of the front line in the defence against infection with the cause of AIDS.
(825) Central Management Services Blood: Record Keeping and Stock Control 1982 DHSC0002221_011
(826) The particular recommendations were as follows:
“148. It is recommended that [RTCs] consider as part of their role a formal process to enable the exchange of ideas and good practice at operational level for hospitals to whom they supply substantial quantities of blood and blood products.”
“149. It is recommended that discussion on a formal basis – say annual or 6 monthly – between the medical staff or Director at the Centre and the hospital based haematologist in charge of the blood bank is considered with a view to sharing problems and good practice experienced in blood banking.”
“160: It is recommended that haematologists in charge of blood banks are asked to ensure that they discuss with their medical colleagues economies in blood usage. (Blood products – although not found to be such a problem – should be considered too.)” Central Management Services Blood: Record Keeping and Stock Control 1982 pp30-31 DHSC0002221_011
(827) Letter from Stanley Godfrey to regional and district administrators and others 28 February 1983 p2 NHBT0000476
(828) NBTS Co-ordinating Committee Status Report from the National Director 15 June 1989 p3 NHBT0010493_001
(829) Letter from Dr George Bird to Dr Maycock DHSC0100028_094, Birmingham Blood Transfusion Service Table of Units of Blood Issued and Returned: 1971 8 February 1972 DHSC0100028_095, Letter from Dr Maycock to Dr George Bird 14 April 1972 DHSC0100028_107, Letter from Dr George Bird to Dr Maycock 18 April 1972 DHSC0100028_108
(830) Letter from Dr Ala to regional administrators 28 October 1985 DHSC0041318_095. The way these worked was for the clinician to say, when requisitioning a supply from the RTC, what they needed the blood for. The RTC would know the range of volumes which different clinicians ordered for what on paper appeared to be the same condition. They would set a figure which represented a reasonable maximum, and seek to have the clinician justify any higher figure. The clinician would by this means learn what the general approach of others in their specialty was: if their figure was higher, they might then effectively be shamed into realising that they were high users, and moderate their demands or at least reflect on whether the amounts they habitually used were justified.
(831) Dr Lorna Williamson Transcript 8 December 2021 pp17-18 INQY1000169
(832) Dr William Wagstaff Transcript 25 January 2022 pp118-119 INQY1000175. He added that it was the haematologists who were influential in “impressing on their surgical colleagues that minimum acceptable levels of haemoglobin had originally been set much higher than necessary”.
(833) Dr Frank Boulton Transcript 4 February 2022 pp145-146 INQY1000181
(834) Dr Vanessa Martlew Transcript 20 January 2022 pp43-44 INQY1000174
(835) Written Statement of Professor Dame Marcela Contreras 14 October 2021 paras 367-375 WITN5711001, Professor Dame Marcela Contreras Transcript 2 December 2021 pp153-160 INQY1000165
(836) Dr Colin Entwistle Transcript 6 December 2021 p49 INQY1000167
(837) Dr Colin Entwistle Transcript 6 December 2021 p33 INQY1000167
(838) Recommendations of the Central Management Services Report (CMS.A.7/82): “Blood: Record Keeping and Stock Control” February 1983 p2 PRSE0000525
(839) Dr Gabra was director for the West of Scotland 1980-89. Written Statement of Dr Gamal Gabra para 70 WITN5495001
(840) Written Statement of Professor Stanislaw Urbaniak para 80 WITN6960001
(841) Dr Boulton was deputy director for Edinburgh and South East Scotland. Dr Frank Boulton Transcript 4 February 2022 pp73-77 INQY1000181
(842) Written Statement of Dr Morris McClelland para 32 WITN0892001
(843) Written Statement of Dr Morris McClelland para 32 WITN0892001, Dr Morris McClelland Transcript 1 February 2022 p82 INQY1000179
(844) See the chapter on Blood Transfusion: Clinical Practice. It should be noted that “giving less” includes giving none, where it is unnecessary to give a transfusion at all.
(845) See the chapter on Haemophilia Centres: Policies and Practice.
(846) See for example Professor Brian Edwards from the Trent RHA describing “the long-standing principle of clinical freedom, which I understand was part of the deal struck between ministers and the medical profession when the NHS was first started” as a reason for not seeking to influence other doctors. Written Statement of Professor Brian Edwards para 63 WITN7641001
(847) Letter from Dr Bowley to colleagues 17 December 1973 p1 CBLA0000171. His arguments were unsuccessful in persuading haemophilia centre directors at a joint meeting with RTDs on 31 January 1974. Minutes of Haemophilia Centre Directors and Blood Transfusion Directors joint meeting 31 January 1974 pp5-6 CBLA0000187. He died in the Paris air crash that July and his deputy, Dr Wagstaff, succeeded him.
(848) Written Statement of Dr William Wagstaff paras 164-169 WITN6988001, Dr William Wagstaff Transcript 25 January 2022 pp56-57 INQY1000175. There is also evidence that the RTCs did try to promote BPL products over commercial, for example at the East Anglia RTC. Dr Lorna Williamson Transcript 8 December 2021 pp47-50 INQY1000169. Also the Yorkshire RTC: Letter from Dr Angela Robinson to Dr Gunson 2 March 1990 NHBT0097035_069, Yorkshire Blood Transfusion Service Business Plan 1991/1992 November 1991 NHBT0097056_002. The Trent RHA used “Considerable persuasion” in 1991 to try to get the Sheffield haemophilia clinicians to use BPL products, but this was on grounds of cost rather than safety. Written Statement of Professor Brian Edwards para 63 WITN7641001, Plasma and Fractionated Blood Products and associated Blood Bags p6 WITN7641006
(849) Dr Entwistle (Oxford) said they could have made the switch away from providing plasma to BPL to producing cryoprecipitate in a matter of days. Dr Colin Entwistle Transcript 6 December 2021 p26 INQY1000167. Dr Brian McClelland (Edinburgh) said “it could have been done very quickly. We would have had … enormous community support in doing that, which would have made it go very quickly.” Dr Brian McClelland Transcript 27 January 2022 p132 INQY1000177. Dr Morris McClelland (Belfast) said it would have been possible to reprioritise production. Dr Morris McClelland Transcript 1 February 2022 pp115-116 INQY1000179. Dr Harrison (North East Thames) in her statement said that the North East Thames Regional Transfusion Centre would have been able to increase their production of cryoprecipitate very quickly, but there would not have been enough plasma to treat all people with bleeding disorders with cryoprecipitate, and so the patients may have had to accept being treated in response to a bleed rather than prophylactically. Written Statement of Dr Jean Harrison paras 198-199 WITN7046001
When asked if it would have been possible to increase cryoprecipitate as an interim measure in response to the AIDS crisis, Professor Contreras (North London) said: “To a large extent, but we were not asked to do it. But we had the capability to do it.” Professor Dame Marcela Contreras Transcript 2 December 2021 pp149-150 INQY1000165. Dr Napier (Cardiff) said that if Professor Arthur Bloom had asked the Cardiff RTC to “switch emphasis totally from concentrate towards cryoprecipitate, we would have done our best to put that into place.” Dr Tony Napier Transcript 30 November 2021 p180 INQY1000163. Dr Wagstaff said one of the reasons for meeting haemophilia clinicians was to discuss whether “they wanted to change back to cryoprecipitate away from concentrate until the question of infectivity was sorted out” and that it caused him “some discomfort” that they did not since they could have provided enough cryoprecipitate to meet demands. Written Statement of Dr William Wagstaff paras 165-167, para 192 WITN6988001. He could have met any increased demand for cryoprecipitate “in weeks rather than months”. Dr William Wagstaff Transcript 25 January 2022 p48 INQY1000175
(850) The high point of the evidence was in respect of the Yorkshire RTC. In 1983 Dr Margaret Swinburne, the then director of the Leeds Haemophilia Centre asked Dr Derrick Tovey, director of Yorkshire RTC, to maintain the supply of cryoprecipitate because of AIDS. Letter from Dr Swinburne to Dr Liakat Parapia 7 July 1983 PARA0000015. As soon as the Yorkshire RTC became aware (in about June 1983) that people with haemophilia not previously treated were to be given cryoprecipitate, Dr Robinson made sure that all cryoprecipitate was made out of the donations of a second-time donor, so that the donor would have been tested twice before the cryoprecipitate was released for use. Written Statement of Dr Angela Robinson paras 286-287 WITN6926001. But there is no evidence of Yorkshire RTC being asked to increase production (and Dr Robinson in her statement recalls no such request) until 1989 when Yorkshire RTC experienced a doubling in the demand from local hospitals for cryoprecipitate and fresh frozen plasma. Notes on visit to Yorkshire RTC by Dr Gunson 24 August 1989 p1 NHBT0003366. Dr Robinson in her statement was clear that had they been asked to switch entirely to the production of cryoprecipitate this could have been done with some restructuring, some capital outlay and some restaffing. Written Statement of Dr Angela Robinson paras 102-105 WITN6926001
(851) Almost all of the treatment in Northern Ireland was with commercial Factor 8 products.
(852) Dr Morris McClelland Transcript 1 February 2022 p67 INQY1000179
(853) Dr Morris McClelland Transcript 1 February 2022 pp115-116 INQY1000179, Written Statement of Dr Morris McClelland para 54(e) WITN0892001
(854) Cash and Spencely Haemophilia A and the blood transfusion service: a Scottish study British Medical Journal 18 September 1976 p2 PRSE0003425
(855) Minutes of SNBTS Directors and Haemophilia Directors meeting 30 January 1981 p2 PRSE0000144
(856) Note of Haemophilia and Blood Transfusion Working Group meeting 4 March 1981 p2 SBTS0000382_008
(857) Minutes of SNBTS Directors and Haemophilia Directors meeting 2 February 1984 p2 PRSE0001556
(858) Draft of Acquired Immune Deficiency Syndrome and Transfusion 5 December 1983 p25 WITN6666011, Dr Brian McClelland Transcript 27 January 2022 p154 INQY1000177
(859) Concerns were also raised by Dr Boulton while he was at the Edinburgh RTC, of Dr Christopher Ludlam’s prescribing practice, in particular that he was using too much Factor 8. These concerns were however based not on the risks to the patient from exposure to large pool products but because Dr Ludlam’s use of Factor 8 was more than his allocation of PFC product, and there was a risk that he may have to start using commercial products. Letter from Dr Boulton to Dr Ludlam 10 May 1982 pp1-3 PRSE0003044, Letter from Dr Brian McClelland to Dr Cash 2 February 1983 PRSE0003653. The reason Dr Boulton and Dr Brian McClelland considered it important to stay away from commercial products was because it was their “hope and expectation that products made from indigenous donor plasma would carry less risk of importing new infections.” Dr Brian McClelland Transcript 27 January 2022 p79 INQY1000177. See also the chapter on Haemophilia Centres: Policies and Practice.
(860) Table of Abstract of Workload Statistics 1959-1986 WITN6960006
(861) Dr Gamal Gabra Transcript 3 February 2022 p60 INQY1000180
(862) See for example Dr Hewitt’s account of the practice at the North London Blood Transfusion Centre: “Blood and plasma taken from donors is put in ‘quarantine’ at the Centre. The blood will then stay there until it has been tested.” Note of meeting with Dr Patricia Hewitt Deputy Director of North London Blood Transfusion Centre p8 NHBT0019621
(863) For example the North East Thames Regional Transfusion Centre informed hospitals that they had received donations from donors who had tested positive for viruses such as HIV. Letter from Dr S Knowles to Dr D Lewis 9 April 1986 NHBT0027607
(864) Procedures for Investigation of Reported Possible Transfusion Transmitted Hepatitis NHBT0005372_002
(865) There does appear to have been a system for quarantining plasmapheresis donations at the Oxford RTC by keeping donations in quarantine, frozen both at the centre prior to shipping to BPL, and for several months at BPL before fractionation so as to reduce the risk from any HIV “window” infection of plasma for fractionation. Dr Entwistle in a draft statement for the HIV litigation suggested therefore that there was a good chance that plasma from a previous donation would be held in quarantine before being pooled and fractionated. Report on plasma collection and response to AIDS and testing by Dr Colin Entwistle 4 January 1990 pp6-7 NHBT0019630_003
(866) For example Dr Tovey reported a potentially infected donation to BPL. Letter from Dr Tovey to B Combridge 15 July 1981 NHBT0105340. The North London Blood Transfusion Centre set out the test it applied for making such a report to BPL: “We only report cases to BPL when we have assured ourselves that a report from a hospital concerning hepatitis in a transfusion recipient is likely to be associated with the transfusion. Thus, if more than 6 months has elapsed after transfusion before the development of hepatitis B, then we (not the clinicians) decide that transfusion is not responsible for the infection. We do not start an enquiry and do not notify BPL. For example, yesterday I received notification of a case where 10 months had elapsed. I have asked the hospital to clarify the dates given, and if they confirm these as true then there will be no enquiry and BPL will never know about it!” Original emphasis. Letter from Dr Hewitt to Dr Moore6 June 1990 NHBT0003772. See also Dr Hewitt’s oral evidence: Dr Patricia Hewitt Transcript 9 December 2021 pp129-133 INQY1000170
(867) Letter from Dr Terry Snape to Dr Napier 26 July 1985 DHSC0002273_021. The RTCs were not themselves expected to trace and inform the recipients of infected donations of their infection. Instead, this was the responsibility of their treating clinicians. See the procedure outlined by the Expert Advisory Group on AIDS (“EAGA”) at a meeting on 29 May 1985, which involved the RTC informing the haematologist in charge of the blood bank about a suspect donation and asking them to identify the recipient of that suspect donation so that the clinician in charge of that patient could be informed and then determine what subsequent investigations should be undertaken. Minutes of Expert Advisory Group on AIDS meeting 30 July 1985 p5 PRSE0002628
(868) See the chapters on HIV Lookback and Hepatitis C Lookback.
(869) DHSS Information for Doctors Concerning the Introduction of the HTLV III Antibody Test October 1985 p4 DHSC0000177
(870) Detailed evidence was given by Professor Contreras and Dr Hewitt as to the procedure for donors who had tested positive for HTLV-3. They would be sent a bland letter asking them to make an appointment. The letter was timed so that it arrived early in the week. The donor would be seen in private by either Dr Hewitt or her colleague, both of whom had received training from St Mary’s hospital in West London on counselling those infected with HIV. The RTC would then make a referral to a specialist centre, whether that was the donor’s local centre or one of the big London ones. The RTC did not communicate with the GP at all, but did impress upon the donor the importance of informing their GP. Dr Patricia Hewitt Transcript 9 December 2021 pp96-103 INQY1000170
(871) Letter from Dr Tovey to Anon 14 June 1982 NHBT0030477_045. Their GP was also told (with donor consent). Letter from Dr Tovey to Dr C Peat 21 January 1980 NHBT0030476_208
(872) Letter from Dr Peter Flanagan to Dr Gunson 26 September 1991 NHBT0000077_074, Written Statement of Dr Peter Flanagan para 178 WITN6933001
(873) Letter from Belinda Phipps to Dr Gunson 20 December 1991 NHBT0000075_074
(874) Letter from Dr Whitrow to Dr Patrick Zentler-Munro 15 November 1990 PRSE0002715
(875) Memo from Dr Martlew to Dr Gunson 13 May 1991 NHBT0000015_065, Dr Vanessa Martlew Transcript 20 January 2002 pp85-86 INQY1000174
(876) Memo from Dr Brian McClelland to Dr Perry 20 November 1984 PRSE0000828. Dr Brian McClelland explained that this was because the six patients who had developed antibodies had also been exposed to other batches (he thought a total of nine batches between them), and the thinking at the time was that if they recalled one batch then logically they would have to recall all of them, which would have left a huge gap in the supply available for patients. Dr Brian McClelland Transcript 28 January 2022 pp46-47 INQY1000178
(877) Memo from Dr Brian McClelland to Dr Perry 20 November 1984 PRSE0000828
(878) Dr Brian McClelland Transcript 28 January 2022 p48 INQY1000178
(879) Letter from Dr Brian McClelland to Dr Cash 15 November 1984 pp1-2 LOTH0000005_052
(880) Dr Brian McClelland explained that it would have involved testing about 3,000 donations (although his letter at the time suggested 4,000) and that neither Dr Tedder nor Dr Philip Mortimer (who had the only laboratories with testing facilities) could undertake this. He candidly stated: “In retrospect, I probably should have attempted to find somewhere in the United States that would have tested them, but I didn’t. It would have been problematical. I suspect I would not have succeeded but I regret not at least having made that attempt.” Dr Brian McClelland Transcript 28 January 2022 p51 INQY1000178, Letter from Dr Brian McClelland to Dr Tedder 28 November 1984 PRSE0000224
(881) See: Letter from Dr Maycock to The British Medical Journal 21 October 1947 DHSC0100009_066
(882) “Maintenance of records: Subsidiary but important means of control are afforded by the maintenance of accurate records of origin, distribution, and administration of blood and blood-products. Such records should include: (1) Record of the names, etc., of donors contributing to each product; (2) Recording of batch numbers of products issued to hospitals and systematic distribution of products to hospitals”. Both were the responsibility of the blood transfusion service centre to maintain. World Health Organization Expert Committee on Hepatitis Report March 1953 p20 RLIT0000215
(883) “A record of every transfusion should be made in the patient’s case notes in addition to the details recorded in the transfusion laboratory. It is not always appreciated that the main reason for accurate recording is the protection of the patient … THE PATIENT’S RECORDS must show: (i) Serial numbers of containers of blood or blood products.” Committee of Regional Transfusion Directors of the Department of Health and Social Security and Welsh Office Notes on Transfusion 1973 p15 HCDO0000861
(884) Blood Transfusion: Record-Keeping and Stock Control Arrangements March 1984 CBLA0001819
(885) “Fiefdoms” was the description Dr Diana Walford used in evidence. Dr Diana Walford Transcript 20 July 2021 p3 INQY1000137
(886) For example, the 101 system was used by quite a few of the RTCs. This was a system by which each donor had a 101 card that captured certain key information. Dr Hewitt described the system as follows: “One side of the card shows his name, address, date of birth, telephone number ... blood group ... any particular antibodies. It does not give all of the information about antibodies which the lab might use. On the reverse side of the card there is a record of the donations which that donor has given. It gives the date of donation, the unique donation, number for each donation and a record of his haemoglobin … If it was a donor who had attended at a workplace session there might well be the employer name included. On the reverse side there was also a column for recording the volume of blood collected. I think. And then there was a column for comments.” Dr Patricia Hewitt Transcript 9 December 2021 pp31-35, pp123-125 INQY1000170
(887) Most RTCs took the donor records of those donors on the panel to the donor sessions. Of course, sometimes a donor might come to a session unexpectedly, and their donor record would not be there. They would be issued with a temporary card.
(888) For example, the Trent RTC kept a separate database of HIV donors and hepatitis donors. They also provided this information to the Centre for Disease Surveillance and Control. Dr William Wagstaff Transcript 25 January 2022 p114 INQY1000175. At the North London Blood Transfusion Centre there was a separate record for donors who were positive. Initiation and Working of a Report of Hepatitis/Jaundice After Transfusion 6 June 1990 p4 NHBT0005376_002. Dr Patricia Hewitt Transcript 9 December 2021 p125 INQY1000170. The records of HIV positive donors at the Aberdeen RTC were kept in a locked drawer in Professor Urbaniak’s desk. Written Statement of Professor Stanislaw Urbaniak para 149 WITN6960001
(889) Blood Transfusion: Record-Keeping and Stock Control Arrangements March 1984 p2 CBLA0001819
(890) Professor Dame Marcela Contreras Transcript 2 December 2021 pp117-118 INQY1000165, Letter from Dr Contreras to Dr F Seymour 3 May 1988 NHBT0115386
(891) For example the East Anglia RTC became computerised sometime before June 1990 because by the time of the Medicines Inspectorate report of June 1990, it was noted that the Centre was computerised. Medicines Inspectorate Inspector Summary of East Anglia Regional Blood Transfusion Centre 3 October 1990 p4 NHBT0006237. The Centre opted to use the TRACE system that had been established in Cardiff. It was a local system (ie not linked to other RTCs) but Leeds, Cardiff and Southampton used the same system. The TRACE system had two kinds of records: there was a section that had all the donor information, including their virus test results, and then there was a manufacturing part, which dealt with all the components and which hospitals they had gone to. For reasons of confidentiality, the two sections of the computer were kept as separate as possible. Dr Lorna Williamson Transcript 8 December 2021 p54 INQY1000169
(892) As from March 1998 it became possible to search across the zones. Written Statement of Dr Gail Miflin paras 156-164 WITN0672006
(893) Written Statement of Dr Gail Miflin para 146 WITN0672006
(894) Dr Jack Gillon Transcript 19 January 2022 pp73-74 INQY1000173, Written Statement of Dr Marc Turner para 72 WITN3530007
(895) Written Statement of Dr Marc Turner paras 63-65 WITN3530007
(896) Whilst there is no evidence that this was a recurring problem, there are instances in the papers of individuals trying to do just this. See for example: Letter from Dr Tovey to Dr Contreras 12 November 1987 NHBT0086883. An HIV positive donor had donated at several centres under different names, which was only discovered because Dr Tovey put the donor’s name on a form to the Public Health Laboratory Service. See also: Written Statement of Professor Dame Marcela Contreras paras 203-204 WITN5711001. See also an article by Drs Contreras, John Barbara, and Moya Briggs about a donor who was asked to refrain from blood donation until further notice as one of his donations of whole blood had caused jaundice in the recipient and his records were withdrawn from the routine donor file; despite these recommendations, he returned as a new donor seven months later and his donation was one of four units given as whole blood to a patient. Barbara et al A Donor implicated in Two Cases of Post-Transfusion Non-A Non-B Hepatitis Vox Sanguinis 1983 NHBT0000030_007
(897) Written Statement of Dr Jean Harrison para 340 WITN7046001
(898) Written Statement of Dr Jean Harrison para 343 WITN7046001
(899) Dr William Wagstaff Transcript 25 January 2022 p108 INQY1000175
(900) Professor John Barbara Transcript 26 January 2022 pp10-11 INQY1000176
(901) Dr Brian McClelland Transcript 28 January 2022 pp167-168 INQY1000178
(902) Dr Morris McClelland Transcript 1 February 2022 pp90-91 INQY1000179
(903) Department of Health Guidelines for the Blood Transfusion Services in the United Kingdom 1989 para 2.62 NHBT0000027_030
(904) Records Storage Report for the National Blood Transfusion Service in England and Wales April 1992 p7 NHBT0071590_001
(905) Minutes of Regional Transfusion Directors meeting 28 November 1973 p7 NHBT0016498
(906) Minutes of Regional Transfusion Directors meeting 28 November 1973 pp6-8 NHBT0016498
(907) In fact the evidence heard by the Inquiry was that it was actually very rare for RTDs to receive such reports.
(908) See also the oral evidence of: Professor Sir Michael Rawlins Transcript 7 June 2022 pp60-68 INQY1000211
(909) An example of such a report is: Letter from Dr Keith L Rogers to Dr Maycock 4 April 1978 HCDO0000255_053
(910) Professor Dame Marcela Contreras Transcript 2 December 2021 p131 INQY1000165, Professor John Barbara Transcript 26 January 2022 p99 INQY1000176
(911) For example the Glasgow and West of Scotland Blood Transfusion Service: Letter from Dr Robert Crawford to Dr Barbara 26 February 1988 NHBT0077898_001, Letter from A Barr to Dr Barbara 30 October 1990 NHBT0080202_001, Letter from Dr Robert Crawford to Dr Barbara NHBT0078118_001
(912) Minutes from Expert Advisory Group on AIDS meeting 29 January 1985 pp2-3 PRSE0002734
(913) Letter from Dr Tovey to Violet Rawlinson 22 October 1986 NHBT0009599, Letter from Dr Flanagan to Violet Rawlinson 9 February 1990 NHBT0019526_001
(914) Minutes of Scottish National Blood Transfusion Service Directors meeting 20 June 1985 p6 PRSE0001423
(915) Minutes of Scottish National Blood Transfusion Service Co-ordinating Group meeting 19 November 1985 p3 SBTS0000243_049
(916) A summary of present practices with respect of recognition and investigation of Transfusion Associated Hepatitis (TAH) in Northern Ireland 24 November 1983 WITN0892004
(917) Written Statement of Dr Chitra Bharucha paras 66-67 WITN6967001
(918) This report came on 16 July 1982 in the Morbidity and Mortality Weekly Report. Epidemiologic Notes and Reports Pneumocystis Carinii Pneumonia among Persons with Hemophilia A Morbidity and Mortality Weekly Report No31 16 July 1982 PRSE0000523
(919) National Institute for Biological Standards and Control.
(920) A minute from Stanley Godfrey in the Policy Division to Dr John Holgate (head of biological products, Medicines Division), copied to Dr Petronella Clarke in the Scientific Services, Equipment and Building Division (Med SEB) who was standing in for Dr Walford during her maternity leave. Memo from Stanley Godfrey to Dr Holgate 16 July 1982 DHSC0002219_009. Dr Holgate responded that he was “aware of the potential adverse publicity concerning the safety of Factor VIII in the USA (and certain other blood products, in my opinion) where the original donation was obtained from the homosexual community.” Memo from Dr Holgate to Stanley Godfrey 20 July 1982 WITN4461115
(921) A few individual health professionals had become aware of the risk of blood-borne infection leading to AIDS before this, such as those who attended the Second International Symposium on Infections in the Immunocompromised Host in Stirling in June 1982, at which a paper referred to “an alarming epidemic of … AIDS … in certain cities in the United States”, that half the patients had died, and that “Blood or bodily secretions would appear to be potential vehicles of infection”. Acquired Immunodeficiency Syndrome: Infection and Neoplasia in Homosexual Men and Intravenous Drug Addicts p105, pp111-112 1983 PRSE0002220. Dr (later Professor) Ian Hann thought, as he later told the Penrose Inquiry, that this was a bombshell, and thought it might be relevant to patients with haemophilia. Written Statement of Professor Ian Hann to the Penrose Inquiry p2 PRSE0003578, Professor Ian Hann Transcript 8 December 2020 pp64-65 INQY1000082.
Dr Mayne remembered Dr John Craske making the connection in an informal lunchtime conversation with Professor Bloom and Dr Peter Kernoff and referring to a paper which may have been an article published in The Lancet in December 1981 that suggested the possibility of an infective agent. Written Statement of Dr Elizabeth Mayne p25 WITN0736009, Immunocompromised Homosexuals The Lancet 12 December 1981 p2 BPLL0002571_098. The CDC convened the first inter-agency meeting in the US to discuss AIDS and its cause in March 1982, but there is no evidence that this or the discussion at it became known at the time to the DHSS or Blood Services. The Krever Report 1997 pp749-750 KREV0000001. Dr Bruce Evatt at the CDC said that his division started to “vigorously pursue the possibility that the new syndrome was blood borne” in the spring of 1982 and that “June and July [1982] became pivotal months in CDC thinking about AIDS.” Evatt The Tragic History or Aids in the Hemophilia Population 1982-1984 2007 p4 CVHB0000042
(922) Agenda and Minutes of Regional Transfusion Directors meeting 20 September 1982 CBLA0001623
(923) Minutes of UK Working Party on Transfusion-Associated Hepatitis inaugural meeting 27 September 1982 CBLA0001625. Dr Craske had written to Dr Gunson before the meeting to suggest that the Working Party’s name be changed to UK Working Party on Transfusion Associated Diseases, so as to allow “discussions of problems which might arise from time to time such as cytomegalovirus infections transmitted by transfusion of the Acquired Immune Deficiency Syndrome (AIDS), the epidemiology of which might have implications for blood transfusion practice.” Letter from Dr Craske to Dr Gunson 17 September 1982 BPLL0001378. However, the Working Party retained the link to hepatitis in its name, and its terms of reference were confined to hepatitis. Minutes of Regional Transfusion Directors Committee Working Party on Transfusion-Associated Hepatitis meeting 27 September 1982 CBLA0001703. This may explain why the Working Party gave little substantive consideration to AIDS at this time. There was, however, no equivalent RTD or NBTS working party responsible for looking at AIDS. There was thus a gap in the organisational structures of the blood service in the UK at this critical time.
(924) Minutes of Regional Transfusion Directors meeting 14 January 1983 CBLA0001663
(925) Minutes of Advisory Committee on the National Blood Transfusion Service meeting 10 January 1983 CBLA0001659. This was a meeting chaired by Dr Edmund Harris, the Deputy Chief Medical Officer, but attended by three RTDs (Dr Gunson, Dr Darnborough and Dr Wagstaff) as well as a number of others with an interest in the blood service.
(926) Minutes of UK Working Party of Transfusion-Associated Hepatitis meeting 18 January 1983 p3 NHBT0000023_002
(927) Minutes of UK Working Party of Transfusion-Associated Hepatitis meeting 20 April 1983 pp3-4 NHBT0000023_003
(928) Dr Brian McClelland thought the uptake of cryoprecipitate would rise as much as fourfold in Edinburgh.
(929) Minutes of Central Blood Laboratories Authority meeting 27 April 1983 p3 BPLL0003987_002. Dr Gunson’s statement, as reported in the minutes, is somewhat confusing. There is no evidence of there having been any substantive or collective consideration of the position on the part of RTDs by this stage, and at the next meeting of RTDs it was not recommended that no further measures be taken. It is possible that the minutes are inaccurate. However, what Dr Gunson was minuted as saying is consistent with a report he and Dr Barbara co-authored dated 28 April 1983 regarding the work of the Working Party on Transfusion-Associated Hepatitis, in which he wrote that: “The Working Party has followed carefully the information from the U.S.A. on AIDS and has considered the recommendations with respect to donor screening and use of cryoprecipitates. To date there have been no cases reported following transfusion of blood or blood products. It has been agreed that, until further information is available, the Working Party will not recommend changes to present practices for donor selection or use of blood products.” Minutes of Regional Transfusion Directors Committee Working Party on Transfusion-Associated Hepatitis meeting 27 September 1982 p2 CBLA0001703
(930) Epidemiologic Notes and Reports Pneumocystis Carinii Pneumonia among Persons with Hemophilia A Morbidity and Mortality Weekly Report No31 16 July 1982 PRSE0000523
(931) Minutes of Regional Transfusion Directors meeting 18 May 1983 p3 CBLA0001707. It is not clear what caused Dr Gunson’s shift from the position as set out on 27 and 28 April (see footnote 929) – ie no changes required – to the position advanced at the meeting of RTDs on 18 May 1983. As at 5 May 1983 Dr Gunson was reporting to Dr Brian McClelland that the question of producing an information leaflet for donors was “to be held back for a few weeks until it is clear whether the present high level of media attention is to continue.” Note on telephone conversation with Dr Gunson on action being taken on AIDS 5 May 1983 PRSE0001182. It may be that it was Dr Gunson’s attendance as rapporteur at the proceedings of the Council of Europe’s Committee of Experts on Blood Transfusion and Immunohaematology in May 1983 which led to specific options finally being put forward to RTDs on 18 May. Dr Gunson had written to Dr Walford on 16 May regarding the Council of Europe meeting to let her know that the proposed resolution would include the provision of information to all donors so that those at risk would abstain from donation. In this letter he commented: “You can see that what they are leading to is the greater use of cryoprecipitate, and we saw two years ago that this tends to be the standard product in many European countries. Although I put forward the UK view of this product the consensus was against us ... Fortunately everyone here [at the meeting] was in agreement that it was vital to present a balanced view of this problem and to avoid emotive over-reaction (my phrase which will appear in the report of the meeting!).” Letter from Dr Gunson to Dr Walford 16 May 1983 DHSC0000716
(932) Dr Brian McClelland had taken the initiative to prepare his own leaflet for use by the Edinburgh and South East Scotland RTC; see below under the sub-heading Scotland.
(933) Dr Wagstaff, the Trent RTD, thought there was unanimity, or at least consensus, with regards to the rejection of option (2). In respect of option (1), this was more contentious, “because it was felt by many people, perhaps up to 50 per cent of the Regional Transfusion Directors, that an approach made by really direct questioning about sexual proclivities at a donor session would be disruptive to the session itself and would certainly be a disincentive to donors to come again.” Dr William Wagstaff Transcript 25 January 2022 pp59-60 INQY1000175
(934) Dr Davies was the North London RTD at the time.
(935) Minutes of Regional Transfusion Directors meeting 18 May 1983 p4 CBLA0001707
(936) Letter from Dr Wagstaff to National Blood Transfusion Service colleagues 7 June 1983 NHBT0096480_013. Dr Wagstaff had been contacted by Dr Walford, with two issues being raised. The first related to the questioning of donors at sessions: it was suggested that the DHSS would prefer that pertinent questions be inserted in the list of diseases to be considered at sessions by donors. Dr Wagstaff wrote to his colleagues: “You will remember that this particular subject was discussed at length in Cambridge and the decision of the meeting as a whole was that it was not really desirable to introduce questions of non-specific symptoms such as weight loss, night sweats, and enlarged glands. My recollection is that we thought that reference to the Medical Officer of every donor who reacted positively to this type of written question would be extremely disruptive at a donor session. However, I have been asked to ask you to review this decision, even though you may think that it should stand.” The second issue related to the method of distribution of the leaflet: the DHSS wanted to know “its degree of availability. For instance, do we intend to simply have it prominently displayed at the Clerking Desk, so that any donor who displays an interest may take one, or do we intend to actively hand one to each donor as he or she signs in. My impression is that the Department would prefer the latter option.” Dr Wagstaff asked for RTDs’ reaction to these two points so that he could communicate the consensus view to Dr Walford.
(937) Letter from Dr Wagstaff to National Blood Transfusion Service colleagues 6 July 1983 NHBT0020668. What was set out in Dr Wagstaff’s letter of 6 July 1983 no doubt reflected the responses he had received to his letter of 7 June. Dr Fraser’s response (from Bristol) noted that there was nowhere where a private discussion could be held between the medical officer and the donor and that they did not support the idea of handing the AIDS leaflet to all donors (although it should be on prominent display), and suggested displaying a poster at the entrance of the session. Letter from Dr Fraser to Dr Wagstaff 15 June 1983 NHBT0039762_049. Dr Tovey (Leeds) was strongly in favour of keeping the matter low key, but saw no reason why the clerk should not hand the pamphlet to each donor to read. He commented: “This is just the DHSS trying to get themselves off the hook … I suggest you ask the DHSS whether they wish us to reject all homosexuals? Lets put the ball in their court.” Letter from Dr Tovey to Dr Wagstaff 13 June 1983 NHBT0021382. Dr Anne Collins (Newcastle) reported the support of her colleagues for each donor being positively given a copy. Letter from Dr Collins to Dr Wagstaff 20 June 1983 NHBT0101333_008. Dr Entwistle (Oxford) proposed that the leaflet be made available along with other NBTS literature but should not be handed to each donor, and thought that routine questioning of donors “in the open forum of a clerking desk” to seek information on their personal habits would be counterproductive. Letter from Dr Entwistle to Dr Wagstaff 14 June 1983 p1 NHBT0020746
(938) Department of Health and Social Security AIDS and how it concerns blood donors National Blood Transfusion Service 1983 BPLL0007247
(939) A meeting of the Western Division of NBTS consultants on 13 September 1983 reported that Birmingham “had produced their own leaflets and have been distributing them for three months.” Minutes of Western Division of National Blood Transfusion Service Consultants meeting 13 September 1983 NHBT0092855_002. The leaflet, dated May 1983, is at: AIDS and Blood Transfusion West Midlands Regional Transfusion Service p2 NHBT0046177. Dr Ala, the RTD, also spoke to local press and radio. Sunday Mercury AIDS scare gays told: Don’t give blood 31 July 1983 DHSC0002231_010, Letter from Dr Ala to Dr Gunson 17 October 1989 NHBT0020751
(940) Written Statement of Dr Brian McClelland para 299 WITN6666001
(941) Minutes of Regional Transfusion Directors meeting 22 September 1983 p1 CBLA0001742
(942) Minutes of UK Working Party on Transfusion-Associated Hepatitis meeting 27 September 1983 p3 PRSE0001299. Dr Barbara, Dr Brian McClelland and Dr Ruthven Mitchell participated from the RTDs. Dr Brian McClelland also pointed out that the distinction between promiscuous and non-promiscuous homosexuals was not conclusive since it did not cover the promiscuity of the partner, and it was suggested that the AIDS pamphlet be made available to special clinics since some donors would be patients at such clinics. Minutes of UK Working Party on Transfusion-Associated Hepatitis 27 September 1983 p4 PRSE0001299. The same preference for uniformity of approach was expressed at the first meeting of the Central Blood Laboratories Authority’s Working Group on AIDS in mid October 1983, at which the view was expressed in relation to the content of the leaflet that the important message not to give blood if in a high-risk group should be highlighted in some way. Dr Richard Lane expressed the view that marketing/advertising expertise might assist on how to get information to the public and the meeting agreed that special clinics should be included in the distribution, health education councils should be approached, gay societies should be contacted, and comments on the leaflets from donors might be invited. These matters were to be raised with the DHSS on 17 October at the next meeting of the Advisory Committee of the NBTS. Minutes of Central Blood Laboratories Authority Working Group on AIDS meeting 14 October 1983 pp1-2 CBLA0001754. However, whilst the AIDS leaflet was mentioned at the Advisory Committee’s meeting, the minutes record no discussion about methods of distribution or the other matters raised by the Working Group on AIDS. Minutes of Advisory Committee on the National Blood Transfusion Service meeting 17 October 1983 p4 CBLA0001763
(943) Minutes of Regional Transfusion Directors meeting 25 January 1984 p2 NHBT0018332. The leaflets do not appear to have provoked much response from donors: in mid September 1983 the centres within both the Western Division and the Eastern Division of the NBTS were reporting that there had been little or no comment from donors in relation to the leaflets. Dr Rogers, of the Eastern Division, expressed the view that a more active approach should be made (rather than simply distributing the pamphlet). Minutes of Eastern Division of Blood Transfusion Service Consultants’ meeting 14 September 1983 NHBT0092845_002
(944) Minutes of National Blood Transfusion Service Advisory Committee meeting 10 April 1984 pp2-3 CBLA0001835
(945) Dr Smithies reported that a revised and updated leaflet was in preparation. Minutes of Regional Transfusion Directors meeting 11 April 1984 p3 CBLA0001836
(946) Minutes of Regional Transfusion Directors meeting 11 July 1984 p3 DHSC0002245_002
(947) Minutes of Regional Transfusion Directors meeting 10 October 1984 CBLA0001905
(948) Minutes of National Blood Transfusion Service Advisory Committee meeting 8 November 1984 p3 PRSE0004783
(949) Agenda for National Blood Transfusion Service Advisory Committee Working Group on AIDS meeting November 1984 pp4-5 CBLA0011985
(950) Memo from Dr Abrams to Dr Harris following Working Group on AIDS meeting 27 November 1984 p1 DHSC0002251_011. The 27 November meeting of the Working Group on AIDS was felt by the RTDs in attendance to be “unproductive”, “there being as yet no new leaflet, no finance and no positive move towards full donor screening.” Minutes of Regional Transfusion Directors meeting 23 January 1985 p1 PRSE0002062
(951) Report on meeting of Advisory Group on AIDS 27 November 1984 p1 PRSE0004191
(952) Minutes of Western Division of National Blood Transfusion Service Consultants meeting 7 December 1984 p2 NHBT0113565
(953) Minutes of Regional Transfusion Directors meeting 23 January 1985 p4 PRSE0002062. Dr Gunson stressed the efforts made by Dr Smithies and Mr Williams: “the regrettable delays are in no way attributable to them.”
(954) National Blood Transfusion Service AIDS: Important New Advice for Blood Donors Department of Health and Social Security January 1985 NHBT0096480_022. A circular was issued to regional health authorities setting out the revised distribution arrangements that were required: the leaflet now had to be brought to the attention of each donor on an individual basis. Memo from Health Services Division to regional health authorities January 1985 DHSC0002159
(955) Minutes from Expert Advisory Group on AIDS meeting 29 January 1985 p5 PRSE0002734. EAGA included three RTDs – Dr Contreras, Dr Gunson and Dr Brian McClelland – amongst its members.
(956) Minutes of Regional Transfusion Directors meeting 17 April 1985 PRSE0002906, Minutes of Regional Transfusion Directors meeting 10 July 1985 CBLA0002212
(957) National Blood Transfusion Service AIDS: Important Information for Blood Donors Department of Health and Social Services September 1985 CBLA0002255
(958) Minutes of Eastern Division of Blood Transfusion Service Consultants’ meeting 3 October 1985 pp1-2 NHBT0092834
(959) Minutes of Regional Transfusion Directors meeting 9 October 1985 DHSC0002365_002
(960) Minutes of Scottish National Blood Transfusion Service Directors meeting 14 September 1982 PRSE0000451, Minutes of Scottish National Blood Transfusion Service Directors meeting 14 December 1982 PRSE0003058
(961) Minutes of Scottish National Blood Transfusion Service and Haemophilia Directors meeting 21 January 1983 p7 PRSE0001736
(962) Minutes of Scottish National Blood Transfusion Service Directors meeting 29 March 1983 p5 PRSE0000193
(963) Minutes of Scottish National Blood Transfusion Service Co-ordinating Group meeting 24 May 1983 p5 PRSE0003620
(964) Guidance on AIDS and Blood Transfusion May 1983 PRSE0000984. This was the first draft of the leaflet, put together by Dr Brian McClelland and his colleague Dr Anne Smith. Dr Brian McClelland’s recollection was that he and his colleagues in the South East Scotland Transfusion Service decided they needed to do something, worked on drafts, and that he then telephoned Dr Bell of SHHD to inform him that the leaflet was going to be used, rather than request his permission or agreement. Dr Brian McClelland Transcript 27 January 2022 pp156-157 INQY1000177. In addition to what he described as the “fairly obvious” factor that it was important to take whatever action they could identify to reduce risk to transfusion recipients, he recalled another factor being the suggestion in local media that Edinburgh could become the “AIDS capital of the North”. Dr Brian McClelland Transcript 27 January 2022 pp160-161 INQY1000091
(965) Minutes of Scottish National Blood Transfusion Service Co-ordinating Group meeting 24 May 1983 pp5-6 PRSE0003620
(966) The version of the leaflet that was used in the South East Transfusion Service region: Guidance on AIDS and Blood Transfusion June 1983 PRSE0004850. Differences in wording between the initial Scottish leaflets and the national DHSS leaflet are considered in the chapter on Role of Government: Response to Risk.
(967) Minutes of Scottish National Blood Transfusion Service Directors meeting 14 June 1983 pp2-3 MACK0001960_001. Dr Brian McClelland was fairly sure that the media were not used at this stage. Dr Brian McClelland Transcript 28 January 2022 p15 INQY1000178
(968) Dr Brian McClelland Transcript 28 January 2022 p12 INQY1000178. Not all directors introduced the leaflet at that stage. The Glasgow and West of Scotland BTS added to its questionnaire a note asking if donors had heard of AIDS and stating that if they had any doubts about giving a donation they should consult the session doctor or their GP or write to the regional director. Glasgow and West of Scotland Transfusion Service donor questionnaire 1983 PRSE0004816. The document bears a handwritten date “16/6/83”. Dr Gabra, a consultant with Glasgow and West of Scotland BTS, thought that Glasgow later used the leaflet drawn up by Dr Brian McClelland. Dr Gamal Gabra Transcript 3 February 2022 pp63-64 INQY1000180. The Aberdeen and North East BTS decided it was premature to issue the leaflet to donors. Letter from Dr Urbaniak to Dr Brian McClelland 10 May 1983 WITN6960012, Written Statement of Professor Stanislaw Urbaniak paras 180-188 WITN6960001
(969) Minutes of Scottish National Blood Transfusion Service Co-ordinating Group meeting 30 August 1983 p4 SBTS0000696_067. The national leaflet replaced the version which had been used by Dr Brian McClelland in the South East Scotland Transfusion Service. Its publication on 1 September 1983 was accompanied by a Scottish Information Office press release. Scottish Information Office Press Release Information Leaflet on AIDS Issued 1 September 1983 PRSE0002778
(970) Minutes of Scottish National Blood Transfusion Service Directors meeting 13 September 1983 pp2-3 PRSE0002617
(971) It was reported that there had been no reaction to the leaflets, which is not surprising if they were merely on display with other leaflets.
(972) The minutes do not record if they were merely displayed or actually provided to donors, but say that there had been “Very little reaction.” Minutes of Scottish National Blood Transfusion Service Directors meeting 13 September 1983 p2 PRSE0002617
(973) The “health notices” or “illness notices” in other Scottish centres had not been amended. It was reported that in England and Wales two questions had been added, namely whether the donor had consulted his doctor recently and whether he had experienced unexplained loss of weight. Minutes of Scottish National Blood Transfusion Service Directors meeting 13 September 1983 p3 PRSE0002617
(974) Dr Brian McClelland Transcript 28 January 2022 pp11-12 INQY1000178
(975) Dr Wagstaff also reported on the position in England and Wales, explaining that there had been pressure to give the leaflet to all donors attending but that the RTDs had objected to this approach, so that a trial was being run with some centres handing the leaflet to every donor, others making them available at sessions, and others sending them out with the call-up letter. Minutes of Scottish National Blood Transfusion Service Directors meeting 13 September 1983 p3 PRSE0002617
(976) Minutes of Scottish National Blood Transfusion Service Directors meeting 8 December 1983 p2 MACK0001529. Dr Brian McClelland had recently returned from the US, where he had attended the WHO meeting on AIDS, and advised that the leaflet required modification and more uniform circulation to donors. Draft of Acquired Immune Deficiency Syndrome and Transfusion 5 December 1983 p9 WITN6666011
(977) As an interim measure Dr Brian McClelland added a specific reference to AIDS in the donor call-up letters sent out from the Edinburgh and South East BTS, drawing attention to the leaflet, and added specific questions and references to AIDS and the leaflet to the questionnaire completed by donors. Letter from Dr Brian McClelland to Dr Cash 23 December 1983 PRSE0003679. Dr Brian McClelland did not know whether other regions within Scotland took similar steps. Dr Brian McClelland Transcript 28 January 2022 p24 INQY1000178
(978) Minutes of Scottish National Blood Transfusion Service and Haemophila Directors meeting 2 February 1984 p3 PRSE0001556. The SNBTS directors meeting on 7 February 1984 recorded that Dr Brian McClelland had produced a revised leaflet which would be discussed at a Co-ordinating Group meeting. Minutes of the Scottish National Blood Transfusion Service Co-ordinating Group meeting 7 February 1984 p4 SBTS0000615_042
(979) Draft of Leaflet on AIDS: Designed to be Sent to Blood Donors with Routine Call Up Letters During 1984 PRSE0001302, Minutes of Scottish National Blood Transfusion Service Directors meeting 13 March 1984 p2 PRSE0003405
(980) Minutes of Scottish National Blood Transfusion Service Directors meeting p1 PRSE0002709, Important Message to Blood Donors Scottish National Blood Transfusion Service 1984 PRSE0000286
(981) Minutes of Scottish National Blood Transfusion Service Co-ordinating Group meeting 20 November 1984 p2 SBTS0002210. On 29 November 1984 Dr Brian McClelland wrote to Dr Cash confirming that the Edinburgh and South East Scotland Region had now introduced modified forms which asked the donor to sign a specific declaration that they had read the AIDS leaflet and were not in a risk group. Letter from Dr Brian McClelland to Dr Cash 29 November 1984 SBTS0000242_026. Dr Brian McClelland accepted in his evidence to the Inquiry that this step – asking donors to sign such a declaration – was something that could have been part of the process from the outset in June 1983. Dr Brian McClelland Transcript 28 January 2022 pp38-39 INQY1000178
(982) Minutes of Scottish National Blood Transfusion Service Directors meeting 11 December 1984 p4 PRSE0001767. At the meeting Dr Cash raised again the question of mailing all donors on the panel and directors agreed this was impracticable.
(983) Dr Brian McClelland confirmed at the next SNBTS directors meeting on 27 February that he was now mailing the leaflet to all active donors on the panel.
(984) Minutes of Scottish National Blood Transfusion Service Co-ordinating Group meeting 19 February 1985 p6 PRSE0003378
(985) Minutes of Scottish National Blood Transfusion Service Directors meeting 27 February 1985 p7 PRSE0003628
(986) Minutes of Regional Transfusion Directors meeting 9 July 1986 pp3-4 CBLA0002312
(987) Minutes of Expert Advisory Group on AIDS meeting 26 September 1986 p3 MRCO0000001_048
(988) National Blood Transfusion Service information leaflet AIDS: What you must know before you give blood September 1986 BPLL0007799_002, Minutes of Regional Transfusion Directors meeting 8 October 1986 pp2-3 CBLA0002345. Dr Cash was reported to have expressed concern that the AIDS leaflet was not being taken seriously, supporting this with evidence of his own experience as a donor recently. He also requested cross-border co-operation in the preparation of future literature and asked the chair (Dr Fraser) to approach the DHSS regarding proposals for a study into the effectiveness of the literature in self-excluding donors in high-risk groups. The initiation of this study was reported at the next meeting of RTDs in January 1987. Minutes of Regional Transfusion Directors meeting 21 January 1987 p4 CBLA0002358_001
(989) Minutes of Regional Transfusional Directors meeting 21 January 1987 p3 CBLA0002358_001
(990) Minutes of Eastern Division of Blood Transfusion Service Consultants meeting 13 April 1987 p3 NHBT0072049_007
(991) Minutes of Regional Transfusion Directors meeting 15 April 1987 p3 CBLA0002372
(992) Minutes of Expert Advisory Group on AIDS meeting 19 May 1987 p6 MRCO0000006_004
(993) National Blood Transfusion Service AIDS: Think before you give blood Department of Health and Social Security July 1987 NHBT0007310
(994) See also for England and Wales a table of RTC experiences with the leaflet for the first six months after September 1983: five centres (Newcastle, Sheffield, Southampton, Manchester and Liverpool) had sent out the leaflets with call-up cards, and at Tooting new donors received the leaflet with their certificate book. The remainder made the leaflets available at sessions. Birmingham and Bristol were a little more proactive at sessions: at Birmingham the leaflets were handed to donors, and at Bristol they were offered on “signing in”. Advisory Committee on the National Blood Transfusion Service AIDS Leaflet: First Six Months Experience CBLA0001820. The position in Scotland is described above.
(995) Dr Morris McClelland Transcript 1 February 2022 pp117-118 INQY1000179. Dr Morris McClelland also explained that Northern Ireland was likely to be one of the most low-risk regions, in contrast to places like London or Edinburgh.
(996) Minutes of Scottish National Blood Transfusion Service Directors meeting 13 September 1983 p3 PRSE0002617
(997) Letter from Dr Morris McClelland to Dr Smithies 25 January 1985 DHSC0101652_002. Dr Morris McClelland anticipated that this would change during 1985 with the advent of a computerised donor call-up system and automatic enveloper.
(998) For example, homosexuality had only ceased to be illegal in 1982.
(999) Dr Morris McClelland Transcript 1 February 2022 pp121-124 INQY1000179
(1000) Note of meeting between Welsh Office and Medical Services Health Professional Group 4 May 1983 p3 HSSG0010055_001
(1001) Western Mail Blood virus assurance 3 May 1983 DHSC0001652
(1002) Letter from J Emyln-Jones to Paul Winstanley 23 November 1983 DHSC0002237_014, Dr Morris McClelland Transcript 1 December 2021 p27 INQY1000179
(1003) Note of meeting called by the Chief Medical Officer of the Welsh Office 19 November 1984 p3 HSSG0010054_008
(1004) Minutes of South Glamorgan District Health Authority meeting 4 December 1984 p1 HSSG0010054_004, Dr Tony Napier Transcript 1 December 2021 p37 INQY1000164
(1005) Letter from Dr Napier to Dr Smithies 30 January 1985 DHSC0101658_015. Dr Napier observed in the letter that a “suitably tactful poster would probably be an advantage” but they would like to see an example before committing themselves.
(1006) Advisory Committee on the National Blood Transfusion Service AIDS Leaflet: First Six Months Experience p1 CBLA0001820, Dr William Wagstaff Transcript 25 January 2022 p63, pp67-70 INQY1000175. Dr Wagstaff thought that donors walking in the door could use the pre-existing (non-AIDS) list as an excuse for not remaining at the session. It was important to be able to facilitate self-exclusion at any point without giving the direct impression that it was because of AIDS. Dr William Wagstaff Transcript 25 January 2022 pp75-76 INQY1000175
(1007) Dr Wagstaff was not aware that the North London RTC, fed up with waiting for the second leaflet, had started to overprint the first leaflet, and did not consider taking such steps himself. He did understand the North London RTC to have issued its own supplementary document regarding the transmission of AIDS by high-risk behaviour. Dr William Wagstaff Transcript 25 January 2022 pp72-73 INQY1000175
(1008) Dr Colin Entwistle Transcript 6 December 2021 pp73-74 INQY1000167
(1009) Dr Colin Entwistle Transcript 6 December 2021 p76 INQY1000167
(1010) Dr Colin Entwistle Transcript 6 December 2021 p83 INQY1000167. It is correct that this would not cater for walk-in donors, such that sending the leaflet with the call-up cards should not have been the only method of distribution used by centres, but one risk of only having the leaflet available at sessions was that some high-risk donors might never read the leaflet, which Dr Entwistle accepted was “quite possible”. Dr Colin Entwistle Transcript 6 December 2021 pp77 INQY1000167
(1011) Letter from Dr Entwistle to S Green 28 March 1984 DHSC0002241_002, Dr Colin Entwistle Transcript 6 December 2021 p84 INQY1000167
(1012) Letter from Dr Davies to all medical officers 23 May 1973 NHBT0109173. Dr Contreras, who at the time was a consultant at the RTC but not director, did not agree with this; her view was that there was nothing wrong in asking donors about their sexual practices. Professor Dame Marcela Contreras Transcript 2 December 2021 pp168-171 INQY1000165
(1013) Professor Dame Marcela Contreras Transcript 2 December 2021 pp176-178 INQY1000165
(1014) Professor Dame Marcela Contreras Transcript 2 December 2021 pp179-181 INQY1000165
(1015) Memo from Dr Contreras to all medical officers 16 October 1984 NHBT0017776, Professor Dame Marcela Contreras Transcript 2 December 2021 pp181-183 INQY1000165
(1016) Professor Dame Marcela Contreras Transcript 3 December 2021 pp2-4 INQY1000166
(1017) Professor Dame Marcela Contreras Transcript 3 December 2021 pp9-11 INQY1000166, Dr Patricia Hewitt Transcript 9 December 2021 p69 INQY1000170, Guidance to blood donors by National Blood Transfusion Service PRSE0001398
(1018) Which became, and is better known as, the Terrence Higgins Trust.
(1019) Written Statement of Dr Brian McClelland para 279, para 321 WITN6666001
(1020) Dr Brian McClelland Transcript 27 January 2022 p124 INQY1000177
(1021) Western Mail Blood virus assurance 3 May 1983 DHSC0001652
(1022) Draft of Acquired Immune Deficiency Syndrome and Transfusion p6 WITN6666011. A point made by Dr Brian McClelland following a visit to New York and participation in the WHO meeting on AIDS in November 1983.
(1023) Draft of Acquired Immune Deficiency Syndrome and Transfusion p6 WITN6666011
(1024) See chapter on Role of Government: Response to Risk.
(1025) A poster was suggested by Dr Fraser (Bristol) in a letter to Dr Wagstaff in June 1983 and by Dr Rogers (South London) to Dr Walford the same month. Letter from Dr Fraser to Dr Wagstaff 15 June 1983 NHBT0039762_049, Letter from Dr Rogers to Dr Walford 10 June 1983 NHBT0039762_046
(1026) Some individual centres used posters. A poster was being used at South London by January 1985: Letter from Dr Rogers to Dr Smithies 22 January 1985 DHSC0002257_057. A “large notice” stating the at-risk categories was introduced in Bristol in 1984 to deter such donors from entering into the session. Draft submission by Dr Ian Fraser p9 NHBT0019638. By January 1985, the Wessex RTC was displaying a poster at sessions and Dr Donald Smith wrote to Dr Smithies, expressing the view that a national poster would be very useful. Letter from Dr Donald Smith to Dr Smithies 24 January 1985 DHSC0101658_014. Yorkshire RTC used a poster possibly from late 1983, which invited donors to read the leaflet. Memo from E Frank to Dr Robinson and Dr Townley 3 January 1989 NHBT0021384
(1027) Some centres sent out call-ups by postcard which made sending the leaflets more difficult. However, that should have been capable of being overcome (eg by purchase of what Dr Rogers called a “stuffing machine” which allowed the cards to be sent in envelopes with a copy of the leaflet). Letter from Dr Rogers to Dr Smithies 22 January 1985 p1 DHSC0002257_057
(1028) Letter from Dr Rogers to Dr Smithies 22 January 1985 DHSC0002257_057
(1029) Memo from Dr Harrison to Mr Smith 1 February 1985 NHBT0039762_088. Donors would be asked to confirm whether they were in at-risk groups rather than being explicitly questioned about sexual practices. Written Statement of Dr Stephen Dealler paras 429-431 WITN7065001
(1030) Letter from Dr Darnborough to Dr Smithies 5 February 1985 NHBT0021395, Memo from the Regional Donor Organiser to colleagues 1 February 1985 NHBT0021396. The new routine involved: sending the leaflet to all donors called by card to sessions; handing the leaflet to new donors, or donors who had not been invited by card, at the time of registration; asking all donors directly if they had read it.
(1031) Dr Patricia Hewitt Transcript 9 December 2021 pp73-74 INQY1000170
(1032) Summary Report on Workgroup to Identify Opportunities for Prevention of Acquired Immune Deficiency Syndrome 4 January 1983 p3, p5 MULL0001034_004
(1033) Memo from Dr Francis to Dr Koplan 6 January 1983 pp1-2 MULL0001202_045
(1034) Successor to a number of previous Victorian statutes relating to the adulteration of food, and to the sale of drugs in a “pure and genuine” condition.
(1035) The most recent statutory scheme concerned with biological standards before that was the Therapeutic Substances Act 1956, which by section 3 provided that substances to which the Act applied must meet appropriate standards of strength, quality and purity.
(1036) The control of medicines in the United Kingdom July 1977 p10 MHRA0004773
(1037) Professor Sir Michael Rawlins Transcript 7 June 2022 pp18-22 INQY1000211
(1038) Dr Diana Walford Transcript 19 July 2021 pp24-5 INQY1000136
(1039) “worked in silos”: Professor Sir Michael Rawlins Transcript 7 June 2022 p9 INQY1000211
(1040) The labels “Armour”, “Cutter”, “Travenol”, “Baxter”, “Hyland”, “Immuno”, “Abbott”, and “Alpha”” are used to describe the companies who produced the main factor concentrates that were imported into the UK and used in the treatment of patients within the UK. This is done for readability. On occasion reference is made to other companies that formed part of the wider corporate entity to which the companies referred to above belonged – for example where it is necessary for context to distinguish between the manufacturing company in the US or Austria and either the UK company that held the relevant product licence or its ultimate owner. See the preface to the chapter Pharmaceutical Companies.
(1041) Professor Sir Michael Rawlins Transcript 7 June 2022 p21 INQY1000211
(1042) A member of CSM from 1980 and CSM chair 1993-1998.
(1043) Professor Sir Michael Rawlins Transcript 7 June 2022 p22 INQY1000211
(1044) Written Statement of Sir Michael Rawlins para 7.17 WITN6406001
(1045) Freedom of Information and the Committee on Safety of Medicines June 1998 WITN6406007
(1046) Professor Rawlins did not know why the CSM had not pressed for greater transparency at an earlier stage. Professor Sir Michael Rawlins Transcript 7 June 2022 p34 INQY1000211. It appears that at the time of the CSM decisions with which this chapter is concerned, the view was taken that confidentiality was required by reason of section 118 of the Medicines Act 1968: see, for example, the CSM’s June 1998 report on Freedom of Information: “The CSM … regards the present constraints preventing disclosure, placed upon it by both statute as well as by custom and practice, as being against the broadest public interest” and “The Committee’s legal advisers have always indicated that the provisions of Section 118 of the Medicines Act (1968) inhibit disclosure.” Freedom of Information and the Committee on Safety of Medicines p1, p5 WITN6406007. In 1989 the CSM obtained advice from leading counsel to the effect that “hitherto s.118 has been regarded as a straitjacket. It is not. Use, including disclosure, of information is permissible if it is reasonably necessary to assist the Licensing Authority in its general duty to safeguard public health. If the information is not confidential in the sense that its disclosure would otherwise be restrained by a court, such use can be relatively easily approved. If it is confidential, the Licensing Authority will have to weigh that in the balance and only disclose it if satisfied that the need to do so outweighs the need to preserve confidentiality.” Disclosure of Information Obtained Under the Medicines Act 1969 1 March 1989 pp12-13 MHRA0029245
(1047) In this respect it echoed the provisions of section 3 of the Therapeutic Substances Act 1956.
(1048) Written Statement of Sir Joseph Smith para 2.8 WITN5281001
(1049) Written Statement of Dr Trevor Barrowcliffe paras 3.15-3.23 WITN6408001
(1050) These could include bulk and in-process materials as well as the finished product, since the control of those is essential to the quality and safety of the finished product. Written Statement of Sir Joseph Smith para 2.11 WITN5281001
(1051) Written Statement of Dr Trevor Barrowcliffe para 3.22 WITN6408001
(1052) Written Statement of Dr Trevor Barrowcliffe para 5.14, para 5.23 WITN6408001. The “named patient” exemption is described later in this chapter.
(1053) Under the Biological Standards Act 1975 section 1.
(1054) See, for instance: The control of medicines in the United Kingdom para 21, para 46 MHRA0004773, a leaflet from the Medicines Division which shows that certainly by July 1977 it had done so.
(1055) Written Statement of Dr Duncan Thomas para 2.10 WITN6405001. Representatives of NIBSC would frequently attend meetings of CSM(B).
(1056) Written Statement of Sir Joseph Smith para 2.28 WITN5281001
(1057) CDSC’s first medical consultant epidemiologist for Wales, Professor Stephen Palmer, took up his post in May 1983: Written Statement of Professor Stephen Palmer para 2.1 WITN7654001
(1058) A matter into which the PHLS might be asked to give input; whereas efficacy and quality were matters more for NIBSC.
(1059) These are simplified descriptions of a definition which is to be found in section 19 of the Act. The simplification is for readability.
(1060) Section 19(2).
(1061) Professor Sir Michael Rawlins Transcript 7 June 2022 p40 INQY1000211
(1062) Food and Drug Administration, a US governmental authority.
(1063) Professor Sir Michael Rawlins Transcript 7 June 2022 p41 INQY1000211
(1064) The Krever Report 1997 p530 KREV0000001
(1065) According to his statement, part of his role was “to assess the clinical trial and medical data that the manufacturers sent in with their application. I would describe myself as a medical assessor.” Written Statement of Dr Duncan Thomas para 2.6 WITN6405001. His input was to summarise the application, provide input, and make a recommendation to the CSM(B). Written Statement of Dr Duncan Thomas para 2.9 WITN6405001
(1066) Written Statement of Dr Duncan Thomas para 2.17 WITN6405001
(1067) Institute of Medicine Committee to Study HIV Transmission Through Blood and Blood Products HIV and the Blood Supply: An analysis of crisis decisionmaking 1995 JREE0000019
(1068) Institute of Medicine Committee to Study HIV Transmission Through Blood and Blood Products HIV and the Blood Supply: An analysis of crisis decisionmaking 1995 p180, pp242-245 JREE0000019. Lord Penrose would conclude in his report, in relation to blood products, that “subjecting UK products to a need for approval to the FDA before introducing them for use in Scotland would not have been a rational exercise of judgement by any UK or Scottish government agency”. The Penrose Inquiry Final Report March 2015 para 30.255 PRSE0007002. What preceded this conclusion was a detailed critique of reliance upon an agency such as the FDA in a foreign country. I accept both his reasoning, and his conclusions, on this particular point.
(1069) Institute of Medicine Committee to Study HIV Transmission Through Blood and Blood Products HIV and the Blood Supply: An analysis of crisis decisionmaking 1995 p244 JREE0000019
(1070) World in Action Blood Money Part 1 1 December 1975 MDIA0000113, World in Action Blood Money Part 2 8 December 1975 MDIA0000114
(1071) Later to become Professor Zuckerman.
(1072) Medicines Act 1968 section 31(1)(b).
(1073) This represents an approach based in large part on the idea of “clinical freedom”, and the corresponding doctrine that the State should stand back from regulating matters of professional judgement too closely – though it would not prevent the profession, via the General Medical Council, or the legal system from intervening if occasion arose.
(1074) Although it might be argued that few complaints to the General Medical Council or actions for clinical negligence occurred, the fact that they might do so may well have exercised some restraining influence.
(1075) Medicines Act 1968 section 31(4)(b).
(1076) Six units are recorded as sold to Crown Agents, one unit to Dr Mibachan: Table showing supply for Kryobulin and Bebulin 22 November 1972 p2 SHPL0000071_185. The use of the term “unit” may not in this case be a reference to what became an international standard unit in 1970 when the Expert Committee on Biological Standardisation of WHO formally established an international standard for Factor 8. All preparations for sale claiming to have Factor 8 activity were legally obliged thereafter to be labelled with those international units.
(1077) Serological Products Ltd later became Immuno Ltd, adopting the name from the parent company Immuno AG, of Vienna.
(1078) Hyland Therapeutics was a division of Travenol Laboratories which in turn was part of the Baxter group of companies in the US.
(1079) Written Statement of Dr Duncan Thomas para 2.24 WITN6405001
(1080) Dr Thomas also described the medical screening of the donors as “rudimentary”. Travenol Laboratories Ltd application for Hemofil product licence January 1973 p15 DHSC0105593_006
(1081) Note the use of “very”.
(1082) Travenol Laboratories Ltd application for Hemofil product licence January 1973 p15 DHSC0105593_006
(1083) Travenol Laboratories Ltd application for Hemofil product licence January 1973 p4 DHSC0105593_006
(1084) Director of the North London Blood Transfusion Centre.
(1085) As does not appear to have been revealed previously.
(1086) Dr Cleghorn’s minute of the meeting is at: Minute of National Blood Transfusion Service meeting 25 July 1975 OXUH0001590_001. The participants are listed in: List of National Blood Transfusion Service meeting participants 25 July 1975 OXUH0001590_003. Investigative reporter Michael Gillard’s notes of his conversation with Dr Cleghorn in October 1975 are at: Note on Dr Thomas Cleghorn interview 9 October 1975 MGIL0000053. Michael Gillard’s notes of his conversation with Dr David Dane, virologist, who also attended the meeting, are at: Note on Dr David Dane interview 7 October 1975 MGIL0000050, Note on Dr David Dane interview September/October 1975 MGIL0000051. A letter Michael Gillard received from Baxter in November 1975 about the source of plasma in Hemofil used in the UK is at: Letter from Richard Wilbur of Baxter Laboratories to Michael Gillard 25 November 1975 MGIL0000085
(1087) Travenol Laboratories Ltd application for Hemofil product licence January 1973 p14 DHSC0105593_006
(1088) Neither of these two statements is strictly accurate. An international forum reported in Vox Sanguinis in 1972 clearly assessed that patients with haemophilia could be adequately maintained with the use of cryoprecipitate, a major advantage of which was seen to be a lower risk of hepatitis. A number of the contributors to the forum observed that major surgery, emergency surgery and even prophylaxis could be achieved by using it: Biggs et al Can Hemophilic Patients be Adequately Maintained with Cryoprecipitates? Or is it Desirable or Even Necessary to Manufacture and Administer Highly Concentrated AFH Products? Vox Sanguinis June 1972 BAYP0000022_050. Dr Katharine Dormandy, who contributed to the discussion, was herself an enthusiast for using cryoprecipitate for home therapy, and evidence to the Inquiry establishes that some was used for this purpose in over ten centres, for some time. It is undoubtedly the case that freeze-dried factor concentrates were easier to store domestically and to use therapeutically: but in recognising these advantages of factor concentrates, Dr Thomas was somewhat overstating the case.
(1089) Emphasis added.
(1090) CSM(B) minutes and recommendations 10 January 1973: Minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 10 January 1973 DHSC0105593_002, Appendix A to minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 10 January 1973 DHSC0105593_003
(1091) The CSM advised that “this product should be regarded as new for the purpose of a special directive for the reporting of adverse reactions.” Appendix A to minutes of Committee on Safety of Medicines meeting 25 January 2973 p15 DHSC0003952_054. The licence was duly granted on 19 February 1973. Travenol Laboratories Ltd Hemofil product licence 10 September 1973 SHPL0000276_159
(1092) Summary and report on Kryobulin for product licence application: Serological Products Ltd application for Kryobulin product licence January 1973 p5, p7 MHRA0033322_060
(1093) Serological Products Ltd application for Kryobulin product licence January 1973 p13 MHRA0033322_060
(1094) Minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 10 January 1973 p3 DHSC0105593_002
(1095) Recommendations made by the CSM(B) in: Appendix A to minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 10 January 1973 p1 DHSC0105593_003. Why seek an inspection if its findings were not going to be relevant to the decision being made?
(1096) Appendix A to minutes of Committee on Safety of Medicines meeting 22 February 1973 p13 DHSC0003952_048. The CSM also advised that “this product should be regarded as new for the purpose of a special directive for the reporting of adverse reactions.” Product Licence for Kryobulin Antihaemophilic Fraction 22 March 1973 MHRA0033322_061
(1097) Annex C table of product licence applications for Factor 8 DHSC0003742_080
(1098) There is a detailed note of this: Note on visit of Dr Thomas to Immuno factories 22 June 1973 DHSC0103054_011. Dr Thomas happened to be in Vienna for a conference and expressed a wish to see Immuno’s factory. The Austrian authorities were happy to permit this, but he recorded they would have objected to an official inspection by a DHSS officer. Donors were paid, and screening of them for hepatitis risks was by counterelectrophoresis (“CEP”) (known already to identify less than half the infected samples screened). He was assured that donors were not “down and outs”. Immuno told him that they were paid two and a half times the amount paid in the US. He also described a worrying, shoulder-shrugging attitude to the spreading of hepatitis risks in the fractionation plant itself. Dr Thomas thought that the Quality Control and Research Development Laboratories were “excellent” and very much a contrast with some other parts of the factory which were “quite old fashioned”. It may be because this was officially an “informal” visit that the concerns it might have given rise to, and called for some discussion, appear not to have been raised with the CSM in any way which has been recorded. Separately, there is a troubling side note to this. On 3 April 1973 Dr Thomas was invited to speak at a meeting of the Scottish National Blood Transfusion Association. A summary of what he said can be found at: Minutes of Scottish National Blood Transfusion Association Regional Directors meeting 3 April 1973 p1 SBTS0000264_010. He is reported to have said: “Both the commercial products now licensed had come from factories inspected by DHSS; samples and protocols had been sent to the National Institute of Biological Standards and Quality Control … No British blood product underwent similar inspection.” If accurately recorded, this is in conflict with the apparent fact that there was no inspection until later, and then it was only informal. It also appears to imply that the inspections showed a satisfactory state of affairs, which at least in the case of Hemofil was simply not the case given his own inspection of the facilities.
(1099) Letter from Serological Products Ltd to DHSS 2 July 1975 MHRA0033322_014
(1100) Later screened as Blood Money parts 1 and 2: World in Action Blood Money Part 1 1 December 1975 MDIA0000113, World in Action Blood Money Part 2 8 December 1975 MDIA0000114, World in Action Blood Money Transcript 1 and 8 December 1975 PRSE0004591
(1101) Note on Professor Arie Zuckerman interview for Blood Money 14 October 1975 MGIL0000067
(1102) Background and current information for members of the Central Blood Laboratories Authority December 1982 p202 CBLA0002201, Minutes of Regional Transfusion Directors’ meeting 10 January 1973 pp7-8 NHBT0016114. The dates differ, and the latter reference is more likely to be accurate as to the date that all plasma was tested. The earlier reference however echoes other memories that screening began in November 1970.
(1103) They used immunoelectrophoresis (“IEOP”) or CEP. They would detect somewhere around a third only of the donations which were infective, and this was well known. World Health Organization Technical Report Series Viral Hepatitis: Report of a WHO Scientific Group 1973 p17 SCGV0000204_073
(1104) A passive haemagglutination or reverse passive haemagglutination (“RPHA”) test was used, which was thought to be more sensitive than CEP. It still left about one third of infections undetected, and slowly was superseded by a RIA test, which was more sensitive.
(1105) The principle of “scientific economy” – similar to the more colourful “Occam’s razor” – suggests that where one cause of an effect is known, there is little need to speculate that there is another. It is described, even more colourfully, in these terms: “If you hear the sound of hoofbeats outside the window, you do not rush to it expecting to see a herd of zebra”. In addition, it is for ease of understanding that the text refers to two major viruses: it has not been lost sight of that there were other viruses in blood which could cause post-transfusion hepatitis, albeit they are of much less overall effect and importance in the account of “what happened and why”.
(1106) Garrott Allen Commercially Obtained Blood and Serum Hepatitis Surgery, Gynecology and Obstetrics August 1970 pp1-2 RLIT0002180. The reference to Dr Krugman’s studies is Giles et al Viral Hepatitis Relation of Australia/SH Antigen to the Willowbrook MS-2 Strain New England Journal of Medicine July 1969 NHBT0029420
(1107) Garrott Allen Commercially Obtained Blood and Serum Hepatitis Surgery, Gynecology and Obstetrics August 1970 RLIT0002180
(1108) Walsh et al Posttransfusion Hepatitis after Open-Heart Operations Journal of the American Medical Association 12 January 1970 RLIT0000073
(1109) See in particular the chapter entitled “Is the Gift a Good One?” which is chapter 8 of the original edition. Titmuss The Gift Relationship 1970pp142-157 HSOC0019917
(1110) Alter et al Posttransfusion Hepatitis After Exclusion of Commercial and Hepatitis-B Antigen-Positive Donors Annals of Internal Medicine 1972 PRSE0001521
(1111) Grady et al Risk of Posttransfusion Hepatitis in the United States – A Prospective Cooperative Study Journal of the American Medical Association 1 May 1972 CGRA0000957
(1112) Garrott Allen The Epidemiology of Posttransfusion Hepatitis: Basic Blood and Plasma Tabulations 1972 PRSE0003483
(1113) Extract from Hospital Week – American Hospital Association No10 1972 DHSC0100024_079
(1114) Biggs et al Can Hemophilic Patients be Adequately Maintained with Cryoprecipitates? Or is it Desirable or Even Necessary to Manufacture and Administer Highly Concentrated AFH Products? Vox Sanguinis June 1972BAYP0000022_050
(1115) Jones Answering the needs of haemophilic children and their families Community Medicine 28 July 1972 p1 HSOC0022656
(1116) Kasper et al Letters to the Editor discussing Hepatitis and Clotting-Factor Concentrates Journal of the American Medical Association31 July 1972 PRSE0003913
(1117) In a report on the progress of the Medical Research Council (“MRC”) Cryoprecipitate Working Party Survey of the Incidence of Transfusion Jaundice, circulated for the April 1971 meeting of haemophilia centre directors, it was stated that: “The danger of infection can be calculated and will be related to the number of donors used to make the material used for treatment or the number of ‘donor exposures.’ If large pools of plasma are used to make therapeutic concentrates the theoretical danger of infection will be increased.” The report went on to note that in the subjects of the study (who would have been in receipt of domestically produced concentrates, not commercial concentrates at this time) the increased risk of “clinical illness” from the use of large pools was “not so great as to overbalance the advantages of the use of concentrates.” Jaundice and Factor-VIII Antibodies in Treated Patients with Haemophilia and Christmas Disease p2, p10 DHSC0002173_048. The expression “clinical” suggests that the dangers of chronic infection, which were established, were not in their direct consideration when drawing a comparison between concentrates and cryoprecipitate.
(1118) Although the International Forum referenced above supports a view that cryoprecipitate could be used in major surgery, given the choice of that or concentrate it seems clear that most if not all clinicians would have preferred to use concentrate.
(1119) Probably because it could more easily be stored and reconstituted by patients at home.
(1120) Chairman of the haemophilia centre directors and director of the Sheffield Centre.
(1121) Then Dr George Godber.
(1122) Letter from Professor Blackburn to Sir George Godber 12 December 1972 p2 BPLL0008096_002. The reason given for this need was that “The great shortage of materials is limiting the treatment that can be performed, particularly the introduction of Home Treatment.”
(1123) Note from Dr Maycock to Dr J J Reid 7 February 1973 BPLL0008090. Dr Maycock was Consultant Adviser to the CMO on Blood Transfusion.
(1124) The word “should” is of some importance when considering the question of self-sufficiency, examined in greater detail later in this Report.
(1125) When the Bureau of Biologics of the FDA in the US had a panel reviewing blood and blood derivatives in June 1976, it noted that the panel considered that where anti-haemophilic factor (“AHF”) was used to control spontaneous bleeding episodes in people with congenital Factor 8 deficiency the benefits of its use outweighed the risks presented by the product, and when used for surgery made the risks the equivalent to those with normal haemostatic function. Where prophylactic use was concerned, however, safety had not been well evaluated and “The risks may outweigh the benefits” and “A similar situation applies to recommendations for home therapy either in chronic low dose prophylactic use or for intermittent, episodic home therapy. Antihemophilic Factor (Human) usage is limited because of risk of transmitting viral hepatitis.” Minutes of Panel on Review of Blood and Blood Derivatives meeting 25 June 1976 p3 MULL0003445. The supply of cryoprecipitate and NHS concentrate was sufficient for the two former situations: however, the US deliberations might indicate the benefits of prophylaxis or episodic home treatment were likely to be outweighed by the risks, viewed overall.
(1126) This is what should have happened – see the chapter Consent – even if it is difficult to think that it would, given the very paternalistic nature of much of the interaction between patient and haemophilia doctors at the start of the 1970s.
(1127) Note from G A Drewe and R A Tunnard to Dr Maycock and others 25 June 1974 DHSC0100005_138, Note from G E John to Dr J J Reid DHSC0100005_044
(1128) Note from G Drewe and R Tunnard to Dr Maycock and others 25 June 1974 p1 DHSC0100005_138
(1129) ie the already reduced quantity: in short, there was less than one quarter of the originally anticipated uptake.
(1130) Note from G Drewe and R Tunnard to Dr Maycock and others 25 June 1974 p1 DHSC0100005_138. This low take-up might be explained by an over-enthusiasm amongst some (especially Dr Biggs of the Oxford Haemophilia Centre) for commercial concentrates leading to an overestimate of demand for it; or a reflection that regions were not keen to spend the money needed to supply the product to them unless satisfied it was strictly necessary, or a combination of both of these.
(1131) The manufacturer was recorded on the licence as Abbott Scientific Products Division, Abbott Laboratories in California: Abbott Laboratories Ltd Profilate Anti-Haemophilic Factor product licence 22 May 1975 CBLA0000006_009. The application was made in August 1974 and Abbott were informed in December 1974 that it would be granted subject to conditions: Letter from J Marriot to Dr M Duncan 14 January 1975 p16 MHRA0000091_012
(1132) An application to vary the product licence for Hemofil was approved on 13 June 1975, allowing for the use of RIA testing for Hepatitis B antigen: Travenol Laboratories Ltd Hemofil product licence alteration 13 June 1975 SHPL0000276_185, Travenol Laboratories Ltd Hemofil product licence renewal 19 February 1978 SHPL0000276_076. In respect of Kryobulin a similar application was granted on 14 October 1975: Serological Products Ltd Kryobulin product licence alteration application MHRA0033321_097, Serological Products Ltd Kryobulin product licence alteration 14 October 1975 MHRA0033321_099
(1133) The original tests for Hepatitis B were believed to identify around a third of the infections; RIA at least doubled this, but still left much undetected.
(1134) Abbott Laboratories Ltd application for Antihemophilic Factor product licence November 1974 p8 MHRA0000091_005
(1135) The report stated that the donors met the criteria of the regulations and each was tested for syphilis: Abbott Laboratories Ltd application for Antihemophilic Factor product licence November 1974 p5, p8 MHRA0000091_005
(1136) If anything, the use of the RIA test to exclude Hepatitis B might be thought to render it safer.
(1137) Letter from Dr Biggs to Dr Sheila Waiter 23 May 1974 CBLA0000206. The letter enclosed a draft letter to The Lancet; Biggs Supply of Blood-clotting-factor VIII for Treatment of Haemophilia The Lancet 29 June 1974 PRSE0002515. Blackburn Treatment of Haemophilia The Lancet 13 July 1974 WITN6914033
(1138) The manufacturer was recorded as Cutter Laboratories Inc of California, USA: Bayer UK Ltd application for Anti-Haemophilic Factor (Human) Koate product licence January 1976 p3 MHRA0009305
(1139) Bayer UK Ltd application for Anti-Haemophilic Factor (Human) Koate product licence January 1976 MHRA0009305
(1140) Bayer UK Ltd application for Anti-Haemophilic Factor (Human) Koate product licence January 1976 pp3-9 MHRA0009305. Presumably this was taken on trust, since no sufficient inspections could be carried out to check it given the wide range of ownership of the various sources. The absence of reports of hepatitis is particularly puzzling given what is now known about the likelihood that those taking factor concentrates would be infected. It may possibly be correct as to an absence of actual report, but the inference to be drawn from the comment (ie that the absence of report meant the absence of infection, and that Koate was free of any real risk of transmitting hepatitis) must be suspect. The product particulars in the eventual licence said that the presence of hepatitis should be assumed. Speywood Laboratories Ltd Anti-Haemophilic Factor (Human) Koate product licence 1 March 1977 p3 IPSN0000312_036
(1141) Bayer UK Ltd application for Anti-Haemophilic Factor (Human) Koate product licence January 1976 p1 MHRA0009305. The requirement for information was ongoing.
(1142) Pool size was 2,500 litres, from “at least 1000 individual donors”, but the DHSS were told that Cutter did not collect information about the rejection of donors. Nonetheless, they gave an assurance that “the collection of plasma is carried out according to the US Code of Federal Regulations”. Letter from J Boult to Dr Andrews 27 February 1976 IPSN0000312_109, Letter from J Boult to Dr R D Andrews 4 March 1976 BAYP0000001_113
(1143) Letter from the Committee on Safety of Medicines to the Licensing Authority 29 July 1976
MHRA0009276
(1144) Referred to subsequently as Bayer UK.
(1145) Letter from Dr Andrews to Bayer UK Limited 2 February 1976 BAYP0000001_110
(1146) Memo from J Kris Piper to Lowell Crow 23 February 1976 BAYP0000020_014
(1147) Letter from Dr John Holgate to Dr Maycock 15 May 1975 BPLL0004286. The letter thanked Dr Maycock for a copy of a proposed FDA rule on Hepatitis B testing.
(1148) Letter from J Boult to Dr Andrews 4 March 1976 BAYP0000001_113
(1149) Letter from D Bangham to Dr Andrews 18 March 1976 MHRA0009293
(1150) Letter from Dr Andrews to J Boult 7 May 1976 BAYP0000001_119
(1151) Speywood Laboratories Ltd Anti-Haemophilic Factor (Human) Koate product licence 1 March 1977 p3 IPSN0000312_036
(1152) Armour Pharmaceutical Company of Arizona USA was named as the manufacturer: Armour Pharmaceutical Company Ltd application for Factorate Factor VIII product licence March 1975 ARMO0000001
(1153) Armour Pharmaceutical Company Ltd application for Factorate Factor VIII product licence 16 October 1975 pp4-7 DHSC0105603
(1154) Minutes of Committee on Safety of Medicine Sub-Committee on Biological Substances meeting 12 November 1975 DHSC0105604_002, Committee on Safety of Medicines Sub-Committee on Biological Substances recommendation to grant product licence to Armour Pharmaceutical Company Ltd for Factor VIII DHSC0105604_005
(1155) Minutes of Divisional Management Group meeting 9 December 1975 pp3-4 MHRA0004180
(1156) Whilst the Supply Division and the Medicines Division were separate divisions within the DHSS, and there is no direct evidence of the thinking of the CSM(B) or CSM due to the limited information set out in the minutes that recorded their decisions, the possibility that the Supply Division’s “anxiety” that Factorate should be licensed due to its price, which was explicitly recorded in contemporaneous documents, created a pressure to license the product cannot be ignored. It should be recognised that through the passage of time, there has been a potential loss of evidence either way on this issue.
(1157) Minutes of Divisional Management Group meeting 9 December 1975 p4 MHRA0004180
(1158) Memo from Raymond Tringham to Mr Lillywhite at the DHSS 16 January 1976 DHSC0003742_077
(1159) The author was Raymond Tringham, an assistant secretary in the Medicines branch of the Medicines Division since the creation of CSM(B), according to the Secretary’s note about its membership, secretariat and staff. Note by Secretary of Committee on Safety of Drugs p3 MHRA0033745
(1160) See the discussion towards the start of this chapter.
(1161) Armour Pharmaceutical application submission for Factor VIII product licence p2 DHSC0003742_078
(1162) Note of Minister of State (Health) meeting 21 January 1976 DHSC0003742_076
(1163) Letter from Department of Health and Social Security to Armour 27 January 1976 p2 ARMO0000004
(1164) Letter from Armour to Department of Health and Social Security 2 February 1976 p1 ARMO0000005
(1165) Craske et al An outbreak of hepatitis associated with intravenous injection of Factor VIII concentrate The Lancet 2 August 1975 PRSE0001794
(1166) Minutes of UKHCDO meeting 1 November 1974 p5 HCDO0001017
(1167) Craske An outbreak of hepatitis associated with intravenous injection of Factor VIII concentrate The Lancet 2 August 1975PRSE0001794. The full text reads: “Treatment with factor-VIII concentrates exposes the patient to a higher risk of contracting transfusion hepatitis. Cryoprecipitate, in which each bag is made from one or two donations, carries a relatively low risk of hepatitis. Commercial factor-VIII concentrates, which are prepared from pools of 2 to 6000 litres of plasma obtained by plasmapheresis from paid donors, would be expected to carry a much higher risk of transfusion hepatitis … Commercial factor VIII concentrates should be reserved for the treatment of life-threatening bleeds in all haemophiliacs and for covering major operations. If used for treatment, commercial concentrates should be reserved for severely affected haemophiliacs, since they are more likely to be immune to hepatitis A and B.” Note that his view as to their use in severe haemophilia is not a third category to which their use should be reserved: the sentence begins with “If”, recognising that the realities of practice may not always correspond with the best advice of public health professionals.
(1168) Something may depend on the emphasis with which these words were spoken. “Best known” may mean “most familiar to the reader”, as in “He is best known for”. It may, however, mean “the best in quality amongst those products we know about”, as in “the best ‘known treatment’”. The idea that a product should be preferred merely because it is already the most well known amongst available treatments – the first reading of these words – makes little sense in context. Further, Dr Owen has since explained to the Inquiry in oral evidence that his principal reason for promoting self-sufficiency was that it would help to ensure the safety of blood products because those made from volunteer domestic donors – ie NHS concentrates – were already the safest amongst concentrates. Dr David Owen Transcript 22 September 2020 INQY1000055. Taking those two considerations into account, it seems that the better reading of these words is in the second sense. However, anyone reading the words shortly after the event could not be blamed for naturally thinking it was the first – and it is their effect on the reader with which this part of this chapter is centrally concerned. His view that safety was a reason for his push for self-sufficiency is supported by the evidence of Peter Wormald, Under-Secretary at the DHSS, who said: “The reasons for the policy were that imported products were very expensive and in general were considered to carry much higher risk of cross-infections, particularly hepatitis.” He went on to add that: “I do not believe that these reasons, or their relative importance, changed during the period in which I was active in this policy area, though it would be fair to say that the relative importance attached to cost and safety varied between individuals.” Written Statement of Peter Wormald para 5.1, para 5.3 WITN6934001
(1169) Parliamentary written answers on Haemophilia 22 January 1975 p2 DHSC0000274
(1170) Letter from Professor Garrott Allen to Dr Maycock 6 January 1975 CBLA0000249
(1171) It raises eyebrows that there should be such a dramatic intervention in the affairs of another state, until it is realised that this was a highly-respected scientist expressing concern about actions of his own countrymen which he saw as exporting disease and possibly death, and which he believed were avoidable.
(1172) World in Action Blood Money Part 1 1 December 1975 MDIA0000113, World in Action Blood Money Transcript 1 and 8 December 1975 PRSE0004591
(1173) World in Action Blood Money Part 2 8 December 1975 MDIA0000114, World in Action Blood Money Transcript 1 and 8 December 1975 PRSE0004591
(1174) Wellcome Witnesses to Twentieth Century Medicine – Haemophilia: Recent History of Clinical Management seminar Transcript 10 February 1998 p67 RLIT0000022
(1175) Minutes of Haemophilia Society Executive Committee meeting 11 December 1975 p3 HSOC0029671_045. Interestingly, the DHSS minute of the same meeting does not record Dr Owen’s promise to achieve self-sufficiency by 1977, though it does record concern by the Society that the volume target set for self-sufficiency might be too low (an MRC study had suggested that in practice 500,000 rather than 340,000 units were needed) and suggested more use of plasmapheresis might be an answer. It also records Dr Owen stressing “his personal commitment to self-sufficiency”. Note of Minister of State (Health) meeting 11 December 1975p1DHSC0100006_093. It does not record criticism of the regional structure of the blood transfusion service, though Dr Owen would take Dr Maycock’s advice on this, recorded in a Department of Health minute dated 23 June 1976. Memo from M Draper to Mr Benner 23 June 1976 DHSC0003738_054
(1176) Cash Commercial and NHS Factor VIII Concentrates British Medical Journal 24 January 1976 PRSE0004064. Dr Cash had been director of the regional transfusion centre in Edinburgh since 1974 and would become national medical director of the Scottish National Blood Transfusion Service (SNBTS) in 1979.
(1177) They are also implicit in the evidence of Peter Wormald. Written Statement of Peter Wormald para 5.1, para 5.3 WITN6934001
(1178) Letter from US Assistant Secretary of Health to Dr Yellowlees 24 November 1975 p3 DHSC0100001_036
(1179) Like Dr Walford, Dr Waiter would move from the Medicines Division to the Scientific Services, Equipment and Building Division where she would be Dr Walford’s immediate predecessor. Letter from Dr Waiter to Dr Raison 30 December 1975 DHSC0100001_023
(1180) Draft letter to Dr Raison 23 January 1976 p2 DHSC0100001_018
(1181) Dr Walford said in evidence that shortly after she joined the Medicines Division of the DHSS in 1976 she accompanied two assessors and Dr Lane on a visit to the US. She saw two facilities, and compiled a report which reflected poorly upon the manufacturer. It appears however to have been at the production end of the chain since she did not recount visiting a blood collection centre: Dr Diana Walford Transcript 19 July 2021 pp21-22 INQY1000136. Dr Holgate partly explained this on the basis of cost – not, this time, the cost of the product but the cost to the DHSS of arranging inspections abroad: Minutes of Divisional Management Group meeting 9 December 1975 p1 MHRA0004180. It is difficult to understand why, if that was a problem, it could not have been solved by requiring the inspection to have been at the expense of the applicant for a licence, rather than be an unrecovered cost of the licensor.
(1182) Minutes of Divisional Management Group meeting 9 December 1975 pp3-4 MHRA0004180
(1183) See the chapter on Hepatitis C Surrogate Screening.
(1184) Immuno Ltd Kryobulin product licence alteration 11 November 1976 MHRA0033321_085. This product licence alteration was approved on 7 March 1978 MHRA0033321_084
(1185) Minutes of UK Haemophilia Centre Directors meeting 6 April 1979 pp2-3 HCDO0000403
(1186) Professor Ingram was the haemophilia centre director at St Thomas’ Hospital, London.
(1187) This would be surprising if accurate, since what was implied to be the “safer” material (that of European origin) was already available, and until Immuno succeeded in varying its licence to permit it to manufacture product from plasma sourced from the US the cheaper material could not be marketed in the UK. As clarified by Professor Ingram afterwards, Mr Berry had not, in fact, said this as reported.
(1188) Minutes of UK Haemophilia Centre Directors meeting 6 April 1979 p4 HCDO0000403, Minutes of Haemophilia Reference Centre Directors meeting 15 October 1979 p3 PRSE0000539
(1189) Immuno Ltd Kryobulin product licence alteration 11 November 1976 MHRA0033321_085
(1190) Counsel Presentation on Pharmaceutical Companies Transcript 24 September 2021 pp31-36 INQY1000147
(1191) The original and the translation are at: Minute of telephone conversation between Dr Schwarz and Mr Berry original 25 November 1976 SHPL0000071_083, Minute of telephone conversation between Dr Schwarz and Mr Berry translation SHPL0001094. The date of the meeting is 24 November 1976, thus nearly a fortnight after the application to vary the licence (which was dated 11 November 1976) had been lodged.
(1192) Annual UK sales compiled in June 1983: Memo from C Wrigglesworth to others 28 June 1983 p2 DHSC0002229_055
(1193) It was understood in the 1970s that paid donors were much more likely than voluntary non-remunerated donors to transmit hepatitis, and other blood-borne infections which were not purely confined to one locality. See, for example, Grady et al Risk of Posttransfusion Hepatitis in the United States – A Prospective Cooperative Study Journal of the American Medical Association 1 May 1972 CGRA0000957
(1194) In her second written statement concerning the licensing of the variation, Dr Walford has looked to see what research was available that might be the material reflected in the internal company note. It is right to record that there does not appear to be a persuasive study known of at the time to establish the points reflected in the note. Written Statement of Dr Diana Walford paras 15.1-15.11 WITN4461158. Moreover, Dr Walford has, correctly, pointed out when Hemofil and Kryobulin, as originally licensed, were compared to see if one caused more hepatitis than the other by Dr Peter Kirk (whose view was echoed by Dr David Magrath of NIBSC: Letter from Dr Kirk to Dr Magrath 1 April 1977 CBLA0000590; with the response: Letter from Dr Magrath to Dr Kirk 20 April 1977 HHFT0000925_002), he could not make any distinction between the two on the grounds of risk. The study by Dr Craske of the outbreak in Bournemouth (see above in the text) was linked by him to Hemofil, but this is not an adequate basis for saying that as a matter of generality European paid donors were less infective than US paid donors. In short, there was no compelling medical research or commentary which would have required a different approach by the regulator. Dr Walford regards it as an open question, even now, whether European plasma as used by Immuno was safer than US-sourced plasma as used by pharmaceutical rivals.
(1195) This is probably a matter of common knowledge, but in any event is supported both by the timing of the parent legislation and by what Dr Thomas said in his statement. Written Statement of Dr Duncan Thomas para 2.5 WITN6405001
(1196) This is not to lose sight of the fact that treatment with concentrate could be given faster, reducing pain, could be more accurately given in an appropriate dose, and could be given in lesser volumes which avoided risks of creating too large a circulating volume for the heart to cope well; nor does it lose sight of the fact that the quality of cryoprecipitate varied across the country, further complicating the picture.
(1197) Dr Saad Al-Ismail (Swansea, Morriston Hospital) said: “Well, maybe in retrospect it was probably a misplaced trust in the medicine licensing agency in the UK, in that we never used a product which is not licensed. We never used a product which has not proved to be efficacious. This is what the statement is based on, in that whatever we used were [sic] supposedly licensed, and to be licensed you had to have a safe and efficacious product. But, you know, that -- I mean, we could talk about that later on if you want, but that is our trust in the system in the UK, like you trust that system for any medicine you use.” Dr Saad Al-Ismail Transcript 17 November 2020 p48 INQY1000074
(1198) Travenol Laboratories Ltd application for Hemofil product licence January 1973 p14 DHSC0105593_006
(1199) This is not to say that an unlicensed product is necessarily unsafe – rather, that where a clinician knows that it is, any decision to use it will be (or should be) deliberate and balanced in the light of that: the named patient basis involves a degree of thought and careful decision-making which may not be possible in more pressured environments. Hence the word “routinely”, which allows for exceptions.
(1200) A point perhaps highlighted by the low take-up of Hemofil and Kryobulin in the first year after they had been licensed, to a level less than a quarter of the demand the DHSS had at first anticipated.
(1201) Though this did not preclude a product being “de-licensed” in the meantime – as might well have happened in 1986 if Armour had not then agreed to withdraw its heat-treated products voluntarily from the UK market (see the chapter on Pharmaceutical Companies).
(1202) The Inquiry has not been able to locate consideration by CSM(B) or CSM of relevant renewals for this period.
(1203) Appendix C to minutes of Committee on Safety of Medicines meeting 22 January 1981 MHRA0036365_018, Memo from J Savage to A Gover 4 January 1990 IPSN0000139_022. The last batch of Koate imported by Speywood was released by DHSS in February 1980.
(1204) Appendix C to minutes of Committee on Safety of Medicines meeting 22 January 1981 p2 MHRA0036365_018
(1205) Original emphasis. The history of this episode is conveniently summarised in: Appendix C to minutes of Committee on Safety of Medicines meeting 22 January 1981 p5 MHRA0036365_018
(1206) This is the reasonable conclusion from what is set out above. The reason for seeking the information as to donors, rate of rejection, source etc is not to build up a knowledge resource for the sake of it, but to see if those data reassure the analyst that the product to which they relate is safe. If the data are simply missing – as in the case of Speywood – or inadequate (as it seems to have been in respect of Koate and Factorate) – then if safety is the criterion (as it was expressly and emphatically in the case of Speywood) the product should not be licensed nor continue to be.
(1207) Documentary or from oral or written testimony.
(1208) If this Inquiry had been held 25-30 years ago, it seems likely that more evidence would be available to illuminate the decision, and either support a judgement that it was wrong or explain why it was right. I have, however, to reach a decision on the material that is available to me, rather than speculate what it might have been.
(1209) As set out above.
(1210) It is of interest that some later comment touching on the decision to allow importation in 1973, made by Dr Arthur Codd, a virologist in Newcastle, was reported in The Journal (a paper in the north of England): The Journal My Anger Over Blood Deaths 19 February 2001 p6 CGRA0000835. He said that it was known that viruses were transmitted in this way: “we knew there was always a risk there might be other things lurking there” adding that it had always been his advice to create a “pedigree herd” of volunteer donors in the UK in order to minimise the risk of infection. In respect, it appears, of a decision to import commercial concentrates he said: “We could not have met demand at that time but we could have continued with the older products until Britain became self-sufficient.” He went on to say that it was well known that US pharmaceutical companies“scoured the world for cheap plasma.” An article written later in the same year as Hemofil and Kryobulin was licensed was more forceful still. Its authors were prestigious: Dr Harvey Alter (later given the Nobel prize for his work on hepatitis in blood), Professor Paul Holland, Dr Robert Purcell and Dr John Gerin. In the journal Blood they concluded that AusRia (“RIA”) testing, which by then was available, was clearly more sensitive than CEP for revealing Hepatitis B surface antigen (“HBsAg”). They concluded, however, with these words: “Lastly, it is important to emphasize that the impact of HBAg testing on posttransfusion hepatitis is minimal when compared with the potential impact of eliminating the use of commercial blood. By far, the single most significant measure for the reduction of posttransfusion hepatitis is the total exclusion of the commercial donor.” Alter et al The Ausria Test: Critical Evaluation of Sensitivity and Specificity Blood December 1973 p11 RLIT0002022
(1211) Letter from Professor Bloom to Dr Holgate 10 March 1981 DHSC0001191. Dr Holgate was the principal medical officer in the Medicines Division who dealt with biological products.
(1212) His letter described this as “somewhat irregular”.
(1213) Letter from Dr Holgate to Professor Bloom 23 March 1981 BPLL0001351_039. In essence, Speywood had distributed Koate (manufactured by Cutter in the US) in the UK from June 1976 to the end of 1979, and was licensed to do so. Cutter then decided to market Koate in the UK under its own licence, rather than via Speywood. Some stocks of Koate remained in the possession of Speywood. A US company (Parlier Medical Supply Company) agreed to buy Koate from Cutter in the US, and then to sell it on, unlabelled, to Speywood. Speywood then obtained a variation to its licence which permitted it to sell those stocks and, further, to import unlabelled Koate for relabelling and sale in the UK using the brand name Humanate. NIBSC became aware of this and was concerned about the impossibility of tracing product back to its donor sources. The Licensing Authority then informed Speywood that the terms of the licence could be varied such as to mandate the provision of certain information in the protocols provided during the batch release process. This information would include evidence of the source and date of the collection of the donor blood, the date of manufacture of the concentrate, and the results of the tests done during and on completion of manufacture. Though Speywood appealed, the CSM considered the variation appropriate, and the licence was varied in accord with it. However, at the time Professor Bloom wrote, this had not yet become public. The release of the last batch of Humanate to be sold was authorised on 13 December 1980: that which followed (around 21 January 1981) was not. However, some of the December batch was still being sold in June 1981. A number of adverse reports were associated with Humanate, and this may have been the catalyst for Professor Bloom to write as he did.
(1214) Between November 1976 and August 1979 in her post as a civil servant in the Medicines Division. Dr Diana Walford Transcript 19 July 2021 pp15-21, pp22-23 INQY1000136
(1215) He described his visit to Michael Gillard during the latter’s preparatory interviews for the World in Action programme Blood Money screened in December 1975. Note on Professor Arie Zuckerman interview for Blood Money 14 October 1975 MGIL0000067
(1216) Appendix A to minutes of Committee on Safety of Medicines meeting 22 February 1973 p13 DHSC0003952_048. The CSM also advised that “this product should be regarded as new for the purpose of a special directive for the reporting of adverse reactions.” Appendix A to minutes of Committee on Safety of Medicines meeting 22 February 1973 p10 DHSC0003952_048
(1217) Letter from Dr Holgate to Professor Bloom 23 March 1981 BPLL0001351_039
(1218) Minutes of Divisional Management Group meeting 9 December 1975 p1 MHRA0004180
(1219) See the chapter on Pharmaceutical Companies.
(1220) For over ten years there had been convincing evidence of the significantly greater risk to be expected from prison donations than others. For one example see the article: Allen Commercially Obtained Blood and Serum Hepatitis Surgery, Gynecology and Obstetrics August 1970 RLIT0002180
(1221) Dr Holgate had also said (see above, in the discussion of the Factorate application) that “what was needed was to strengthen the requirements in the product licence, and to insist on returns from each collecting centre including the rate of rejection of donors or donations.” Minutes of Divisional Management Group meeting 9 December 1975 p4 MHRA0004180. It could have been done, but it is precisely what was not done when the applicant companies showed unwilling to provide it unless pressed harder. In the case of the applications to licence both Koate and Factorate the indirect controls exercised could not sensibly be said to amount to “detailed knowledge and control over early stages of manufacture and in-process control” when the companies did not provide the assurances and materials sought as set out above. Letter from Dr Holgate to Professor Bloom 23 March 1981 p1 BPLL0001351_039
(1222) Centers for Disease Control Epidemiologic Aspects of the Current Outbreak of Kaposi’s Sarcoma and Opportunistic Infections New England Journal of Medicine 28 January 1982 OXUH0002850
(1223) Report of ISH/ISBT Congress Budapest August 1982 p33 PRSE0003247
(1224) A positive HBsAg test result indicates current Hepatitis B infection.
(1225) Letters from Alpha: Letter from Marietta Carr to Dr Meyer 30 August 1982 CGRA0000277, Letter from Marietta Carr to Dr Meyer 7 September 1982 CGRA0000657
(1226) Memo from Steven J Ojala, Cutter, to those listed, re: AIDS and FDA. summarising meeting between Blood Product Manufacturers and Dr Donohue (FDA) concerning ways to minimise the risk of AIDS CGRA0000425. See also Counsel Presentation on Pharmaceutical Companies: Response to Risk Transcript pp12-13 INQY0000311
(1227) Minutes of Haemophilia Reference Centre Directors meeting 6 September 1982 p11 HCDO0000410
(1228) Centers for Disease Control Update on Acquired Immune Deficiency Syndrome (AIDS) – United States Morbidity and Mortality Weekly Report No37 24 September 1982 p1 OXUH0002848
(1229) 50 of these cases were reported from 10 foreign countries.
(1230) By Dr James Curran; Acquired Immune Deficiency Syndrome (AIDS) 12 October 1982 MULL0003226
(1231) Centers for Disease Control Update on Acquired Immune Deficiency Syndrome among Patients with Hemophilia A Morbidity and Mortality Weekly Report No48 10 December 1982 p6 PRSE0003276
(1232) Cytomegalovirus.
(1233) The Acquired Immune Deficiency Syndrome (AIDS) 5 November 1982 pp2-3 CBLA0001653_003. This report was revised on 1 March 1983 and sent to all UKHCDO doctors on 22 March. Letter from Dr Craske, Dr Rizza and Professor Bloom to haemophilia centre directors 22 March 1983 HCDO0000517_001, The Acquired Immune Deficiency Syndrome (AIDS) 1 March 1983 HCDO0000517_002. They would have been aware of its contents beforehand: if not in 1982, when Dr Craske first wrote it, then at the latest on 24 January 1983 when many of the haemophilia centre directors in England and Wales met at the Excelsior Hotel at London Heathrow Airport, and heard a presentation by Dr Craske about AIDS and its probable causes.
(1234) Health Authority Defendants Reportby Dr Rizza p76 HCDO0000394
(1235) Centers for Disease Control Update on Acquired Immune Deficiency Syndrome among Patients with Hemophilia A Morbidity and Mortality Weekly Report No48 10 December 1982 pp4-5 PRSE0003276
(1236) Centers for Disease Control Epidemiologics Notes and Reports Immunodeficiency among Female Sexual Partners of Males with Acquired Immune Deficiency Syndrome (AIDS) – New York Morbidity and Mortality Weekly Report No52 7 January 1983 p2 PRSE0003270
(1237) Letter from I Marshall of Alpha Therapeutic UK Ltd to Professor Bloom 16 March 1983 p2 CBLA0000060_067; the letter enclosed a press release issued by Alpha Therapeutic Ltd.
(1238) There are two records of the meeting: Letter from Norman Berry to Dr Peter Kernoff 16 March 1983 RFLT0000050, Notes of Immuno meeting 24 January 1983 PRSE0002647
(1239) ie it could not be treated if it arose.
(1240) A prestigious US medical journal much read in the UK.
(1241) Ragni et al Acquired Immunodeficiency-like Syndrome in Two Haemophiliacs The Lancet 29 January 1983 STHB0000771_006
(1242) Omar Sattaur AIDS: transfusion patients may be at risk New Scientist 3 February 1983 PRSE0000726
(1243) The Dutch Association of Haemophilia Patients wrote to members on 27 February 1983 and the guidelines were published in the Dutch Journal of Medicine in May 1983. The Krever Report 1997 pp922-923 KREV0000001
(1244) Centers for Disease Control Prevention of Acquired Immune Deficiency Syndrome (AIDS): Report of Inter-Agency Recommendations Morbidity and Mortality Weekly Report No8 4 March 1983 p1 SBTS0003036_004
(1245) It did not adopt its present name until 1983, when it adopted a formal constitution – but it was active in the latter part of 1982.
(1246) Two possibilities which had been suggested to explain the original appearance of an outbreak linked to men having sex with men.
(1247) Evatt The Tragic History of Aids in the Hemophilia Population 1982-1984 2007 pp4-5 CVHB0000042
(1248) For instance, an epidemiologist from the German national institute for infectious diseases (Dr L’age-Stehr, of the Robert Koch Institute in Berlin) visited the CDC in November 1982. She reported in the federal health bulletin (Bundesgesundheitsblatt) that AIDS appeared to be caused by an unknown infectious agent transmitted through blood and blood products. Her report was widely published, being reprinted in the German medical gazette, distributed to all physicians, on 18 February 1983. The Krever Report 1997 p855 KREV0000001. It is to be inferred that others too came to similar views. In his report, Mr Justice Krever reports “As early as January 1983, [the Ministry in the Netherlands] had discussed the possibility of prohibiting imports of factor VIII concentrate.”The Krever Report 1997 p924 KREV0000001
(1249) Letter from I Marshall of Alpha Therapeutic UK Ltd to Professor Bloom p2 16 March 1983 p2 CBLA0000060_067; the letter enclosed the press release issued by Alpha Therapeutic Ltd. It is worth noting that in an internal memo of 29 December 1982, Edward Cutter, of Cutter Pharmaceutical, wrote that that company too might consider being open about the risk for those who consumed its products. Memo from Edward Cutter to Jack Ryan and others 29 December 1982 CGRA0000434. It is probable that it was some time after this, however, that this internal memo was acted upon.
(1250) The sense is, however, that it was a recommendation that if it were not acted upon might lead to obligatory requirements being imposed – in much the same way as a police officer’s recommendation to a citizen that they should “move along” might be observed, for fear of stricter enforcement if it were not complied with.
(1251) Notifications from the FDA: Letter from John Petricciana of the FDA to all licensed manufacturers of plasma derivatives 24 March 1983 DHSC0001203, Letter from John Petricciana of the FDA to all establishments collecting human blood for transfusion 24 March 1983 DHSC0001204
(1252) He was director of NISBC from 1976 to August 1985. He was a member of the CSM from 1978 to 1986, sat on the CSM(B) from 1980 to 1986 and chaired the CSM(B) from 1981 to 1986. Written Statement of Sir Joseph Smith paras 2.3-2.4 WITN5281001
(1253) Letter from Dr Smith to Dr Fowler 28 March 1983 CBLA0000043_034
(1254) It is unclear why it took the CSM(B) so long to meet, Dr Smith having identified the need for a meeting back in March; the fact that the CSM(B) did not meet until mid July suggests a worrying lack of urgency.
(1255) See the chapter Role of Government: Response to Risk. Dr Galbraith’s letter to Dr Ian Field of 9 May 1983 is at: Letter from Dr Galbraith to Dr Field 9 May 1983 CBLA0000043_040
(1256) Agenda for Committee on Safety of Medicines Sub-Committee on Biological Products discussion on AIDS in relation to licensed blood products 13 July 1983 DHSC0001209
(1257) The agenda also contains hand written notes, but it is not known whose handwriting it is. Agenda for Committee on Safety of Medicines Sub-Committee on Biological Products discussion on AIDS in relation to licensed blood products 13 July 1983 DHSC0001209. Dr Barrowcliffe was not involved in the CSM(B) meeting in July 1983. He says in his statement to the Inquiry, however, that “it was unusual but not unknown for meeting agendas to include possible conclusions on the face of it. I do not think it was typical of the way Dr Joseph Smith worked or the manner in which he chaired and conducted meetings.” Written Statement of Dr Trevor Barrowcliffe para 7.24 WITN6408001. Dr Walford thought it was a “fairly unusual format”. Dr Diana Walford Transcript 21 July 2021 p81 INQY1000138
(1258) In his statement to the Inquiry, Dr Smith thought it likely that he would have sought Dr Fowler’s views and those of others with expertise in haemophilia and its treatment and the manufacturing processes for such products. Written Statement of Sir Joseph Smith paras 3.30-3.31 WITN5281001. These descriptions suggest that those that he thought he was likely to have asked would have been Dr Fowler himself, Professor Bloom and Dr Lane. However, Dr Smith also attended an internal DHSS meeting that took place on 3 June 1983. It is conceivable that the suggested conclusions were influenced by the content of the discussions at that meeting.
(1259) The agenda went on to address other products: the Hepatitis B vaccine, immunoglobulin and albumin. Agenda for Committee on Safety of Medicines Sub-Committee on Biological Products discussion on AIDS in relation to licensed blood products 13 July 1983 p3 DHSC0001209
(1260) The paper which Dr Fowler produced at Dr Smith’s request was entitled Acquired Immune Deficiency Syndrome (AIDS): a new hazard for haemophiliacs? It might be inferred from the question mark at the end of the title that Dr Fowler himself regarded it as questionable whether AIDS posed a risk to people with haemophilia. It is a curious paper, whose author appeared to be highly doubtful as to whether AIDS was caused by a single transmissible virus. It read, in its material parts: “AIDS is clearly a transmissible condition. The repeated intimate contacts with transfer of saliva, urine, blood and sperm, which appear to favour its transmission are very much a feature of the ‘gay scene’ in New York, Los Angeles, San Francisco, Miami and Haiti, a holiday resort much favoured by US homosexuals. On this basis, the popular press has seized on the search for a single causative agent, probably a virus. If this were so, transmission of AIDS from affected blood donors to haemophiliacs would be a real possibility. However, even if we accept the single virus theory, there are still snags. Transmission would require donation during a period of viraemia. Chronic, asymptomatic viraemia would be unlikely and donors would tend not to donate while feeling unwell as presumably they would as a result of an acute viraemia which would almost certainly produce symptoms. The concept of an acute viral infection acting as a trigger in a susceptible individual makes transmission by blood products even less likely. Putting aside speculation about ‘recreational drugs’ such as nitrates, the most convincing hypothesis so far for the aetiology of AIDS is advanced by Sonnabend et al (1983). This suggests that repeated exposure to allogeneic sperm together with cytomegalovirus (CMV) over a prolonged period impairs T Cell mediated immunity, allowing reactivation of Epstein Barr Virus (EBV). Both viruses are almost universal among sexually active homosexuals and the part played by sperm ties in with the observation that it is the passive homosexual who gets AIDS rather than his active partner. Whether or not this hypothesis is valid, it must cast doubt on the simple transmission of ‘gay’ AIDS to ‘straight’ haemophiliacs who are in some way predisposed to the syndrome. Is it not possible that the odd case of ‘haemophiliac’ AIDS may have occurred during the ten years or so that AHF concentrate has been available? Is it not possible that ‘haemophiliac’ AIDS may require years of repeated treatment with large quantities of concentrate? In a word, is it not possible that ‘haemophiliac’ AIDS may be a function of the concentrate itself rather than a specific agent transmitted by homosexuals with or ‘incubating’ AIDS?” Acquired Immune Deficiency Syndrome (AIDS); A New Hazard For Haemophiliacs? July 1983 pp2-3 DHSC0002229_059
Phrases such as “even if we accept”, “there are still snags”, and “even less likely” serve to cast substantial doubt on the idea of viral transmission, as do the series of rhetorical questions posed by Dr Fowler. The significance of the long latency period between an infection and the appearance of symptoms seemed to have been overlooked by him at this point in his paper (“chronic asymptomatic viraemia would be unlikely”) although it is referred to explicitly by him later, and it is unclear whether his assumption that “donors would tend not to donate while feeling unwell” took into account the position of paid, as opposed to voluntary, donors. The paper by Sonnabend and others, the only paper referenced by Dr Fowler, was characterised by the latter as advancing “the most convincing hypothesis so far” without any paper expressing a rival view being compared. Sonnabend et al Acquired immunodeficiency Syndrome, Opportunistic Infections, and Malignancies in Male Homosexuals Journal of the American Medical Association 6 May 1983 OXUH0002239_005. Yet the evidence available to the Inquiry suggests that by this stage the single virus theory was widely accepted as the most likely hypothesis; and when searching for an unknown cause of AIDS to suppose that there might be a different cause in the cases of haemophiliacs than in the cases of other sufferers (“haemophiliac AIDS” as opposed to “ordinary” AIDS) is to ignore generally sound scientific principles.
In essence, the Sonnabend theory was that the bombardment of recipients of blood products by a large range of different proteins, recognised by recipients’ immune systems as “foreign” and consequently provoking an immune reaction, eventually overloaded the immune system of the recipient to the point that it failed.
It is difficult to see how this theory, if accepted despite its obvious shortcomings, could help to answer the question to be answered by the CSM(B), which was whether or not to suspend the importation of factor concentrates manufactured commercially in the US. The logical conclusion from Dr Fowler’s paper would be that the large pool concentrates from the US should be denied entry to the UK because of the increased risk they posed to those people with haemophilia who might receive them (assuming that the risk of recipients developing AIDS was thought to be of sufficient magnitude).
It is right to note that Dr Fowler went on to say that “one cannot ignore other views and hope that the problem will go away.” The “media concept of a ticking time bomb” was, he said, a “very real one for haemophiliacs and no effort should be spared to protect them by all practical means.” He considered possible precautions: the first was the use of indirect markers such as those for syphilis and Hepatitis B, which would, he suggested, “remove many homosexual donors”. The second was to “appeal” to “active” homosexuals to exclude themselves voluntarily from blood donation for the time being. The third was the suggestion “in some quarters” that there should be explicit questionnaires about sexual activity. The latter was not supported by Dr Fowler, on the basis that it would probably be little more effective than propaganda to encourage voluntary exclusion and “would certainly alienate many ordinary donors.” The fourth possible precaution was the use of cryoprecipitate. It might be thought somewhat remarkable that Dr Fowler described the evidence that cryoprecipitate made from single donations or very small donor pools, was safer than concentrate made from pools of thousands of donations as “scanty” and “very suspect”, although he then acknowledged that if a patient with haemophilia could be managed on cryoprecipitate alone, it made good sense to do so, as it minimised the number of donations to which a patient was exposed.
Dr Fowler then turned to “the problem of imported concentrate”. Referring to the FDA’s recommendations, he considered that it “behoves us” to ensure that concentrate imported from the US was not prepared from plasma obtained prior to the implementation of the FDA recommendations, and suggested the use of stop orders by NIBSC as a means to accomplishing this.
Notwithstanding his apparent scepticism about the cause (and possibly extent) of the risk, Dr Fowler’s conclusion, having expressed the hope that there was no ticking time bomb, was that it was essential that such methods as were available should be used to minimise “this potential hazard”.
It may be that Dr Fowler’s views were influenced by a letter he had received during the previous month from Cutter questioning whether “the syndrome contracted by hemophiliacs [sic] really is the same as the AIDS syndrome contracted by other high risk groups.” Letter from J Ashworth to Dr Fowler 3 June 1983 p1 BAYP0000002_183
(1261) Acquired Immune Deficiency Syndrome (AIDS); A New Hazard For Haemophiliacs? July 1983 pp3-4 DHSC0002229_059
(1262) Written Statement of Sir Joseph Smith para 3.32(a) WITN5281001
(1263) Dr Diana Walford Transcript 20 July 2021 pp122-124 INQY1000137
(1264) Minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 13 July 1983 ARCH0001710
(1265) Dr Smith (chairman and NIBSC director), Professor Dudgeon (professor of microbiology at The Hospital for Sick Children, Great Ormond Street), Professor Jenkins (haemophilia centre director at the London Hospital), Professor Lambert (professor of microbial diseases, St George’s Hospital), Dr Lane (BPL director), Professor Melling (director of the Vaccine Research and Production Laboratory at Porton Down), Dr Pollock (CDSC), Dr Tyrell (MRC communicable disease director) and Mr Watt (Protein Fractionation Centre director). See also: Written Statement of Sir Joseph Smith paras 3.28-3.30 WITN5281001
(1266) Archer Inquiry Transcript 29 August 2007 p120 ARCH0000009
(1267) Minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 13 July 1983 ARCH0001710, Agenda for Committee on Safety of Medicines Sub-Committee on Biological Products discussion on AIDS in relation to licensed blood products 13 July 1983 DHSC0001209
(1268) Agenda for Committee on Safety of Medicines Sub-Committee on Biological Products discussion on AIDS in relation to licensed blood products 13 July 1983 DHSC0001209. The authorship of the annotations is not known.
(1269) Minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 13 July 1983 p2 ARCH0001710
(1270) The Acquired Immune Deficiency Syndrome (AIDS) 5 November 1982 CBLA0001653_003. It was updated further in March 1983, and circulated to UKHCDO directors. The Acquired Immune Deficiency Syndrome (AIDS) 1 March 1983 HCDO0000517_002
(1271) His letter was in reply to a request from Professor Bloom for information as to the latest position in the US. Letter from Dr Evatt to Professor Bloom 7 March 1983 p1 DHSC0001175
(1272) Minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 13 July 1983 p2 ARCH0001710
(1273) There was separate minuting of the decisions in respect of concentrates generally, and US concentrates.
(1274) Summary of the Main Points from a Consideration of AIDS and Licensed Blood Products 13 July 1983 p2 DHSC0001208, Minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 16 June 1983 p2 ARCH0002485_002
(1275) Written Statement of Dr Diana Walford para 99.3(i) WITN4461001
(1276) Acquired Immune Deficiency Syndrome (AIDS)22 April 1983 CBLA0001697
(1277) Dr Colin Entwistle (Oxford) said they could have made the switch away from providing plasma to BPL to producing cryoprecipitate in a matter of days. Dr Colin Entwistle Transcript 6 December 2021 p26 INQY1000167. Dr Brian McClelland (Edinburgh) said “it could have been done very quickly. We would have had … enormous community support in doing that, which would have made it go very quickly.” Dr Brian McClelland Transcript 27 January 2022 pp131-132 INQY1000177. Dr Morris McClelland (Belfast) said it would have been possible to reprioritise production. Dr Morris McClelland Transcript 1 February 2022 pp115-116 INQY1000179. Dr Jean Harrison (North East Thames) in her statement said that the North East Thames Regional Transfusion Centre would have been able to increase their production of cryoprecipitate very quickly, but there would not have been enough plasma to treat all people with bleeding disorders with cryoprecipitate, and so the patients may have had to accept being treated in response to a bleed rather than prophylactically. Written Statement of Dr Jean Harrison paras 198-199 WITN7046001. When asked if it would have been possible to increase cryoprecipitate as an interim measure in response to the AIDS crisis, Professor Dame Marcela Contreras (North London) said: “To a large extent, but we were not asked to do it. But we had the capability to do it.” Professor Dame Marcela Contreras Transcript 2 December 2021 pp149-150 INQY1000165. Dr Tony Napier (Cardiff) said that if Professor Bloom had asked the Cardiff Regional Transfusion Centre to “switch emphasis totally from concentrate towards cryoprecipitate, we would have done our best to put that into place.” Dr Tony Napier Transcript 30 November 2021 p180 INQY1000163. Dr William Wagstaff said one of the reasons for meeting haemophilia clinicians was to discuss whether “they wanted to change back to cryoprecipitate away from concentrate until the question of infectivity was sorted out” and that it caused him “some discomfort” that they did not since they could have provided enough cryoprecipitate to meet demands. Written Statement of Dr William Wagstaff paras 165-167, para 192 WITN6988001. He could have met any increased demand for cryoprecipitate “in terms of weeks rather than months”. Dr William Wagstaff Transcript 25 January 2022 p48 INQY1000175. Although this evidence has been given nearly 40 years after the meeting, there is a compelling commonality about it. It has, however, to be acknowledged that Dr Gunson, who had a general oversight of the blood transfusion service was present at the meeting, and might be expected to make a contribution on the question of supply.
(1278) Written Statement of Sir Joseph Smith para 3.49 WITN5281001
(1279) Written Statement of Sir Joseph Smith para 3.50 WITN5281001
(1280) Evidence of Sir Joseph Smith to the Archer Inquiry 27 August 2007 p3 ARCH0000442_005
(1281) Written Statement of Sir Joseph Smith para 3.46 WITN5281001. In his statement to the Inquiry Sir Joseph suggested that the discussion at a DHSS meeting on 3 June 1983 may have caused him to “expect that self-sufficiency could possibly be reached within perhaps six months.” Written Statement of Sir Joseph Smith para 3.22 WITN5281001
(1282) Dr Diana Walford Transcript 21 July 2021 pp99-101 INQY1000138
(1283) Though the CSM(B) were most probably unaware of it, it appears that the French were offered heat-treated product by Hyland and Behringwerke earlier in 1983: Cutter learned on 11 May 1983 that as a result the French had stopped all imports “until they can evaluate the information and offers they have received insofar as they relate to the hepatitis and AIDS questions.” Memo from R Mouradian to J Ashworth 11 May 1983 p1 BAYP0004565. Though Hemofil was licensed by the FDA in March 1983, and Behringwerke was approved in Germany, neither product was licensed in the UK until 1984 (Behringwerke, a conditional licence) and February 1985 (Hemofil).
(1284) Minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 13 July 1983 p3 ARCH0001710
(1285) Letter from Dr Galbraith to Dr Ian Field 9 May 1983 pp1-4 CBLA0000043_040
(1286) Sir Joseph Smith Archer Inquiry Transcript 29 August 2007 p125 ARCH0000009
(1287) Written Statement of Sir Joseph Smith para 3.51 WITN5281001
(1288) Evidence of Professor Christopher Bartlett to the Archer Inquiry ARCH0001446
(1289) Professor Bartlett Archer Inquiry Transcript 30 August 2007 ARCH0000010
(1290) Professor Bartlett Archer Inquiry Transcript 30 August 2007 p3 ARCH0000010
(1291) Professor Bartlett Archer Inquiry Transcript 30 August 2007 p6 ARCH0000010
(1292) Professor Bartlett Archer Inquiry Transcript 30 August 2007 pp5-7 ARCH0000010
(1293) Professor Bartlett Archer Inquiry Transcript 30 August 2007 p22 ARCH0000010
(1294) Written Statement of Professor Stephen Palmer para 25.1 WITN7654001
(1295) Note from Thelma to AIDS Working Party 5 September 1983 p1 MRCO0000373_071
(1296) The Penrose Inquiry Final Report 1 March 2015 para 12.65 PRSE0007002
(1297) Council of Europe Recommendation R 83 8 23 June 1983 p3 MACK0000307
(1298) Note of Dr Tedder talk on sero-epidemiology of HTLV3 in the UK at the Cardiff Haemophilia meeting p1 PRSE0004532
(1299) Written Statement of Professor Richard Tedder para 440 WITN3436003
(1300) Professor Richard Tedder Transcript 13 October 2022 pp25-26 INQY1000255
(1301) Minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 21-22 July 1983 ARCH0001709
(1302) Professor Sir Michael Rawlins Transcript 7 June 2022 pp100-108 INQY1000211
(1303) Written Statement of Sir Joseph Smith para 3.16 WITN5281001
(1304) Lord Simon Glenarthur Transcript 22 July 2021 p172 INQY1000139
(1305) Lord Kenneth Clarke Transcript 27 July 2021 p156, p165 INQY1000141
(1306) And Hepatitis D.
(1307) There had already been an authoritative suggestion that importation of US concentrate should cease on the ground of the risk of hepatitis alone. Dr Smith had said as much in a minute which he sent to Dr Lane on 15 October 1980, when he interpreted graphs produced by Dr Craske as giving a good reason against continued importation. He discounted at least one of the arguments against this view – that most people with haemophilia already had been exposed to non-A non-B Hepatitis by receiving concentrate – on the basis that he would have thought one attack was better than two. Memo from Dr Smith to Dr Lane 15 October 1980 CBLA0001186
(1308) It is much less clear that it recognised the far greater risks of hepatitis arising from the use of large pool concentrate, especially that which was produced commercially, over and above the risks from using locally derived cryoprecipitate, as relevant to the question whether importation should be suspended. The likelihood is that this was regarded merely as an inherent risk of treatment, as it tended to be seen throughout the 1970s, without any significant thought as to whether increasing treatment by the use of cryoprecipitate (to reduce the risk of AIDS) would also help to reduce the long-term risks of non-A non-B Hepatitis. The fact that the suspension of imports would reduce the dual risks of these two significant adverse outcomes does not feature in the minutes.
(1309) In the minutes of the meeting.
(1310) It advised a hierarchy of safety. For young children, and those who were newly diagnosed with haemophilia, cryoprecipitate was to be used. Next, preference was to be given to NHS factor concentrate. The last resort was US-imported concentrate. Letter from Professor Bloom and Dr Rizza to Unknown 24 June 1983 HCDO0000270_004. This hierarchy was indeed that which Professor Bloom’s own centre at Cardiff had adopted, as shown in: Haemophilia Treatment Policy Guidelines 18 May 1983 pp1-2 WITN4029002
(1311) Or at least safer than factor concentrates, all things considered.
(1312) “Or” is used not only to reflect that hepatitis was also a risk of taking a blood product, but the argument by some at the time that people with haemophilia suffered from AIDS in consequence not because there was a causative virus but because of an overload of “foreign” protein, or of antigens, which itself would be a consequence of taking significant quantities of factor concentrate such as were taken in prophylactic home treatment. Indeed, this argument was that published by Sonnabend and others, which Dr Fowler personally thought the most convincing at the time.
(1313) In an article published in the British Journal of Haematology in 1977 Dr Biggs said: “Cryoprecipitate is a simple concentrate made from plasma at all Regional Transfusion Centres. Cryoprecipitate is much superior to plasma for the treatment of haemophilia A patients but the material is very variable from one sample to another and the potency cannot be known before it is used. For each dose the assumption must be made that the material is of low potency thus there is a tendency to use more material for each patient than is probably needed.” Biggs Haemophilia Treatment in the United Kingdom from 1969 to 1974 British Journal of Haematology 1977 p5 PRSE0004645
(1314) For those who suffered from inhibitor reactions to cryoprecipitate, NHS concentrate would have remained necessary if they were not to go untreated.
(1315) Minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 13 July 1983 p3 ARCH0002484
(1316) Minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 13 July 1983 p3 ARCH0002484
(1317) Letter by Professor Bloom written for publication to Haemophilia Society members 4 May 1983 DHSC0001228
(1318) Christopher Bishop Transcript 4 November 2021 p173 INQY1000158
(1319) Memo from Dr Foster to John Watt 13 July 1983 PRSE0002014
(1320) See the text above, setting out what was known of the possible cause(s) of AIDS in early 1983.
(1321) Letter from Dr Evatt to Professor Bloom 7 March 1983 p1 DHSC0001175
(1322) The point about the mismatch between the number of people with immunological abnormalities in at least two of the four groups identified as most at risk of AIDS (large), and the number of people diagnosed with the syndrome (small as yet), was already being said by the CDC in the Morbidity and Mortality Weekly Report for 4 March 1983 as suggesting that “the pool of persons potentially capable of transmitting an AIDS agent may be considerably larger than the presently known number of AIDS cases”. Centers for Disease Control Prevention of Acquired Immune Deficiency Syndrome (AIDS): Report of Inter-Agency Recommendations Morbidity and Mortality Weekly No8 4 March 1983p2 SBTS0003036_004
(1323) Letter from Dr Evatt to Professor Bloom 7 March 1983 p1 DHSC0001175
(1324) The history of AIDS, as was to be seen at the time, was typical of an infectious epidemic – low numbers, doubling over short periods, to become high figures over a number of months. Whatever was causing it was likely to have a similar pattern. Assuming an infectious cause, then if it took two years to show itself, from the first low numbers of infections, the likelihood was that cases of AIDS too would increase to a similar epidemic scale, just lagging two years behind the infections themselves. On these two assumptions – that it was infectious (ie probably a virus) and that (broadly) it took around two years to have such an effect on the immune system that AIDS was apparent – it was to be expected that the number of cases of AIDS would rise at an increasing pace from small beginnings. Both of the critical assumptions in this line of reasoning were the assumptions generally made at the time.
(1325) See also the information leaflet: Department of Health and Social Security AIDS and how it concerns blood donors National Blood Transfusion Service 1983 p2 BPLL0007247
(1326) It should also be noted that the argument in respect of the risk being low took only cases where the clinical diagnosis was already confirmed, thereby limiting any contribution of developing “pipeline symptoms” to the debate.
(1327) If the minutes of the AGM of the UKHCDO three months later are faithful to what was said, Professor Bloom’s apparent determination not to concede that concentrates might be the cause of AIDS is further demonstrated. They record (under “Any Other Business”) that Dr Morag Chisholm wondered if directors could revert to cryoprecipitate, given the “worry of patients” to which Professor Bloom responded that “he felt there was no need for patients to stop using the commercial concentrates because at present there was no proof that commercial concentrates were the cause of AIDS”. Quite apart from proof being well established by now on the balance of probabilities, looking for “proof” was to take the wrong approach. The question should have been whether there was a real risk. This was undeniable at the time: Minutes of UK Haemophilia Centre Directors meeting 17 October 1983 p10 PRSE0004440. Indeed, the DHSS and Central Office of Information prepared an information leaflet for donors in September in which it stated that Factor 8 was made from plasma obtained from many donors, and then: “Should just one of the donors be suffering from AIDS, then the Factor VIII could transmit the disease.” Department of Health and Social Security AIDS and how it concerns blood donors National Blood Transfusion Service 1983 BPLL0007247. As for Professor Bloom, a little over a year later he seems to have had a change of heart: the notes of a meeting on 10 December 1984 of representatives of the reference centre directors, BPL, DHSS, PHLS and Dr Tedder which was chaired by Professor Bloom record that he said “one has to accept, for the present, that it is difficult to avoid the argument that non-HT [non-heat-treated] constitutes a risk. There were problems in adopting a two-tier system of treatment.” Minutes of Haemophilia Reference Centre Directors meeting 10 December 1984 p7 HCDO0000394_117. By then, a substantial proportion of people with haemophilia were known to be seropositive, and heat treatment of factor concentrate was thought to reduce or eliminate the risk that those who were as yet uninfected would seroconvert. He now argued publicly and very strongly for steps to be taken to reduce or eliminate the risk, without any longer querying whether there was any risk worth bothering about, and without arguing (as was open to him) that there was yet no conclusive proof that heat treatment would necessarily be safe. It seems to be a case of his being too late in turning away from what Dr Colvin described in evidence as “wishful thinking”. Dr Brian Colvin Transcript 7 October 2020 p20 INQY1000062
(1328) Letter from David Watters to Paul Winstanley at the DHSS 17 May 1983 DHSC0003824_170
(1329) He was chair of the Medical Advisory Panel of the Haemophilia Society at the time.
(1330) Minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 13 July 1983 p4 ARCH0002484
(1331) Written Statement of Sir Joseph Smith paras 3.49-3.50 WITN5281001
(1332) Minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 13 July 1983 p4 ARCH0002484
(1333) They might arguably imply it since they suggest that self-sufficiency was highly desirable since it “should reduce risk appreciably”, thus linking the overall appreciation of risk with the potential development of self-sufficiency. The sooner self-sufficiency was achieved, the lesser the risk – if, however, the later it was, the greater the risk.
(1334) Albeit there might have had to be adjustments in the way in which plasma supplied went to BPL to provide for the continued production of albumins and immunoglobulins.
(1335) Minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 13 July 1983 p4 ARCH0002484
(1336) Compare, for instance, the views of CDSC directors with those of UKHCDO directors. See also the contemporaneous reference in a memo of 26 July 1983 from Mr J Parker, enclosing a “background note” prepared by Dr Walford in which she refers to “the cries from some quarters to ban the import of Factor VIII”. Memo from Mr J Parker to Mr Joyce 26 July 1983 p2 DHSC0002309_032
(1337) This, for instance, happened in the Netherlands where patients could continue after the start of 1983 to receive commercial concentrates provided there was written evidence of their consent. The Krever Report 1997 p923 KREV0000001
(1338) Professor Sir Michael Rawlins Transcript 7 June 2022 p110 INQY1000211. The whole exchange can be seen at: Professor Sir Michael Rawlins Transcript 7 June 2022 pp96-117 INQY1000211
(1339) To a meeting of the Blood Products Advisory Committee of the Center for Biologics Evaluations and Research, a standing committee which advised the US Secretary of Health (and the FDA). Minutes of Blood Products Advisory Committee meeting 19 July 1983 BAYP0004674. I deal further with this same evidence below.
(1340) He was speaking of contamination by an assumed infectious agent. See: The Krever Report 1997 p379 KREV0000001
(1341) Letter from A Barrell to Dr Walford 9 May 1983 p1 WITN4461116. This, suggests Dr Walford in her statement, was her earliest record of the FDA directive being referred to (despite Dr Fowler of the Medicines Division having been alert to it as early as 28 March 1983). Written Statement of Dr Diana Walford para 89.4 WITN4461001
(1342) David Watters wrote to the Medical Advisory Panel of the Society on 9 May 1983 to say that “a group of us” would be meeting him: Letter from David Watters to members of the Medical Advisory Panel 9 May 1983 BPLL0001351_076. An agenda for this meeting was put forward on 12 May 1983. Minutes of Haemophilia Society Executive Committee meeting 12 April 1983 pp2-3 HSOC0029476_024
(1343) Letter from Professor Bloom to K Fitch 23 May 1983 DHSC0001288. A reply (shared with DHSS) came on 8 June: Letter from K Fitch to Professor Bloom 8 June 1983 BPLL0001351_125. It is not straightforward. It reads: “First of all, I have to tell you that the Armour Pharmaceutical Company USA in anticipating the FDA ruling established the FDA protocols in compliance one month before the actual FDA recommendations were issued. For your further advice and assurance, you should know that we supplied Plasma prior to February 24 on a business-as-usual basis, but that most of this stock was supplied to customers in the USA, since 70% of our Plasma business is in the USA. At no time have we preferentially exported Plasma stocks ex the USA pre-February 24 or March 24.” On a careful reading this gives no reassurance at all about the future policy of Armour and as this chapter goes on to record, marketing by Armour of pre-March products is exactly what then occurred in the UK in and after August.
(1344) Although considering that Dr Galbraith’s recommendation was “premature” she wrote a memo on 16 May to Dr Fowler of the Medicines Division asking whether the supply of blood comprising pre-March plasma could be resisted: Memo from Dr Walford to Dr Fowler on Factor 8 and AIDS 16 May 1983 DHSC0001394
(1345) Memo from Dr Walford to Dr Fowler on Factor 8 and AIDS 16 May 1983 DHSC0001394, Memo from Dr Walford regarding an update on AIDS in people with haemophilia in UK 20 May 1983 DHSC0002227_060
(1346) The senior principal medical officer to whom Dr Walford reported.
(1347) It seems that there was already hesitation about maintaining an approach that there should be absolutely no dumping in the UK: an approach which regarded this as ideal rather than essential is one which contemplated that in reality it might not be achieved.
(1348) Letter from Dr Oliver to Mr Parker 17 May 1983 p1 DHSC0001395
(1349) Memo from Dr Fowler to Dr Walford 23 May 1982 p2 DHSC0002229_006
(1350) Of the Medicines Division.
(1351) Note on Acquired Immune Deficiency Syndrome (AIDS) meeting 3 June 1983 p1 WITN4461139. The nature of the “significant practical difficulties” is unclear. It is also unclear, in retrospect, why informal discussions should be contemplated as an alternative to legal restrictions, rather than as a precursor to them if those discussions did not produce a resolution satisfactory to the UK.
(1352) Note on Acquired Immune Deficiency Syndrome (AIDS) meeting 3 June 1983 p2 WITN4461139
(1353) Cutter Laboratories Inc later became a division of Miles Laboratories Inc.
(1354) Memo from C Wrigglesworth to others 28 June 1983 p1 DHSC0002229_055
(1355) Memo from Dr Oliver to Dr Walford 4 July 1983 DHSC0002229_062
(1356) Most probably 1 July 1983.
(1357) Memo from P Winstanley to Mrs Walden 28 June 1983 DHSC0002309_022, Memo from Dr Oliver to Mr Joyce 22 June 1983 DHSC0002309_123
(1358) Acquired Immune Deficiency Syndrome (AIDS) p3 DHSC0002309_124
(1359) Memo from Mr Parker to Mr Joyce 26 July 1983 p2 DHSC0002309_032. The letter was sent on 26 August 1983 and took a different line: “In March this year the US Food and Drug Administration initiated new Regulations for the collection of plasma, designed to exclude donors from high-risk groups. Although future supplies of Factor VIII both for export and for use in America will be manufactured from plasma collected in accordance with these Regulations, there is still a quantity of stock, some already in the UK and more in America awaiting shipment here, which has been made from ‘pre-March’ plasma. The FDA has recently decided not to ban the use of similar stocks intended for the USA market because to do so would cause a crisis of supply. The same considerations apply to the UK supply position.” Letter from Lord Glenarthur to Baroness Masham 30 August 1983 p2 DHSC0002231_037. This now contemplates that future supplies for the UK would not all be manufactured from pre-March plasma if those supplies had already been made and then stockpiled in the US awaiting shipment.
(1360) It thus promised more than the US firms had assured they would give.
(1361) Which it had the power to do.
(1362) Note the word, which tends to water down the effect.
(1363) Original emphasis. Minutes of Blood Products Advisory Committee meeting 19 July 1983 p3 BAYP0004674
(1364) Institute of Medicine Committee to Study HIV Transmission Through Blood and Blood Products HIV and the Blood Supply: An analysis of crisis decisionmaking 1995 p161 JREE0000019
(1365) Minutes of Blood Products Advisory Committee meeting 19 July 1983 BAYP0004674; see also Institute of Medicine Committee to Study HIV Transmission Through Blood and Blood Products HIV and the Blood Supply: An analysis of crisis decisionmaking 1995 pp161-166 onwards JREE0000019. Its analysis led to the following conclusion: “The Committee believes it is not possible to conclude that the FDA made a decision that was clearly in the interest of public health given available information as of July 19, 1983. A close reading of the data suggests that a policy, not only of automatic recall, but of delicensing AHF concentrate until further information was available concerning its role in the transmission of AIDS might have been justified on public health grounds. This would have included, of course, a recall of all stocks of AHF then on the market and withdrawal of all AHF concentrate in the inventory of producers. On the other hand, the Committee would like to reiterate that the facts clearly did not compel such an aggressive approach.” Emphasis added.
(1366) Memo from Dr Fowler to Dr Walford 28 July 1983 DHSC0002231_063. Though the memo is addressed to C Wrigglesworth of the Supplies Division.
(1367) Memo from C Wrigglesworth to Dr Walford 2 August 1983 DHSC0002231_014
(1368) Original emphasis. Memo from Dr Fowler to C Wriggleworth 3 August 1983 DHSC0002231_015
(1369) Memo from Dr Walford to C Wrigglesworth 3 August 1983 DHSC0002351_017
(1370) Memo from C Bishop to A Bessler 18 August 1983 ARMO0000287. Armour appears to have had no qualms internally about disposing of or selling pre-March 1983 product in the UK: Christopher Bishop Transcript 4 November 2021 p97 INQY1000158
(1371) Memo from C Wrigglesworth to Dr Walford August 1983 DHSC0002351_018
(1372) Letter from Lord Glenarthur to Reverend Tanner 28 September 1983 p1 HSOC0008598_035
(1373) Letter from Lord Glenarthur to Clive Jenkins 26 August 1983 p1 DHSC0002231_036. Emphasis added.
(1374) The tension is increased by the fact that only two days earlier the MRC had issued a brief on AIDS saying: “Over the last six months the possibility of transmission by blood transfusion has become increasingly apparent with the description of AIDS in an infant who received platelets from an adult who later developed the disease … An infectious agent has therefore been implicated which is sexually, parenterally and even perinatally transmitted with a long asymptomatic infectious incubation period varying from months in infants to two years in adults.” Extract of Appendix from MRC brief on AIDS 24 August 1983 DHSC0002231_031
(1375) Memo from Robin Maysmith to Mr Winstanley 26 August 1983 p2 DHSC0002309_034
(1376) Memo from Robin Maysmith to Mr Winstanley 26 August 1983 DHSC0002309_034. The Press Statement finally released contained no reference to the special requirements introduced by the FDA, but when sent to editors for release in the press was accompanied by a “Note to Editors” which repeated the wording. Department of Health and Social Security Press Release AIDS - and Blood Donation 1 September 1983 DHSC0006401_006
(1377) Lord Glenarthur Transcript 23 July 2021 pp7-84 INQY1000140
(1378) Lord Glenarthur Transcript 23 July 2021 p83 INQY1000140. Although it could be said that ministers should have been more questioning of their officials, and that here Lord Glenarthur was not being sufficiently challenging, I do not criticise him for taking on trust what his officials were saying on this occasion. However, those who drafted the letter should have ensured it was suitably qualified. They could, and should, have required pharmaceutical companies to adjust the labelling requirements to show the date of collection of the plasma from which the product was made, so that haemophilia centre clinicians could have been alert and put in a position where they could inform their patients of the choices they had as to product, and the particular risks of the pre-March plasma product they were being offered (when and if they were).
(1379) Armour seems to have thought it was decided at a meeting attended by Professor Bloom: Memo from C Bishop to A Bessler 18 August 1983 ARMO0000287. If so, no written record survives.
(1380) This was the approach: what seems to have been lost sight of is that the Licensing Authority was the Minister (acting together with his counterparts in Scotland, Northern Ireland and Wales) as set out above, and (again as set out at the start of this chapter) ministerial authority was in practice delegated to the Department. The CSM advised the Department; it was for the Department to accept or reject that advice. Here the Department seems instead to have ceded its authority to the CSM, and then had to interpret what was being said to it without asking Dr Smith for clarification.
(1381) Inquiries were – rightly – made by Dr Walford on 16 May 1983 to seek to know if available post-March products together with non-US imports might be sufficient. Memo from Dr Walford to Dr Fowler on Factor 8 and AIDS 16 May 1983 DHSC0001394. Dr Fowler said a week later that neither Immuno “nor the other European manufacturers could have any chance at all” (of producing enough to fill the gap left). Memo from Dr Fowler to Dr Walford 23 May 1982 p2 DHSC0002229_006
(1382) And the place: knowing where any infections might have come from if a particular batch of product was implicated in them might be critical in protecting future recipients of product, and would permit the pharmaceutical company concerned to eliminate any implicated individual source from future collection schedules; it might also be important to enable a check to be made by UK regulators to see if the collection practices at that location were indeed as recommended by the FDA.
(1383) Memo from K Egerton to Dr Walford 7 September 1983 p2 DHSC0002231_052. The author however commented that they were however “unhappy about the return from Miles”. 70% of the Armour and 68% of the Alpha stock had been collected in this way, leaving therefore around 30% which had not been. “Special precautions” are a reference to some of the measures which companies had variously taken before March 1983 in response to what they recognised as a risk that the cause of AIDS might be transmitted by blood products.
(1384) To a meeting of the Blood Products Advisory Committee of the Center for Biologics Evaluations and Research, a standing committee which advised the US Secretary of Health (and the FDA): Minutes of Blood Products Advisory Committee meeting 19 July 1983 p3, BAYP0004674
(1385) He was speaking of contamination by an assumed infectious agent. The Krever Report 1997 p379 KREV0000001
(1386) Minutes of Blood Products Advisory Committee meeting 19 July 1983 p3 BAYP0004674
(1387) Letter from Lord Glenarthur to Clive Jenkins 26 August 1983 DHSC0002231_036
(1388) Dr Fowler sent a memo to Mr Wrigglesworth on 28 July, very shortly after the FDA meeting, which infers he looked at the discussions with some detail: “It lasted four and a half hours … Although the subject got a very thorough airing nothing new came to light. The possibility of banning all products made before the implementation of the March ‘83 regulations was discussed but was rejected on a majority vote. The hiatus in supplies which such action would cause was the deciding factor.” Memo from Dr Fowler to C Wriggleworth 28 July 1983 DHSC0002231_063
(1389) Though, as noted in the preceding footnote, Dr Fowler appears to have considered it.
(1390) This assumes they had the detail at least as set out in the text: but as pointed out, it is unclear that DHSS had been given it.
(1391) See the reference to the discussion between Dr Walford and Dr Fowler set out at the start of this section.
(1392) Note of Acquired Immune Deficiency Syndrome meeting 3 June 1983 p1 WITN4461139
(1393) Whether this would actually have resulted in a change of practice, or in patients being told, would very much depend upon the attitudes and practice of the doctor concerned. The chapter on Haemophilia Centres: Policies and Practice may give little ground for confidence in many cases: but they should at least have been put into the position of being able to do so, and this does not detract from the principle that the DHSS should have done as it ought to have done.
(1394) For fairness, it should be pointed out that this was in response to the assertion by Counsel to the Inquiry that there was no evidence of any such review. It seems clear Professor Sir Michael Rawlins did not know of any either: but his answer was on the basis there was none.
(1395) Immuno Ltd application Tissel Kit product licence 11 May 1983 MHRA0033335_039
(1396) Hoechst UK Ltd application Serum Cholinesterase product licence 12 January 1983 p2 DHSC0003948_039
(1397) Inferentially, safer ones.
(1398) Especially non-A non-B Hepatitis.
(1399) Berntorp et al A systematic overview of the first pasteurised VWF/FVIII medicinal product, Haemate P/Humate-P: History and clinical performance European Journal of Haematology 2008 p8 JREE0000008
(1400) Letter from P Taub to H Terreer 2 February 1979 CGRA0000218
(1401) Letter from L Kriley to G Phelps 22 May 1979 CGRA0000219, Memo from L Kriley to Distribution 14 June 1979 CGRA0000220
(1402) Cutter had itself conducted experiments in 1972, which had some promising results but were taken no further at the time, and began further experiments in 1978. See chapter Viral Inactivation.
(1403) Baxter, for Hemofil-T; Alpha in December 1982 for Profilate; and Armour in December 1982 for Factorate. Institute of Medicine Committee to Study HIV Transmission Through Blood and Blood Products HIV and the Blood Supply: An analysis of crisis decisionmaking 1995 p106 JREE0000019
(1404) Cutter – the application being made in the name of Miles Laboratories Ltd in August 1983 for pasteurisation product: Miles Laboratories Ltd Antihaemophilic Factor (Human) Koate product licence 16 August 1983 BAYP0000002_196; and in November 1983 for a dry-heated product: Miles Laboratories Ltd Dired Factor VIII Fraction Koate product licence application November 1983 BAYP0000002_206
(1405) Institute of Medicine Committee to Study HIV Transmission Through Blood and Blood Products HIV and the Blood Supply: An analysis of crisis decisionmaking 1995 p106 JREE0000019
(1406) May 1983: Hemofil-T; July 1983: Behringwerke: “Haemate P”; Factorate: February 1984. Counsel Presentation on Overview Chronology of the Licensing of Commercial Blood Products in the United Kingdom during the 1970s and 1980s 6 December 2022 pp23-24 INQY0000411
(1407) In September 1983 for Hemofil-T; in July 1984 in respect of Factorate.
(1408) Travenol Laboratories Ltd Hemofil product licence variation 14 September 1983 DHSC0003951_006
(1409) Dr Purves.
(1410) Travenol Laboratories Ltd Hemofil product licence variation May 1983 p5 DHSC0105556_028. “Confirm” is a form of wording which adopts a similar approach to that which the phrase “no conclusive proof” adopts. If not to “confirm” it there was, certainly, evidence at least to support it. It is an approach which by seeking certainty takes insufficient account of risk. The assessor may have been pharmaceutical but nonetheless expressed a view about the then state of knowledge about the cause of AIDS which they ought to have known was incomplete and risked being wrong.
(1411) Dr Fowler.
(1412) Travenol Laboratories Ltd Hemofil product licence variation May 1983 p7 DHSC0105556_028. As a matter of fact Hyland/Travenol had written to haemophilia centre directors and to the DHSS to say that it could not give an assurance that the heat-treated product eliminated the risk of transmission to AIDS since the causative agent for AIDS had not been identified, but it “believes that administration of the heat treated product, designed to reduce active viral content, may increase patient and centre personnel safety … Travenol Laboratories believes that the above steps represent the most responsible action that can be taken at this time to assure a continued safe supply of coagulation factor concentrate to the Haemophiliac population.” Letter from A Barrell to Professor Bloom 9 May 1983 p2 DHSC0001291
(1413) The likelihood is that this is because the Committee was influenced by the pharmaceutical assessor, who was concerned that a dry heat technique was considerably less effective than a wet heat (pasteurisation) method: in view of the risk that a virus might be killed if on the surface of the product, but protected against this if surrounded by protein. It was thought the heat-treatment step should be justified. Indeed, the product was refused a licence on all three bases: safety, quality and efficacy. Travenol Laboratories Ltd Hemofil product licence variation 14 September 1983 DHSC0003951_006
(1414) Travenol Laboratories Ltd application for Antihaemophilic Factor (Human) Method Four-Heat Treated Hemofil-T product licence 30 November 1984 p17 SHPL0000283_005. However, this did not and does not mean that the UK Licensing Authority should not reach its own independent judgement: its doing so is an important aspect of UK health protection.
(1415) Hoechst UK Ltd application for heat-treated Haemate P Factor VIII product licence 22-23 March 1983 p56 MHRA0000090
(1416) Hoechst UK Ltd application medical assessment for heat-treated Haemate P Factor VIII product licence p85, p89 MHRA0000090
(1417) Letter from Pat Turner of Hoechst UK Ltd to Dr Thomas 23 February 1987 p43 MHRA0000090
(1418) Armour Pharmaceutical application for Heat Treated High Potency Factorate product licence declined 27 July 1984 p64 MHRA0000088
(1419) Centers for Disease Control Update: Acquired Immunodeficiency Syndrome (AIDS) in Persons with Hemophilia Morbidity and Mortality Weekly Report No42 26 October 1984 CBLA0001909
(1420) Minutes of Committee on Safety of Medicines Sub-Committee on Biological Products meeting 7 November 1984 p3 DHSC0105559_002, Minutes of Committee on Safety of Medicines meeting 22 November 1984 p6 WITN5281034
(1421) Of course, the CSM’s formal role was advisory. It had no power in itself to grant a licence. That was for the ministers who constituted the Licensing Authority (see text at the start of this chapter). So Dr Smith could not act on his own initiative. There had to be a recommendation by the CSM followed by a decision by the Licensing Authority in order for the invitation to be given. Such a division of function might normally result in some delay. It makes the speed of response all the more remarkable, but leaves one wondering why the DHSS (as, in effect, the Licensing Authority) did not itself initiate the process earlier. Given that the issue concerned risk to life, a better response to the CDC report might have been for the DHSS to have invited applications in late October and to have consulted the CSM(B) on the appropriate way to handle them most speedily.
(1422) Minutes of Committee on Safety of Medicines meeting 22 November 1984 p6 WITN5281034
(1423) Letter from M Duncan to Mr Nicholson 26 November 1984 SHPL0000067_028
(1424) Memo from Jack Wood to Distribution pp3-4 BAYP0000025_087
(1425) Counsel Presentation on Overview Chronology of the Licensing of Commercial Blood Products in the United Kingdom during the 1970s and 1980s 6 December 2022 pp29-30 INQY0000411
(1426) The Safety of Heat Treated Factor VIII 4 March 1986 p4 WITN5281049
(1427) It is a reasonable inference that when Behringwerke’s application was granted, it had supplied the necessary information and detail not simply on safety but in respect of quality and efficacy. It is also the case that when licensing the Behringwerke product the Committee had required it to make no claim that the treatment eradicated the virus. It was plainly cautious about claims for viral reduction.
(1428) If it felt unable, as a body focused on safety, to rely on its implicit understanding of the reason for the heat treatment and deal with the application on that basis, whilst being given the additional information it had lacked on the efficacy of the heat treatment applied.
(1429) Travenol Laboratories Ltd Hemofil product licence variation May 1983 p7 DHSC0105556_028
(1430) It is fair to point out that the Behringwerke product used a wet-heat process, so it cannot be regarded as exactly comparable.
(1431) Some period for consideration is necessary, given that any product has a potential to cause undesirable side effects which have to be guarded against. It must however not be too long in a context such as this. A month is not unreasonable.
(1432) Immuno Ltd Kryobulin product licence alteration 12 December 1984 MHRA0033320_066
(1433) Of its nature it is a reference resource for many, rather than required reading.
(1434) The Control of Medicines in the United Kingdom July 1977 p16 MHRA0004773
(1435) The Control of Medicines in the United Kingdom July 1977 p16 MHRA0004773
(1436) The Control of Medicines in the United Kingdom July 1977 p17 MHRA0004773
(1437) Dr Frances Rotblat of the DHSS is reported also to have told Cutter that “it is extremely rare for the yellow card system to be used for this [hepatitis in blood products] because haemophilia centres have their own computerised surveillance unit based in Oxford. The vast majority of physicians treating haemophiliacs report any occurrences to this centre rather than to the CSM.” Note of telephone conversation between J Boult and Dr Rotblat 18 May 1988 p2 WITN6984035
(1438) Acute refers to symptoms within a period of six months from the causative transfusion or infusion or injection, whereas “chronic” means symptoms arising after that initial period of six months.
(1439) Written Statement of Anne Ryan para 3.3 WITN7183001
(1440) A very small number when compared with the total number of reports for that period, which was 310,042. Table showing All UK spontaneous suspected Adverse Drug Reaction (ADR) reports received by the MHRA between 1970 to 1995 16 February 2022 WITN6406025
(1441) These are lay terms to simplify the wording of the classifications by which adverse reactions were grouped: the relevant ones being “Blood and lymphatic system disorders, Hepatobiliary disorders, Infections and infestations, Investigations”. Table showing All UK spontaneous suspected Adverse Drug Reaction (ADR) reports received by the MHRA between 1970 to 1995 16 February 2022 WITN7183005
(1442) It was described, in relation to a drug which has no relation to the Terms of Reference of the Inquiry, by Professor Adolf Asscher in an affidavit of January 1989 which formed part of the evidence before the court in an application for judicial review at the time: Statement made by A W A Asscher regarding the adverse drug reporting scheme 27 January 1989 WITN6406024
(1443) The policy lead in the Regulatory Reform Team in the MHRA’s Partnership Division liaised with colleagues with relevant knowledge and experience to collate any information. The files are partially incomplete, however. Written Statement of Anne Ryan para 1.5 WITN7183001
(1444) The addendum of British Pharmacopoeia from 1973 to 1991 contains no reference to the risks of HIV/AIDS: British Pharmacopoeia addendum definitions of Dried Human Antihaemophilic Fraction/Dried Factor VIII Fraction 1973-1991 pp9-10 SBTS0002189. Discussed in the evidence of: Dr Robert Perry Transcript 1 April 2022 pp24-29 INQY1000184. It is right to acknowledge that, so far as people with bleeding disorders were concerned, there was a reporting system operated by most clinicians engaged in haemophilia care, where a computerised system was kept by UKHCDO; but this did not cover reports of infection following transfusion. It was not designed to fulfil a function similar to that which the Yellow Card scheme did. It is also right to acknowledge that information was relayed to the CDSC – though some of the weaknesses of the completeness of reporting are apparent from the fact that a patient with AIDS symptoms in Bristol in early 1983 was not notified to the CDSC until after his death later that summer.
(1445) Safer – which does not mean to say safe, as experience in Edinburgh with HIV infections in 1984 was later to show.
(1446) Though in the case of Hepatitis C much would probably have depended upon the pool size used.
(1447) Dr Cumming was the regional transfusion director for Edinburgh and South East Scotland. He was also one of the first three Scottish blood donors to reach 200 donations (in 1976), not only being a professional advocate for plasmapheresis but practising what he preached. History of Blood Transfusion p3 SBTS0000286_099. Dr Maycock oversaw the fractionation plants in England and was also consultant advisor to the Chief Medical Officer in respect of blood transfusion.
(1448) The Voluntary Blood Donor p7 SBTS0000605_005. Emphasis in the original. This, interestingly, is echoed (though not cited) in a paper by Dr Antonio Fernández-Montoya Altruism and payment in blood donation as the abstract makes clear: “This paper argues that blood donation is an example of genuine altruism where the altruistic behaviour is incorporated into the self as a role. Unpaid donation is proven to be much safer for receivers, and supply problems can be attributed fundamentally to inefficiencies in the organization of transfusion services. Voluntary and non-remunerated donation may be sufficient for a country/region to cover all its blood product needs, but requires an efficient organization and the elimination of ‘spurious altruism’, non-monetary forms of compensation that harm the social image of voluntary donation and obstruct its further development.” Fernández-Montoya Altruism and Payment in Blood Donation Transfusion Science 1997 p1 DHSC0004571_082. Ironically – and misleadingly – the Department of Health relied on this article by Dr Fernádez-Montoya in its 2006 report on self-sufficiency for the conclusion that: “It is now known that it is an indisputable reality that very few countries are capable of completely satisfying their blood needs (i.e. becoming self-sufficient) without acquiring a proportion of blood from paid donors.” Self-Sufficiency in Blood Products in England and Wales: A Chronology from 1973 to 1991 2006 pp30-31 DHSC0200111. On any fair reading of this article the author was saying precisely the opposite. In short, the article made exactly the same point in 1997 as Dr Cumming did in 1975.
(1449) He also said, in 1967, that: “I am sure that there is really no valid reason for a shortage of ‘coagulation factor’ products for therapy in this country and recent results from frozen plasma for producing a concentrate, make me more than ever convinced that cryoprecipitate will probably have a minor role and that centralised production by other methods will be perfectly feasable [sic].” Letter from Dr Cumming to Dr Rosemary Biggs 14 December 1967 OXUH0003778_008
(1450) This is no longer as true as it was before the mid 1990s. Some blood products were made by BPL not only for domestic consumption but for supply overseas. Some profit was realised from this for what became in due course a private company.
(1451) Under the Medicines Act 1968 section 9(1)(a) individual clinicians could obtain and import an as yet unlicensed product on a “named person” basis where it was intended for use by a specific patient. This is how the first commercial products gained entry to the UK, possibly in the late 1960s but if not then, certainly in the early 1970s.
(1452) Arrangements changed in the mid 1970s – see for instance a circular directed towards Health Authorities performing such tasks as producing cryoprecipitate. Circular from DHSS to Regional Health Authorities and others May 1975 CBLA0000001_038
(1453) A graphic illustration of this is a mother’s memory of a set of white leather suitcases seen at Birmingham Children’s Hospital as a gift, which were understood to be from a pharmaceutical company. Written Statement of Elisabeth Buggins para 59 WITN1021001
(1454) Plasma for US manufacture was from time to time derived from certain African countries (such as Lesotho), from South and Central America (such as Belize and Mexico), and the Caribbean (notably Haiti). A statement offered to the Inquiry from an investigative reporter investigating Belize’s trade in plasma to the US describes how a visitor to his motel room told him to take the first plane out the following morning. The reporter took this as a warning and left the next day. Written Statement of Edward Harriman para 19 WITN0696001. It can be inferred that the quality of the product was dubious, or the donors exploited (or both), and that it was being collected to make substantial profits.
(1455) Immuno at one stage marketed products with different coloured labels to denote whether the raw material was plasma from a plasma broker in the US or elsewhere (cheaper), or came from European sources (more expensive). A body of material accumulating from the mid 1960s onwards evidenced that commercial product manufactured in the US (where it was understood there was a higher rate of endemic hepatitis) was at least 5 times, and could be as much as 20 times, more likely to transmit infection: the underlying assumption behind Immuno’s pricing structure appeared to UK haemophilia clinicians to be that the European-sourced plasma was more expensive because it was less likely to be infective and that this would be of such value to the likely purchasers that they would pay the premium. Or that the new product, being from cheaper US plasma, would be cheaper, and thus command a greater share of the market for those purchasers more concerned with price than safety. See the chapter on Regulation of Commercial Factor Concentrates.
(1456) This is so where donors are not screened, donations are untested, and where the pool as a whole is not subjected to a process which inactivates the virus. For much of the period central to the Inquiry donations were untested (there was no test which would directly identify the virus for HIV until late 1984 at the earliest, and until 1989 for non-A non-B Hepatitis (Hepatitis C); there were tests for Hepatitis B from 1972 onwards but they were imprecise, and improved only slowly until by the early 1980s they became more or less reliable (see the chapter on Hepatitis Risks 1970 and After); there was no viral inactivation until heat treatments developed in the late 1970s and early 1980s, and these were initially only partially effective for non-A non-B Hepatitis though proved generally effective for HIV with one or two notable exceptions. (See the chapter on Viral Inactivation). Donor selection was less effective amongst commercial producers – one or more took from high-risk penal institutions in the US, and for a while from the Caribbean, Central America, or further afield – than in the UK, and although donors were screened to an extent in both systems there is room to doubt that it was as effective in the US as it was in the UK. That is despite the fact that in the UK it was often rudimentary.
(1457) Cohn et al Preparation and Properties of Serum and Plasma Proteins. IV. A System for the Separation into Fractions of the Protein and Lipoprotein Components of Biological Tissues and Fluids Journal of the American Chemical Society March 1946 PRSE0002176
(1458) Dr Ralph Kekwick (England), Dr Margareta Blombäck (Sweden) and Dr Jean-Pierre Soulier (France). Wellcome Witnesses to Twentieth Century Medicine – Haemophilia: Recent History of Clinical Management September 1999 p17 RLIT0000022. Also Dr Drummond Ellis in Scotland.
(1459) Antihaemophilic Fraction 27 April 1954 p1 SCGV0001182_190. It stated that it was obtained by the ethanol fractionation method of Dr Cohn, and had been prepared from 15 donor pools of plasma from selected donors who had no history of clinical jaundice. Dr Ellis and others later described how experimental quantities were made between 1952 and 1956 and then its manufacture was developed. By 1960 they were fractionating plasma from 1,425 donors and started investigating red cell concentrates to make full use of the donated blood. Cumming et al Red Cell Banking and the Production of a Factor VIII Concentrate Vox Sanguinis 1965 p1 PRSE0003381
(1460) Drs Kekwick and Wolf reported that they had developed antihaemophilic fraction (“AHF”) which had been used with success in six cases. “AHF” represented that fraction of blood which would enable clotting, and hence be “anti” haemophilic. Kekwick and Wolf A Concentrate of Human Antihaemophilic Factor - its use in six cases of haemophilia The Lancet 30 March 1957 RLIT0000043_013
(1461) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine Vol 6 1996 p51 NHBT0000028. This was similar to the Swedish achievement by Drs Birger and Blömback, whose product had treated 59 patients by 1959. Nilsson et al The Use of Human Anti-haemophilic Globulin (Fraction I-O) in Haemophilia A and in von Willebrand’s Disease Acta Haematologica 1960 RSME0000078
(1462) Report to Advisory Sub-Committee on Blood Products and Blood Group Reference Laboratories 8 September 1978 p11 CBLA0000840, Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine Vol 6 1996 p48 NHBT0000028. A principal reason for this was that large Pool sizes were regarded as unsafe because the risks of any part of a pool formed transmitting hepatitis became too high: a World Health Organization Expert Committee had, for instance, advised against their use in 1952 (see the chapter on ‘Pool Sizes). Dr Maycock in 1964 took the view that pools for fractionation should be maintained at their then present pool size (30 litres, or approximately 150-180 donors) rather than changed to a larger size, by inference regarded as more convenient for fractionating larger quantities. Minutes of Working Party on Human AHG meeting 16 March 1964 p8 BPLL0003647
(1463) Report to Advisory Sub-Committee on Blood Products and Blood Group Reference Laboratories 8 September 1978 p11 CBLA0000840. Dr Maycock was superintendent of the Lister Institute’s laboratory in Elstree and then director of BPL 1949-78.
(1464) Report to Advisory Sub-Committee on Blood Products and Blood Group Reference Laboratories 8 September 1978 p11 CBLA0000840, Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine Vol 6 1996 p50 NHBT0000028, Minutes of Joint Steering Committee on Blood Products Production meeting 20 June 1973 p1 PRSE0004359
(1465) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine Vol 6 1996 p58 NHBT0000028
(1466) Report to Advisory Sub-Committee on Blood Products and Blood Group Reference Laboratories 8 September 1978 p11 CBLA0000840
(1467) To whom he reported as consultant adviser on blood transfusion. Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine Vol 6 1996 p48 NHBT0000028. The Medical Research Council (“MRC”) had also foreseen a need for improved production facilities. On 26 June 1957, following the developments by Drs Kekwick and Wolf, it updated the then CMO, Sir John Charles: “Both the Haemophilia Committee and the Sub-Committee consider this human preparation to be a most important advance in the treatment of haemophilia and are anxious that everything possible should be done to facilitate its manufacture in larger quantities so that a more extensive clinical trial can be made. We should accordingly be very grateful for any assistance you may be able to give in furthering this matter.” Letter from the MRC to Sir John Charles 26 June 1957 p2 DHSC0103048_012. Dr Charles was succeeded as CMO by Dr George Godber in 1960.
(1468) Report to Advisory Sub-Committee on Blood Products and Blood Group Reference Laboratories 8 September 1978 p11 CBLA0000840
(1469) Not limited to coagulation factor concentrates such as Factors 8 and 9: albumin, immunoglobulins, and other fractionated proteins, were all to be produced.
(1470) Minutes of Regional Blood Transfusion Centre meeting 9 May 1968 p4 SBTS0000470_105. A litre contained the plasma from approximately five donations of blood.
(1471) In early documents it is often labelled “HAHG”, for “human anti-haemophilic globulin”, to distinguish it from AHG produced from cows, pigs or sheep. Biggs and Macfarlane Treatment of Haemophilia and other Coagulation Disorders 1966 p67 RSME0000009
(1472) Protein Fractionation Centre Liberton and the Arrangements with the NBTS p1 DHSC0003715_171
(1473) Protein Fractionation Centre Liberton and the Arrangements with the NBTS p1 DHSC0003715_171
(1474) It may owe much to Dr Cumming’s enthusiasm and activism. See for example his minute covering the annual report for 1963: “I would like to repeat what I have said frequently – that the time has come to reassess the whole question of the provision, handling and use of blood, and that a large sum of money laid aside specifically for the pursuit and development of this aim should be considered as a priority.” Letter from Dr Cumming to Dr R Gordon 15 November 1963 p2 SCGV0001192_064. 15 months later, Dr Gordon of the SHHD visited Dr Maycock to “discuss the part which the Blood Products Unit in Edinburgh should play in the production of part of the requirement of plasma fractions in England and Wales” prior to reaching an agreement with the DHSS. Letter from Scottish Home and Health Department to Dr Maycock 4 February 1965 SBTS0000284_060. The same energy and enthusiasm for catering for the future does not seem to have followed in the 1970s.
(1475) This development was reported by Dr Judith Pool in 1965. Pool Production of High-Potency Concentrates of Antihemophilic Globulin in a Closed-Bag System The New England Journal of Medicine 30 December 1965 PRSE0000314
(1476) A paper produced for the Working Party by Dr Maycock and Leon Vallet dated February 1964 concluded that 35,000 donations (one donation per bottle) would be needed. It suggested that collecting blood in plastic equipment of “Fenwal” type would permit aseptic separation of red cells and plasma and immediate rapid freezing of the plasma, which could then be stored until thawed for fractionation. As to where the preparation of AHG should take place, the rival merits of central preparation, or dividing the task between BPL and a small number of selected laboratories, or between BPL and a large number of peripheral laboratories, were debated. Minutes of Working Party on Human AHG meeting 16 March 1964 p3 DHSC0100006_100. Of additional interest is the paper’s view that it would be preferable to retain a pool size of 30 litres (approximately 150-180 donors) “because of the risk of transmitting serum hepatitis.” Minutes of Working Party on Human AHG meeting 16 March 1964 p4 DHSC0100006_100
(1477) Minutes of Working Party on Human AHG meeting 16 March 1964 BPLL0003647. The paper was to be sent by the MRC to the Ministry of Health.
(1478) Formerly known as the Blood Products Unit, and formerly located in the Royal Infirmary of Edinburgh. Liberton was a new site without the constraints of space.
(1479) “AHG” and “AHF” are used interchangeably throughout the early history of concentrate production and haemophilia treatment.
(1480) Cumming et al Red Cell Banking and the Production of a Factor VIII Concentrate Vox Sanguinis 1965 p3, p9 PRSE0003381
(1481) If plasma is frozen and then slowly thawed under controlled conditions it will leave a sludge or precipitate. It is this which is “cryoprecipitate”. It forms the basis for all manufacture of factor concentrates from human sources.
(1482) Bennett et al Cryoprecipitate and the Plastic Blood-bag system: Provision of Adequate Replacement Therapy for Routine Treatment of Haemophilia British Medical Journal 8 April 1967 p4 RLIT0000682. It added that a changeover on a national scale from glass bottles to the closed plastic bag system offered a solution to the “problem of providing adequate therapeutic material for the treatment of haemophilia”. This is because the method for producing cryoprecipitate in a sterile manner was by use of bags in which the sludge left after the first stage of fractionation could be collected, the bag sealed, and the whole of it then fast frozen, presenting a loss of significant Factor 8 activity. Plastic bags were increasingly used, though they were yet to become emblematic in media portrayals of blood transfusions as they are today.
(1483) Letter from Dr Jones to the editor of The Lancet 8 April 1967 p1 PJON0000136_001. Dr Jones was the director of the Newcastle Haemophilia Centre.
(1484) ie at regional transfusion centres.
(1485) Cryoprecipitate could contain a greater range of proteins which the body recognised as “foreign”, though the risk of immune reactions was quite often controlled by the prophylactic use of Piriton or other antihistamines.
(1486) They were physically close to each other, forming what was referred to in evidence by Dr James Smith as a “Virtuous Triangle” (he had in mind PFL, the haemophilia centre, and the wider hospital services): “The Oxford HC [Haemophilia Centre] in Church Hospital treated many more patients than average, partly because families with haemophilia migrated to the Centre which, under Dr. [Robert] McFarlane and Dr. [Rosemary] Biggs, had always offered more generous treatment from the beginning. Partly, too, because it attracted some of the hardest cases, often from farther afield, including those needing innovative surgery – also carried out in Churchill Hospital ... About 50m from the HC, and working under the most trying conditions, Dr. Grant and later Dr. Gunson at Oxford RTC made heroic efforts to provide the fresh plasma for PFL’s production of F.VIII, all of which went next door to the HC. I was never given a convincing technical reason why, with BPL playing the role of the PFL in the Virtuous Triangle, the same could not have been done in every Region, long before the surge in about 1982.” Written Statement of Dr James Smith para 165 WITN3433001
(1487) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine Vol 6 1996 p52 NHBT0000028. This is a retrospective review, so the authors may be excused for some inaccuracy of dating. They have ascribed the significant discovery which was the preparation of cryoprecipitate by Dr Pool as having happened in 1970, whereas it was actually five years earlier. There is no reason to disbelieve the other dates set out in their text, but given this substantial error of retrospective dating the other dates they quote should be approached with appropriate caution.
(1488) The one other notable exception to that was at a time when heat-treated Factor 9 concentrates first became available, in 1985. Counsel Presentation Note on the Use of Factor IX Concentrates for the Treatment of People with Haemophilia B January 2023 pp2-12 INQY0000443. For a detailed account of what happened in response to vCJD so far as blood products were concerned, see the chapter on vCJD.
(1489) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine Vol 6 1996 p52 NHBT0000028
(1490) Dr Katharine Dormandy at the Royal Free Hospital was an enthusiast for home therapy with cryoprecipitate, but it required deep freeze facilities which were not as commonplace then as they are today. A number of centres provided it. Wellcome Witnesses to Twentieth Century Medicine – Haemophilia: Recent History of Clinical Management 1999 pp45-48 RLIT0000022
(1491) Preparations had been based on the method of Blömback between 1968 and 1972. The method of Newman (1971) allowed for greater specificity, and improved solubility. Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine Vol 6 1996 p52 NHBT0000028, Newman et al Methods for the Production of Clinically Effective Intermediate and High-purity Factor VIII Concentrates British Journal of Haematology 1971 PRSE0000461. At the same time, there was a change from the use of ether to the use of ethanol. Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine Vol 6 1996 pp50-51 NHBT0000028. Ether had been substituted for ethanol in the original method of Cohn fractionation, because ether had been more readily available. Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine Vol 6 1996 p47 NHBT0000028. An advantage of ethanol was that being an alcohol, its sterilising effects ensured a greater freedom from biological contaminants.
(1492) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine Vol 6 1996 p52 NHBT0000028
(1493) Minutes of Working Party on Human AHG meeting 16 March 1964 p2 BPLL0003647. Amongst English centres, Oxford was known to provide a greater quantity of clotting factors than most if not all of the other centres at the time. Biggs Jaundice and Antibodies Directed against Factors VIII and IX in Patients Treated for Haemophilia or Christmas Disease in the United Kingdom British Journal of Haemotology 1974 p8 HCDO0000581. Note that the estimates by the working party mentioned earlier in the chapter had been for 35,000 donors only a couple of years earlier and with no particular development in the meantime: this was suggestive of increasing demand for concentrate as opposed to cryoprecipitate.
(1494) Letter from Dr Biggs to Sir George Godber 22 August 1967 DHSC0100025_062
(1495) This represented a first clarion call for the UK to become self-sufficient in the production of factor concentrates. Letter from Dr Biggs to Sir George Godber 22 August 1967 DHSC0100025_062
(1496) PFC first produced factor concentrates in January 1975, and reached full capability using “9 to 5” production in 1976. Counsel Presentation Note on Self-sufficiency and Domestic Production of Blood Products in Scotland and for Northern Ireland March 2022 pp10-11 INQY0000343. It was never utilised fully on a 24-hour shift pattern, for reasons which are explored below.
(1497) By contrast with Edinburgh, BPL was not originally intended to accommodate means for fractionating of plasma nor, as first planned, was its extension. See the text above for Dr Maycock’s scathing views of the overall suitability of the plant even after the extension.
(1498) Report to Advisory Sub-Committee on Blood Products and Blood Group Reference Laboratories 8 September 1978 p11 CBLA0000840
(1499) Report to Advisory Sub-Committee on Blood Products and Blood Group Reference Laboratories 8 September 1978 p11 CBLA0000840
(1500) A commercial Factor 8 concentrate for treating patients with Haemophilia A.
(1501) Table of Supply for Kryobulin and Bebulin 1969-1972 p2 SHPL0000071_185
(1502) See the chapter on Regulation of Commercial Factor Concentrates.
(1503) Indeed, in the first year that they were licensed the purchase of product proved to be considerably less than half the quantity which the companies had been contracted to supply, on the understanding that the full quantity was one which it was reasonable to expect would be purchased. See also Figure 1 below.
(1504) Some one third of English needs, together with those of Scotland and possibly (at this stage) Northern Ireland, which had no facility of its own to produce blood products other than cryoprecipitate and did not have a population large enough to sustain one.
(1505) Principally Dr Biggs and Dr Charles Rizza at Oxford.
(1506) Dr Terry Snape in his written statement described this in similar terms as the interpretation given in Scotland by a “coherent national blood transfusion service”. Written Statement of Dr Terence Snape para 234 WITN3431001
(1507) Dr Biggs wrote about this to Professor Edward Blackburn: “The problem of the 10 year estimate is very difficult to arrive at by any information apart from that which we are already collecting. I can find out how many patients may accumulate in 10 years because of the rise in average age at death and have taken steps to get this data. The general ‘demand’ for treatment is quite another matter. ‘Need’ is not an absolute concept but reflects a background of useage [sic]. People don’t ‘need’ television sets but they are paid for on social security. Our estimates have been bare minimum amounts of factor VIII ‘needed’ to prevent crippling and to cover surgical operations. If Physicians experience a number of years with an apparently unlimited supply there is no telling how much factor VIII will be used.” Letter from Dr Biggs to Professor Blackburn 28 October 1976 p2 OXUH0003759_004
(1508) That this had real practical consequences is borne out in a memo from Donald Jackson to Michael Lillywhite (DHSS) of 11 July 1975 in which he struggled to provide an estimate for the level of production which would achieve self-sufficiency so as to implement the policy to achieve it because: “It is difficult to be precise in estimating a date for achieving self-sufficiency, not least because not all are agreed as to what constitutes self-sufficiency; some Haemophilia Centre Directors envisage prophylactic treatment whereas the Department’s programme is based upon home treatment of those patients for whom treatment at home can be recommended.” Memo from Donald Jackson to Michael Lillywhite 1 July 1975 DHSC0001774
It is further supported by the views of the Expert Group on the Treatment of Haemophilia and Allied Conditions in May 1976 where the minutes record that: “It must be accepted that the old target [ie for Factor 8 production] was now quite irrelevant to the widely recognised treatment needs of haemophiliacs; it had been rendered out of date largely by the advances of home therapy”. Minutes of Expert Group on the Treatment of Haemophilia and Allied Conditions meeting 4 May 1976 p3 CBLA0007964
Again, in considering what “needs” the Department of Health should plan for, a review of the clinical use of blood and blood products in October 1976 noted: “little information was available to show whether current practice represented optimal use of these products or whether the figures were misleading, due to wasteful practices, and should not therefore be used as a basis for planning. It was also difficult to obtain, from the information available in respect of any product, a reliable estimate of the amount required for the foreseeable future, since in many instances the pattern of treatment which had developed may well have resulted from current shortages which might in time be overcome.” Note on Central Committee for the National Blood Transfusion Service meeting October 1976 p1 DHSC0002181_045
(1509) Letter from John Watt to Dr Biggs 9 November 1976 p2 OXUH0003612_001
(1510) Often short.
(1511) Written Statement of Dr Terence Snape para 234 WITN3431001
(1512) This view, expressed now, was also contemporaneously expressed by B Gidden of the DHSS in a memo of 15 November 1974: “The arrival of the commercial material in quantity precipitated a demand from the NHS which has become more and more insistent, and which could hardly have been anticipated at the time forecast estimates were being drawn up a year ago.” Memo from B Gidden to Mr Campbell 15 November 1974 DHSC0002359_016
(1513) Closing Submission of Collins Solicitors 16 December 2022 paras 511-513 SUBS0000063, Closing Submission of Milners Solicitors 16 December 2022 paras 20-28 SUBS0000055
(1514) Where a very rare blood group was needed, and it had to be sourced from abroad.
(1515) This is important to understand. Many commentators have suggested that “blood” sourced from paid US donors who were in financial need, or in prison, and amongst whom disease was rife was given to UK patients. In a sense, they are right, but it was not given as red blood by transfusion: it was the plasma in the blood which was extracted and which formed the basis of blood products which were supplied in quantity to patients in the UK.
Witnesses who have described nurses speaking of giving American blood are either describing a loose understanding by the nurse, reflecting transfusions given near US bases in the UK where some Americans may have donated, or reflecting having seen blood bags which were labelled as coming from the US. That is true of the plastic bags (supplied to a great extent by Travenol) but not of the contents.
The Inquiry has looked carefully for any evidence that US whole blood or red cells were given to UK residents, and apart from the suggestions made above, and one more below, have found none. In particular there is none of the paperwork that would have accompanied any such supply if it had ever occurred in bulk. It is also inherently unlikely given the adequate supply of whole blood from UK donors within the UK, and the fact that at the time red blood cells had to be stored carefully, and could not be used after three weeks from donation, such that transit over long distances would have been particularly difficult and expensive. Plasma, by contrast, once made into blood products could be freeze dried and transported easily as such. However, there is some evidence of plasma coming from Canada for a while after 1945 as a continuation for a short time of the war effort. The one further discovery is evidence that London private hospitals which would normally expect to be supplied by the NHS would, in times of shortage, source blood from abroad (probably Europe, because of the short shelf-life of whole blood); when, as happened, they were over-provided, they would then pass their surplus to the NHS. In this way some patients in London would be given blood which was not necessarily tested in the same way as NHS blood would have been, which was not necessarily sourced from voluntary donors. The evidence for this is a 1986 report by Dr John Cash. NETHRA Blood Transfusion Services with Special Reference to Hampstead Bloomsbury and Islington 19 March 1986 p5 SBTS0000618_160
(1516) The amount of plasma released by doing this could be increased markedly by use of “SAG-M” (saline-adenine-glucose-mannitol mixture) as described later in this chapter.
(1517) Albeit also part of the NHS.
(1518) Which in turn was likely to depend upon terms and conditions of employment, such as paying a shift premium or an unsocial hours supplement.
(1519) Discussed above. Letter from Dr Biggs to Sir George Godber 22 August 1967 DHSC0100025_062
(1520) The SHHD, which fulfilled the role in Scotland which the DHSS had in England, wrote to the Treasury to say: “we are satisfied on the basis of our experience … the estimates of anti-haemophilic globulin required are … too low. Enquiries are at present in progress and we would not wish to commit ourselves to a new estimate at this stage.” Letter from Andrew Mitchell to Malcolm Widdup 30 May 1968 p3 DHSC0103209_172. In October 1968 the Treasury approved the changed proposals. Letter from Malcolm Widdup to Andrew Mitchell 24 October 1968 DHSC0103209_160. Dr Biggs’ view that more AHF/AHG was needed appeared therefore to be shared, and to have been convincing enough that the Treasury were prepared to fund preparations to meet it.
(1521) It is not clear how this fitted with the use of the “named patient exemption”, which was the permitted ground for importing unlicensed material for therapeutic use. (See the chapter on Regulation of Commercial Factor Concentrates). There is no evidence that the substance of this letter was shared more widely. It appears to be a plea for a local purchase. Letter from Dr Rizza to W Trillwood 18 July 1972 p2 OXUH0000673
(1522) Minutes of Haemophilia Centre Directors meeting 27 October 1972 pp8-10 HCDO0001015
(1523) Minutes of Haemophilia Centre Directors meeting 27 October 1972 pp5-7 HCDO0001015. England had a number of “haemophilia reference centres” (larger, specialist provision) to which “haemophilia centres” within their area could make reference. Oxford was the reference centre for the Alton Centre which served Treloar’s school.
(1524) Dr Biggs’ conclusion was that to enable these therapies in addition to hospital provision, some 500,000 donor units would be needed annually for England and Wales, with 250,000 of those in the form of freeze-dried concentrate, and the other 250,000 cryoprecipitate. Minutes of Haemophilia Centre Directors meeting 27 October 1972 pp8-10 HCDO0001015
(1525) Letter from Professor Blackburn to Sir George Godber 12 December 1972 pp1-2 BPLL0008096_002
(1526) Letter from Dr Maycock to Dr John Reid 24 January 1973 DHSC0100026_164
(1527) Letter from Dr Maycock to Dr Reid 7 February 1973 p1 BPLL0008090. He wrote: “as far as possible, the UK should aim to be self-sufficient in the supply of preparations of anti-haemophilic globulin and Factor IX. The preparations made in this country are as good as any available commercially from abroad and can be made by the transfusion services here more cheaply. However, at present insufficient anti-haemophilic globulin concentrate is made in the UK. There is thus considerable pressure from those who treat haemophiliacs for foreign commercial material to be bought. There is indeed, at present, the need to supplement the existing UK supply but the facilities for larger fractionation that will become available in England and Scotland should eliminate the need to use foreign commercial preparations or go a long way towards doing so.”
(1528) Memo from Sir George Godber to Sir Philip Rogers 6 February 1973 DHSC0003741_136, Memo from Sir Philip Rogers to Sir George Godber 9 February 1973 DHSC0003741_135. The Permanent Secretary ends with the words: “Furthermore, it would be helpful for us to have any estimate at all that is possible of the likely increase of cost, since I confess to be somewhat alarmed by your estimate ‘in millions of pounds.’” It seems plain that whether commercial or domestic concentrates were to be used, expense was thought unavoidable in principle, would be high, and that providing for domestic supplies was likely to be cheaper than purchasing commercial supplies.
(1529) Minutes of the Expert Group on the Treatment of Haemophilia meeting 20 March 1973 pp1-2 PRSE0004706
(1530) This range, in which the higher figure is almost double the lower, is itself indicative of the scarcity of reliable information about how many people had haemophilia and what the severity of their condition was.
(1531) Factor VIII Concentrates and the Treatment of Haemophilia pp17-18 PRSE0002553
(1532) Minutes of the Expert Group on the Treatment of Haemophilia meeting 20 March 1973 p3 PRSE0004706
(1533) Minutes of the Expert Group on the Treatment of Haemophilia meeting 20 March 1973 p4 PRSE0004706
(1534) Approximately 44,000 donor units for plasma, 220,000 donor units for cryoprecipitate and 25,000 donor units for concentrate. Factor VIII Concentrates and the Treatment of Haemophilia p21 PRSE0002553
(1535) Present Sources of Materials for Treatment of Haemophilia and Potential Future Sources March 1973 p1 DHSC0100005_132. Litres is the unit of measurement used here. Approximately five-donor units contribute a litre of plasma when the plasma is recovered from the donation (it is known as “recovered plasma”). Accordingly, 135 litres per week equals around 675 donor units per week, or 351,000 per year.
(1536) The term “activity” can be used interchangeably with the term “level” to describe the amount of clotting factor present in the blood. For example, normal Factor 8 levels expressed as a percentage range from 50-150% (100% being an average, not the very top of a range) but a person with haemophilia will have Factor 8 activity of less than 50%.
(1537) Though it is likely that a litre of plasma yielded more international units if it was fractionated into cryoprecipitate than it would when further processed to make AHG concentrate, the need to err on the side of overprescription with cryoprecipitate may have evened the score once they had been used for treatment. There was little to choose between them, therefore, on the basis of yield so far as practical use was concerned.
(1538) There is a lack of consistency between different documents from this period – some figures are for the total usage of factor replacement therapies (ie both cryoprecipitate and concentrate, and (at least at an early stage) some FFP); some figures are for England and Wales, others for the whole UK. These divergences need to be borne in mind when attempting to interpret what the figures shown actually meant. The 275,000 figure relates to the amount for fractionation.
(1539) This is the full name of the working party. There was another working party that was simply the Blood Transfusion Working Party which started in 1980.
(1540) Treloar’s is examined in a separate chapter, and its enthusiasm for the administration of large amounts of factor concentrate should be noted.
(1541) It did not need to be unless it is assumed that all factor replacement therapy was to be provided by means of factor concentrate, and that there was no place for cryoprecipitate. It is also notable that the paper appears to accept the probability that pools of plasma used to make concentrates would be more likely to contain hepatitis viruses but that “the incidence of jaundice in multi-transfusion haemophilic patients does not rise very greatly with the use of freeze-dried concentrates.” Factor VIII Concentrates Made in the United Kingdom and the Treatment of Haemophilia Based on Studies Made During 1969-1972 p21 PRSE0002350. As reported elsewhere in this Report, this questionable assertion was based upon studies concluded before 1973, at a time when NHS pools had a mean size of less than 200 donors, and a time when there was little commercial concentrate in use from which to draw comparisons between cryoprecipitate therapy and the use of commercial concentrates. It seems clear that Dr Biggs was an enthusiast for concentrates, to the extent of seeing little or no place for cryoprecipitate, and downplayed the risks.
(1542) Factor VIII Concentrates Made in the United Kingdom and the Treatment of Haemophilia Based on Studies Made During 1969-1972 PRSE0002350, Biggs et al Factor VIII Concentrates Made in the United Kingdom and the Treatment of Haemophilia Based on Studies Made During 1969-72 British Journal of Haematology 1974 MULL0002860. Dr Biggs was the principal author, but other members of the working party included Dr Maycock, Professor Blackburn and Dr Rizza.
(1543) The treating doctors would expect to have the “clinical freedom” to prescribe as they thought best for their patient, so their views as to this were critical. Letter from Dr Bowley to colleagues 17 December 1973 CBLA0000171
(1544) She was suggesting a tenfold increase in the amount to go to BPL/PFC to make concentrates. Dr Bowley saw it as her asking that one third of all blood donations should be sent for fractionation.
(1545) Letter from Dr Bowley to colleagues 17 December 1973 p1 CBLA0000171
(1546) Wallace Treatment of Haemophilia 1973 p5 OXUH0000823
(1547) BPL, Elstree.
(1548) Additional staff, equipment and facilities would however be needed. Dr Sheila Waiter could not say how the extra expense of this would be met but reference should be made to the DHSS. She “made the point that the purchase of commercial AHG was already costing the DHSS a lot of money.” The discussion ended by saying: “it was stressed that the estimates [in Dr Biggs’ paper] are just for present and that in five years time there may be a need for more material ... The Chairman agreed to write to the D.H.S.S. saying that the meeting of Haemophilia Centre Directors and Transfusion Directors, approved the contents of [Dr Biggs’ paper] and recommended that this document be used as the basis for planning the future requirements for factor VIII in the United Kingdom.” Minutes of Haemophilia Centre Directors and Blood Transfusion Directors joint meeting 31 January 1974 p7 CBLA0000187
(1549) Nor additional funding for the Oxford Centre.
(1550) Letter from Dr Biggs to Dr Waiter 23 May 1974 CBLA0000206. She told Dr Waiter that she felt that the NHS could provide Factor 8 “in absolutely adequate amounts, if only a little money and effort could go into the fractionation laboratories.”
(1551) There could be more than one reason for this dramatic failure to buy commercial concentrates. The fact that around one third of the anticipated take-up only was bought could support Dr Bowley’s view that enough cryoprecipitate and NHS concentrate was already being provided; it could be seen as tacit support for his suggestion that Dr Biggs and others had been asking for too much. But it may also be seen to demonstrate a problem with persuading regional health authorities to make significant funds available to treat a condition which only a small minority of patients in its region had. It may indicate that regional treasurers doubted whether funding home treatment (likely to be a large user of concentrate) was needed, and thus both support Dr Biggs’ view that it was because of the expense of factor concentrate, and the views of those who thought that home treatment was not such a pressing need that the regions should be funding it.
(1552) Biggs Letter to the Editor on Supply of Blood-Clotting-Factor VIII for Treatment of Haemophilia The Lancet 29 June 1974 PRSE0002515
(1553) Dr Owen was initially appointed Parliamentary Under-Secretary for Health in March 1974 and then Minister of State for Health in July 1974.
(1554) Hansard written answer on Haemophilia 9 July 1974 p1 LDOW0000032, Memo from B Gidden to L Brandes DHSC0100005_108
(1555) This followed an understanding that whereas the figure of 250,000 donations had been based upon a view that a donation would provide 200ml for fractionation as it did at Oxford, a more accurate figure across the country was 180-190ml of plasma. Minutes of Joint Steering Committee on Blood Products Production meeting 20 June 1973 p5 PRSE0004359, Minutes of Regional Transfusion Directors meeting 20 July 1973 p3 CBLA0000153, Plasma Needed for the Preparation of Antihaemophilic Concentrate CBLA0000154
(1556) Minutes of Regional Transfusion Directors meeting 3 July 1974 p5 NHBT0016495. Indeed, Dr Maycock went so far as to tell the July 1974 meeting of RTDs that “The Department [of Health] had been advised that the NBTS [National Blood Transfusion Service] should reach the position of being able to supply this amount of concentrate [from 275,000 donations] by 1975, but this was clearly not possible.” Minutes of Regional Transfusion Directors meeting 3 July 1974 p5 NHBT0016495
(1557) Minutes of Regional Transfusion Directors meeting 3 July 1974 p5 NHBT0016495
(1558) Minutes of Regional Transfusion Directors meeting 3 July 1974 pp5-6 NHBT0016495
(1559) This was based on meeting the target of 275,000 from BPL, PFL and PFC’s fractionation capacities, rather than the MRC Working Party’s range of up to 750,000 donations per year.
(1560) Minutes of Regional Transfusion Directors meeting 3 July 1974 pp5-6 NHBT0016495
(1561) It made little or no sense for plasma which could go to make factor replacement therapies to go unnecessarily into the bloodstream of patients instead.
(1562) Letter from B Gidden to regional administrators 24 December 1974 p1 CBLA0000239
(1563) The best solution of all.
(1564) See for example: Blackburn Letter to the Editor on Treatment of Haemophilia The Lancet 13 July 1974 WITN6914033, Blood Donors and the Transfusion Service British Medical Journal 27 July 1974 DHSC0100024_126, Minutes of Joint Steering Committee on Blood Products Production meeting 20 June 1973 pp6-7 PRSE0004359, Letter from Professor Blackburn to Dr Waiter February 1974 OXUH0003603_004, Letter to Dr Waiter 4 March 1974 OXUH0003604_002, Letter from Dr Waiter to Professor Blackburn 2 February 1974 OXUH0003604_003
(1565) Note the superlative.
(1566) PPF is plasma protein fraction, an albumin fraction, which was replacing dried plasma and plasma substitutes. It was commercially available too, but also a product which could be made domestically.
(1567) Letter from B Gidden to regional administrators 24 December 1974 CBLA0000239
(1568) Hansard written answer on Haemophilia 22 January 1975 p3 LDOW0000032. On 25 February 1975 he told Parliament: “I have authorised the allocation of special finance of up to £500,000, about half of which would be recurring”. He also said: “If we were to go to all-commercial purchase of this factor, it would cost an additional £1½ million to £2 million annually.” Hansard oral answer on Haemophiliacs (Drugs) 25 February 1975 HSOC0015202
(1569) Lord David Owen Transcript 22 September 2020 pp186-189 INQY1000055
(1570) Hansard written answer on Haemophilia 22 January 1975 p4 LDOW0000032, Hansard oral answer on Haemophiliacs (Drugs) 25 February 1975 1975 HSOC0015202
(1571) Hansard written answers on Haemophilia 7 July 1975 DHSC0000281
(1572) Donald Jackson worked in the DHSS Health Service Division. The responsibilities of the Division included the policy on blood products.
(1573) The emphasis is as in the original. He noted that “some Haemophilia Centre Directors envisage prophylactic treatment whereas the Department’s programme is based upon home treatment of those patients for whom treatment at home can be recommended.” Memo from Donald Jackson to Michael Lillywhite 11 July 1975 pp1-2 DHSC0001774
(1574) The basis for saying that he was probably not fully briefed appears from two departmental sources. (1) Note of Minister of State (Health) meeting 11 December 1975 DHSC0100006_093. “The Haemophilia Society was anxious that the volume target set by the Department for self-sufficiency might not be sufficient in practice – the MRC study had said a figure of 500,000 rather than 340,000 was necessary. The Society wondered if greater use of plasmapheresis was a viable solution ... [Dr Owen said he] would look at the MRC study and would write to the Society giving the basis for the Department’s target. He stressed his personal commitment to self-sufficiency.” (2) Note from M Draper to Thomas Dutton 15 December 1975 DHSC0100006_092. “Dr Owen asked me to let him have a copy of ‘the MRC report’ from which the Society were quoting (they mentioned Dr Rosemary Biggs). Could you have a word with Dr Waiter and let me have a note, with the Report if available, fairly soon?” The briefing paper Dr Owen would have had in advance of this meeting is one of the papers the Inquiry has been unable to trace, so it is impossible to say with certainty that the Minister had not been briefed about Dr Biggs’ paper before the meeting or the previous December when he made decisions about self-sufficiency (though he should have been). A reasonable inference is that, not least given his commitment to self-sufficiency, he would probably have been aware of the contents of the document if he had seen it.
(1575) RTD (75) 26 is a document which sets out the regional transfusion directors’ estimates of the number of donations to be used for the production of fresh plasma from AHG concentrate each quarter from 1975 to mid 1977. Production of Fresh Plasma for AHG Concentrate RTD(75)26 DHSC0002179_045
(1576) The proportion of active Factor 8 protein in a finished product when compared with the amount in the plasma used to make it.
(1577) Production of factor VIII concentrate 27 January 1976 CBLA0000336
(1578) Dr Bidwell does not explain what she was referring to as the “latest data from Dr Biggs” on which she bases her assumptions. Interestingly, Dr Richard Lane subsequently commented that these calculations were “based on yields which were far closer to what I consider realistic.” Draft Proof of Evidence of Dr Lane for HIV Haemophilia Litigation 10 December 1990 pp74-76 CBLA0000005_002
(1579) Her assumption was a yield of 200-220ml, which was being obtained in Oxford. Dr Maycock’s assumption had been that 180ml could be expected across the UK. Minutes of Expert Group on the Treatment of Haemophilia and Allied Conditions meeting 4 May 1976 p2 CBLA0007964
(1580) Minutes of Expert Group on the Treatment of Haemophilia and Allied Conditions meeting 4 May 1976 pp3-4 CBLA0007964. The minutes also recorded that it “must be accepted that the old target was now quite irrelevant to the widely recognised treatment needs of haemophiliacs; it had been rendered out of date largely by the advances of home therapy.”
(1581) Brief for Central Committee for the National Blood Transfusion Service meeting 22 June 1976 para 7 DHSC0103254. Dr Owen was also briefed about it. He was told that “the target figure to which we [ie the DHSS] are currently working was no longer sufficient to meet the probable treatment needs of haemophiliacs in a few years time, having been overtaken particularly by the unexpectedly rapid introduction of home therapy ... the Departments are considering the implications for them and for the NBTS of a situation in which approximately 60% of the total blood donations collected may have to be fractionated in order to provide sufficient of one factor to treat 3000 patients.” Dr Owen responded: “This was inevitable and comes as no surprise at all. This only demonstrates once again why we must reform the National Blood Transfusion Service.” Memo from Thomas Dutton to M Draper and Michael Lillywhite 18 June 1976 DHSC0100006_143, Note on anti-haemophilic globulin concentrate DHSC0100006_144, Letter from Gerry Grimstone to Thomas Dutton 21 June 1976 DHSC0100006_145
(1582) Minutes of National Blood Transfusion Service Central Committee meeting 22 June 1976 p4 DHSC0103255
(1583) The Inquiry has a copy signed by Thomas Dutton and the note refers to it having been prepared by one of them. Problems Facing the National Blood Transfusion Service – Particularly with regard to the Provision of Blood Components September 1976 DHSC0103249_071. However, Dr Waiter does not indicate any disagreement with its contents, and the form of its presentation suggests it is a joint offering to the Committee, such that it is proper to refer to it in the text of this Report as a paper from Thomas Dutton and Dr Waiter.
(1584) Note on Central Committee for the National Blood Transfusion Service meeting pp3-4 October 1976 DHSC0002181_045
(1585) Minutes of Haemophilia Centre Directors meeting 13 January 1977 p14 PRSE0002268
(1586) Dr Lane, who became director of BPL in 1978, thought it curious that the capacity should have been thought “adequate”: Draft Proof of Evidence of Dr Lane for HIV Haemophilia Litigation 10 December 1990 para 133, paras 135-136 CBLA0000005_002
(1587) Dr Bidwell, director of PFL at Oxford, told the meeting that supply of plasma was the current limiting factor for production at PFL, but it was expected to double in the next year and there would be no room for any further expansion (ie approximately 2.5 million international units would be the maximum).
(1588) Minutes of Haemophilia Centre Directors meeting 13 January 1977 pp15-18 PRSE0002268
(1589) The second meeting followed in July 1977. Minutes of Working Group on Trends in the Demand for Blood Products meeting 3 February 1977 DHSC0003616_109, Minutes of Working Group on Trends in the Demand for Blood Products meeting 3 February 1977 DHSC0002183_065
(1590) Report of the Working Group on Trends in the Demand for Blood Products December 1977 DHSC0001318
(1591) Report of the Working Group on Trends in the Demand for Blood Products December 1977 p5 DHSC0001318. The working party estimated the international units per 1,000 population. Dr Lane said this “projected utilisation of factor VIII concentrate to grow to 60M iu [international units] per annum over a ten-year period” but suggested a more realistic estimate to achieve self-sufficiency “could be 100M iu per annum” and complained about “substantial under-investment in BPL”. Minutes of Association of Haematologists North East Thames Region Working Party in Haemophilia meeting 16 December 1978 p3 BART0000686. Dr Diana Walford gave the figure of 74 million international units in her written statement, which was what would be achieved when the requirements for albumin were met. Written Statement of Dr Diana Walford para 12.2 WITN4461001. The fractionation process would first extract factor concentrates from the plasma, and then go on to extract albumin. Such was the amount of albumin needed that the plasma for its production would provide for a greater requirement for Factor 8; on her figures, therefore equating to some 74 million international units per year.
(1592) Report of the Working Group on Trends in the Demand for Blood Products December 1977 pp4-5 DHSC0001318.
(1593) And it would rise over time as the population increased as it was expected to do.
(1594) It should also be noted that there were upward pressures beyond population growth alone. Life expectancy in people with haemophilia had increased markedly since the introduction of cryoprecipitate, and this meant that the percentage of people with haemophilia in the population was also increasing. Home therapy was more widespread than it had been, and prophylaxis was yet to be widely utilised.
(1595) It is not clear precisely what he had in mind as leading to an increase in capacity. Assuming what he had said to Parliament was correct, it is plain that shortfalls in plasma supply were no longer a reason for failure to reach self-sufficiency, but the absence of sufficient production facilities was (or a change of treatment to allow for the greater use of cryoprecipitate, which could continue to be made locally). Plans ought already to have been made to increase production facilities so that they could cope with reasonably foreseeable demands in the medium-term future: this statement should have rung alarm bells as to progress on this.
(1596) It was being met by the increasing use of imported blood products. Hansard written answers on Haemophilia 26 June 1978 p1 DHSC0000291
(1597) Hansard written answers on Haemophilia 26 June 1978 p1 DHSC0000291
(1598) Parliamentary written answer on Factor VIII by Roland Moyle 15 December 1978 DHSC0002191_017. The question he was answering asked if he would make a statement on his success in rendering the NHS self-sufficient in the provision of freeze-dried Factor 8. He did not question the commitment to do so, but by use of the words “not yet” plainly recognised it as a continuing aim.
(1599) Minutes of Standing Medical Advisory Committee meeting 11 April 1978 p4 DHSC0103130. The Committee was constituted by the National Health Service Act 1946. Dr Waiter noted that the Committee expected an increasing requirement for Factor 8 for orthopaedic surgery and David Smart recorded the modified figures. Memo from Dr Waiter to Dr Maycock, Dr Raison, Mr Parrott and Thomas Dutton 24 April 1978 DHSC0002187_020, Blood Products Laboratory: Redevelopment May 1979 p2 CBLA0001004_004
(1600) Memo from Thomas Dutton to Mr Parrott 3 January 1977 p1 DHSC0002183_009. Though the document is dated 3 January 1977 this is likely to be a misdate, for 1978, since the report to which it refers was produced only shortly beforehand. As to Thomas Dutton’s assertion that it had by this time become generally accepted that something in the region of 1,000 international units per 1,000 population was needed to provide sufficient treatment to people with haemophilia (approximately 60 million units), Dr Lane for his part thought 100 million units could be a realistic assessment. Minutes of Association of Haematologists North East Thames Region Working Party in Haemophilia meeting 29 November 1978 p3 BART0000686. The working party also noted in its July meeting that the size of the population with haemophilia could rise significantly. Interestingly, they also said: “It was apparent that clinicians were coming to recognise the supply problems; eg, they were moderating their demands for Factor VIII for prophylactic treatment.” Minutes of Working Group on Trends in the Demand for Blood Products meeting 13 July 1977 p2 DHSC0002183_065
(1601) Memo from Thomas Dutton to Mr Parrott 3 January 1977 p3 DHSC0002183_009
(1602) Memo from Thomas Dutton to Mr Parrott 3 January 1977 pp5-6 DHSC0002183_009
(1603) Parliamentary written answer on Factor VIII by Roland Moyle 15 December 1978 DHSC0002191_017
(1604) The Handling of the Trends Working Party Report 26 April 1978 DHSC0002325_013
(1605) Minutes of National Blood Transfusion Service Scientific and Technical Committee meeting 26 March 1979 p2 BPLL0008430_001
(1606) Dr Geoffrey Tovey, who had succeeded Dr Maycock as consultant adviser to the Chief Medical Officer in respect of blood transfusion, thought that if the publicity were right there would be no difficulty in obtaining all the plasma necessary to support a programme rising to 100 million international units per annum. Minutes of National Blood Transfusion Service Scientific and Technical Committee meeting 26 March 1979 p2 BPLL0008430_001
(1607) The intermediate target would require 375,000 litres of FFP per annum. Converting to kilograms by using a specific gravity of 1.03 this equates to just under 390,000 kilograms. The Function of Stop-Gap and Phased Redevelopment of the Blood Products Laboratory 31 May 1979 p16 BPLL0001508
(1608) Capable of producing 100 million international units of Factor 8 and 15 million units of Factor 9. An Appraisal of Redevelopment Options for the Blood Products Laboratory p4 CBLA0001606, Blood Products Laboratory: Redevelopment DHSC0002309_108, Minutes of discussion regarding the redevelopment of the Blood Products Laboratory meeting 7 October 1982 DHSC0002309_019, Letter from Jeremy Colman to D Harris 11 November 1982 DHSC0002319_013
(1609) Chronological Presentation on the Domestic Supply of Blood Products in England and Wales Appendix 1 Factor VIII Demand Estimates March 2022 paras 66-67, para 71 INQY0000336
(1610) See for example Dr Maycock identifying in March 1973 that the requirement was for more than the fractionation capacity of the three plants after building operations were completed, even assuming some further increase in capacity. Present Sources of Materials for Treatment of Haemophilia and Potential Future Sources March 1973 DHSC0100005_132
(1611) Annual consumption of factor VIII in UK 23 August 1999 DHSC0006789_046, Table 5.3.1 showing annual consumption of CFC 1976 to 1994 WITN3826017
(1612) Annual consumption of factor VIII in UK 23 August 1999 DHSC0006789_046, Table 5.3.1 showing annual consumption of CFC 1976 to 1994 WITN3826017, Production of factor VIII concentrate 27 January 1976 CBLA0000336
(1613) See the chapter on Regulation of Commercial Factor Concentrates.
(1614) Annual consumption of factor VIII in UK 23 August 1999 DHSC0006789_046, Table 5.3.1 showing annual consumption of CFC 1976 to 1994 WITN3826017, Letter from Dr Biggs to Professor Blackburn 28 October 1976 OXUH0003759_004, Appendix 4 Factor VIII: Capacity, Production and Demand 1973-1990 CBLA0000004_010
(1615) The following data points have been added to the chart regarding consumption of Factor 8 in the UK: (a) MRC Working Party estimate made in 1974 of 547,540 - 750,000 blood donations, estimated by Dr Biggs as likely to be 38,327,800 - 53,000,000 million units. Factor VIII Concentrates Made in the United Kingdom and the Treatment of Haemophilia Based on Studies Made During 1969-1972 p18 PRSE0002350. (b) DHSS planning target for 1977 of 343,000 donations, estimated by Dr Bidwell to be 12,350,000 million units. Production of factor VIII concentrate 27 January 1976 CBLA0000336. (c) DHSS planning targets up to 1985 set by the Trends Working Group and modified by the Standing Advisory Group, recorded by David Smart. Blood Products Laboratory: Redevelopment May 1979 p2 CBLA0001004_004. (d) DHSS planning target of 100 million units agreed for the redevelopment of BPL for 1986. An Appraisal of Redevelopment Options for the Blood Products Laboratory p4 CBLA0001606
(1616) Or, as will be seen below in the text, because use was not made as it might have been of the production facilities in Edinburgh.
(1617) This is due to lower iron levels in women.
(1618) It is worth noting however, that in the early 1970s there were calls for plasmapheresis to be used more frequently.
(1619) Note that one of the arguments raised about the capacity of Edinburgh to produce factor concentrates was that processes there were better suited to the production of other products which could be made from time-expired plasma.
(1620) BPL Background and Current Information for Members of the CBLA June 1985 p139 CBLA0002201
(1621) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine Vol 6 1996 p61 NHBT0000028
(1622) Blood Donors and the Transfusion Service 27 July 1974 DHSC0100024_126
(1623) Thomas Dutton and Dr Waiter as joint secretaries to the Central Committee for the National Blood Transfusion Service, reflecting respectively their roles as senior officials in the policy and the medical branches of the Civil Service which at that time dealt with medical and policy issues in separate streams, sent the paper attached to a note for the Central Committee for the National Blood Transfusion Service meeting in October 1976. Note on Central Committee for the National Blood Transfusion Service meeting October 1976 p3 DHSC0002181_045
(1624) Emphasis added. He also wrote: “There is ample evidence that the NBTS has the knowledge and experience to meet NHS requirements for most blood components in full. The difficulties currently being encountered appear to arise to a substantial extent from the complication of financing a service in which Regions make a contribution to a national programme for the provision of a particular blood component and in so doing incur expenditure which may bear no relationship to the value of the amount of that component which the Region requires for its own purposes. There are many reasons why a Region’s ability to contribute to a national programme may not always match its requirement for the finished product.
As long as the collection, testing and despatch of whole blood was the predominant occupation of blood transfusion centres they were able to function as independent regional units which were largely self-sufficient except in times of emergency. The adequacy of independent self-sufficient regional units was however greatly reduced with the introduction of component therapy on a large scale. What now appears to be needed is some method of building up a ‘production partnership’ between the individual Regional Transfusion Centres and the central Blood Products Laboratories so that they each contribute to the maximum to the total NHS requirement for blood products, possibly according to an agreed programme.” Note on Central Committee for the National Blood Transfusion Service meeting October 1976 p3 DHSC0002181_045
(1625) This view – that there was significant delay in adopting a suitable production programme – is in essence the same as the view later expressed by several witnesses to the Inquiry that the construction of new production facilities for BPL in order that it might meet the demand for factor concentrates was very considerably delayed: Dr Diana Walford, for instance, described it as “unconscionable”. Dr Diana Walford Transcript 20 July 2021 p29 INQY1000137. It was six years after this particular recognition of delay until the go-ahead was given to rebuild BPL.
(1626) His proposal followed the recognition in the paper by Thomas Dutton and Dr Waiter that there was no clear relationship between the effort that regions had been asked to make to increase plasma supply to central production facilities and the reward which they would receive for those efforts. A first step was that in December 1976 a new scheme of distribution for NHS Factor 8 concentrates was introduced. The amount to be sent to each region would be calculated by reference to the number of patients reported as being treated in the haemophilia centres of that region in 1974. Unconfirmed Minutes of Haemophilia/Associate Haemophilia Centre and Blood Transfusion Centre Directors and Regional Health Authorities meeting 15 December 1976 pp1-2 CBLA0000533. In November 1979 Dr Lane proposed a scheme that allowed regions to receive their concentrate and albumin in proportion to the yield from the plasma they had sent to BPL. He argued that that would provide regions with a meaningful link to BPL and would incentivise and improve the plasma collection system. Slowly, his proposal gained support. Not only might it increase the quantity of plasma supplied by regions, but also its quality, because the yield gained from the plasma supplied would be taken into account in determining the pro rata distribution. The better the quality of the base plasma, the greater the yield, the higher the pro rata return of finished product to the region. Note on Haemophilia Centre Directors meeting 20-21 December 1978 p2 DHSC0002195_065
(1627) Note on the distribution of blood products DHSC0105495_053. Factor 9 fell outside the scheme, because it was considered that the UK was self-sufficient in Factor 9, such that it could be provided on demand, and its inclusion in the pro rata scheme might result in more Factor 9 being produced than was actually needed.
(1628) The scheme remained broadly in place until 1989, though there were some variations when construction works occurred at BPL, and when heat treatment of factor products was first introduced.
(1629) Under the cross-charging system, BPL paid regional transfusion centres a national price for supplying plasma and the regions paid BPL for the blood products supplied. It was anticipated that that would permit a more rational and efficient means of encouraging plasma supply and the distribution of blood products. See: Letter from Dr Edmund Harris to Dr Gunson 14 April 1988 DHSC0002032, Central Blood Laboratories Authority: Activity and Current Issues Update Report May 1988 DHSC0003593_044, Letter from Malcolm Harris to Ms Westbrook 20 May 1988 DHSC0003593_040
(1630) This refers to all doctors who might use blood for transfusions.
(1631) The problems of over-transfusion and the slow movement towards giving patients less blood are discussed in greater detail in the chapter on Blood Transfusion: Clinical Practice Screening.
(1632) ie doctors who were involved in obtaining blood from donors and supplying hospitals in their region with sufficient blood for their anticipated needs.
(1633) It would only be where the behaviour of a doctor was such as to make his peers feel that his practice might be dangerous, or otherwise be so surprised by it that a complaint was made to the regulatory body, that a change was likely to occur.
(1634) Except in Scotland, which was far in front of England and Wales in this respect. Letter from B Gidden to regional administrators 24 December 1974 p1 CBLA0000239
(1635) Chronological Presentation on the Domestic Supply of Blood Products in England and Wales Appendix 5: The Role of the Single Donor Plasma Pack in Plasma Supply in the 1970s and 1980s March 2022 p2 INQY0000338
(1636) Radioimmunoassay test for Hepatitis B.
(1637) Factor 8 activity degrades quickly over time when in plasma in a liquid state. Freezing plasma was quicker with a smaller pack, losing less activity at that stage. Further, where a five-litre pack was thawed, it was a slow process: thawing too quickly could also degrade the factor. The part in contact with the outside wall of the thawing pack became liquid some time before the centre did: the process was by contrast much quicker with a single plasma pack, where the surface area to volume was much greater, so it thawed more quickly and less activity was lost before the pack could be used.
(1638) Chronological Presentation on the Domestic Supply of Blood Products in England and Wales Appendix 5: The Role of the Single Donor Plasma Pack in Plasma Supply in the 1970s and 1980s March 2022 p6 INQY0000338
(1639) Leeds, Southampton and Liverpool all reported they would be able to send more fresh frozen plasma to BPL if it accepted single packs rather than five-litre ones. Table showing Supply of Fresh Frozen Plasma by RTCs CBLA0000743
(1640) ie since Dr Owen’s initiative. BPL and PFL Annual Report 1981/82 20 April 1982 p4 CBLA0001570
(1641) DHSS Notes on Transfusion 1973 p4 HCDO0000861. The edition quoted is that which was revised in 1973. It was issued for the NBTS and the Scottish Blood Transfusion Association.
(1642) The same point was then emphatically made, again, under the paragraph which immediately followed headed “Choice of Fluid”. This began “WHOLE BLOOD is used to restore blood volume. Its use where concentrated red cells are more suitable is not good transfusion practice.”
(1643) Making them thick and sticky.
(1644) Minutes of Scottish National Blood Transfusion Service (“SNBTS”) Directors meeting 11 June 1975 p3 PRSE0003812; see also Letter from Dr Wallace to Dr Brodie Lewis 6 May 1974 p3 SBTS0000289_116
(1645) It seems a greater proportion was recovered in Scotland. Extract from The Treatment of Haemophilia A and B and von Willebrand’s Disease 1977 p9 BPLL0002571_015. Usually there would be about 300ml of plasma in one donation, though not all of this would be recovered.
(1646) This was developed by Travenol Laboratories in the US.
(1647) Cutter Laboratories International Division 1983 Preliminary Marketing Plan 1983 p5 CGRA0000586
(1648) BPL Background and Current Information for Members of the CBLA June 1985 pp101-102 CBLA0002201. It was calculated that optimal additive solutions such as SAG-M, combined with further growth in the percentage of concentrated red blood cells rather than whole blood could yield a maximum of 360,000kg of plasma per annum and more likely approximately 320,000kg. At that stage, it was thought 450,000kg of plasma would be required by the second half of the 1980s.
(1649) Minutes of Regional Transfusion Directors meeting 14 January 1983 pp3-4 CBLA0001663
(1650) Dr Lane stated in a symposium (organised for the NHS by Travenol, the developer of SAG-M) in 1983 that use of SAG-M would result in 100ml more from each unit of whole blood. Value of SAG-M Systems in the Provision of Plasma Products 1983 p2 CBLA0001779. Dr Gunson, director of Manchester RTC and consultant adviser to the CMO on matters of transfusion (he had succeeded Dr Tovey, who had in turn succeeded Dr Maycock), gave a figure of approximately 275ml of plasma per donation after SAG-M had been used, which was a slightly more conservative figure than Dr Lane adopted. Gunson Trends in blood transfusion practice in England and Wales Health Trends November 1986 p3 NHBT0017097
(1651) Appendix 4 Factor VIII: Capacity, Production and Demand 1973-1990 p20 CBLA0000004_010
(1652) Letter from Dr Contreras and others to the Editor of The Economist 12 October 1987 NHBT0086659, Written Statement of Professor Dame Marcela Contreras paras 467-479 WITN5711001, Professor Dame Marcela Contreras Transcript 2 December 2021 pp142-146 INQY1000165
(1653) Dr Thomas Cleghorn made the suggestion. Minutes of Regional Transfusion Directors meeting 17 December 1969 p7 NHBT0017068
(1654) Dr Maycock Present Sources of Materials for Treatment of Haemophilia and Potential Future Sources March 1973 p2 DHSC0100005_132
(1655) Minutes of Expert Group on the Treatment of Haemophilia meeting 20 March 1973 p4 PRSE0004706
(1656) Written Statement of Dr Terence Snape para 218 WITN3431001. 500ml was obtained by plasmapheresis; 200ml if it was recovered plasma.
(1657) At a special meeting of regional transfusion directors it was agreed that if the use of concentrated red cells could be increased there would be no need to consider plasmapheresis. Minutes of Regional Transfusion Directors meeting 20 July 1973 p4 CBLA0000153
(1658) Provision of Plasma for AHG Concentrate 1973 p2 CBLA0000155
(1659) Central Committee for the NBTS Clinical use of Red Cell Preparations 1975 DHSC0002359_039. Although by 1975 Dr Biggs thought that the additional units of blood then being sought to achieve self-sufficiency could not be obtained without the establishment of plasmapheresis, a DHSS minute recorded that it was not the intention to embark on a programme of plasmapheresis in England. Note of meeting between Dr Biggs and Dr Rizza 12 June 1975 p3 BAYP0000022_073, Memo for Factor 8 Production Directors meeting 11 March 1976 p1 CBLA0008747
(1660) Minutes of SNBTS Directors meeting 11 June 1975 p4 PRSE0003812. However, between 1975-76 there was an increase of 82% in the number of units obtained by plasmapheresis of fresh frozen plasma. It seemed that Edinburgh, in particular, was using more plasmapheresis. SNBTS Annual Report 1975/76 pp33-34 PRSE0002133
(1661) Note from M Draper to Thomas Dutton 15 December 1975 DHSC0100006_092
(1662) Code of Practice for the Clinical Use of Blood Cell Separators 1977 pp11-12 SCGV0000081_004
(1663) Later to become the medical director of NHSBT.
(1664) Written Statement of Dr Angela Robinson paras 770-773 WITN6926001
(1665) Minutes of DHSS meeting 3 March 1980 p2 DHSC0002313_030
(1666) Minutes of Advisory Committee on the NBTS meeting 23 February 1981 p4 CBLA0001287
(1667) It was tried out by Dr Robinson in Bradford, using six machines. She reported her findings to the NBTS and later wrote the pilot study up in Vox Sanguinis for early 1983. The study found that “The results show that large-scale automated plasmapheresis could safely and economically produce high-quality source plasma necessary for national self-sufficiency.” Pilot study for large scale plasma procurement using automated plasmapheresis 16 April 1981 p2 DHSC0002207_054, Robinson et al Pilot Study for Large-Scale Plasma Procurement Using Automated Plasmapheresis Vox Sanguinis 44:143-150 1983 DHSC0002263_064
(1668) Thus on 18 February 1981, the North East Scotland Blood Transfusion Centre described in a letter their plan to increase the use of plasmapheresis which would involve a large increase in the amount of donations collected from the Centre. Letter from Dr Lewis to Dr Cash 18 February 1981 p2 SBTS0000230_055
(1669) Expressed, for instance, by Dr Archibald McIntyre in a memo to Dr Bell 27 February 1981 SCGV0000082_039
(1670) Pilot study for large scale plasma procurement using automated plasmapheresis 16 April 1981p2 DHSC0002207_054. When cost was estimated later in 1981 by the working party, it concluded that the costs of plasmapheresis compared favourably with the estimated cost of obtaining the same weight of whole blood: £41-44 using manual pheresis; £50 per kg using machine pheresis; £56.55 for obtaining 1kg of whole blood. Working Party to Advise on Plasma Supplies for Self-sufficiency in Blood Products Preliminary Report June 1981 pp7-10 CBLA0001377. See the different views from regional transfusion centres in the chapter on Regional Transfusion Centres.
(1671) See, for instance, Mersey Regional BTS which opted against manual pheresis due to the problems associated with the need for continuous supervision, the time needed to complete a procedure and the need for temperature controlled centrifuges. This was despite the use of machines (£25,000 each to buy and run). Mersey Regional Health Authority Mersey Regional Blood Transfusion Service Report of the Director 22 February 1983 pp4-5 DHSC0002225_010
(1672) Plasma Supply – National Blood Transfusion Service11 April 1983 pp3-4 CBLA0001778. North London RTC was a pioneer in plasmapheresis, beginning with manual in 1967, later moving to machine; it had three plasmapheresis clinics. Professor Dame Marcela Contreras Transcript 2 December 2021 pp142-146 INQY1000165. By October 1987 the number of regular attenders exceeded 2,500, and over 80% of these donors attended for donation once a fortnight. Letter from Dr Contreras and others to the Editor of The Economist NHBT0086659. Yorkshire was also an early adopter of automated plasmapheresis, opening a centre in Bradford in 1982. By August 1983 there were 22 automated machines operating in Yorkshire RTC spread across three sites. Notes on visit to Yorkshire RTC 24 August 1989 pp1-2 NHBT0003366. However, Dr Jean Harrison (Director, North East Thames RTC) did not consider plasmapheresis an efficient way to collect plasma. Notes on visit to North East Thames RTC 2 August 1989 p1 NHBT0003370. She preferred to use recovered plasma because this was in her view a much cheaper way to reach her targets. Written Statement of Dr Jean Harrison paras 142-163, para 221 WITN7046001. At Newcastle, Dr Lloyd explained that initially he thought “the only way to get a major change in plasma production was to go full force into plasmapheresis … But once I got into the job … I realised we had a terrific opportunity to separate a lot more blood.” His RTC had a small plasmapheresis unit but mostly plasma was recovered from whole blood donations and by 1992/3 the Northern Centre was producing the third highest amount of plasma in England and Wales, behind North London and Yorkshire. Dr Huw Lloyd Transcript 8 February 2022 pp147-154 INQY1000182, Written Statement of Dr Huw Lloyd p34 WITN6935001
(1673) Glasgow and West of Scotland BTS Report to the Scottish Directors Source Plasma by Automated Plasmapheresis 20 April 1984 p4 SBTS0000238_104
(1674) Plasmapheresis now made up 11.2% of the plasma sent to BPL, having grown from 2,750kg in 1985 to 9,000kg in 1987. BPL and PFC Annual Report 1986/87 September 1987 p9, p13 CBLA0002371
(1675) Of course time expired plasma was not used to make factor concentrates: it was, however, of use for producing immunoglobulins and albumin.
(1676) Memo from Dr Smith to Dr Lane 29 April 1981 pp1-2 BPLL0007526
(1677) See the chapter on Organisation of the Blood Services.
(1678) The total spent (presuming regions spent their full allocations unless there is evidence they did not) was £270,865.29 of capital in 1975/76, and £192,144 of revenue in 1975/6. If the £58,000 that BPL received is included, this makes a total expenditure of 1975/6 of £501,009.29. These figures should be treated as approximations, though, as some regions included VAT in their calculations and others did not, and the final expenditures for some regions have not been found. Chronological Presentation on the Domestic Supply of Blood Products in England and Wales Appendix 3: The Expenditure of the £500,000 Special Allocation p70 INQY0000334
(1679) Northern, South East and South West Thames, Wessex, Mersey and North Western.
(1680) Draft letter from Mr Gidden to regional administrators 4 March 1975 DHSC0000935
(1681) Because instead of being used to produce cryoprecipitate locally it would now be sent to BPL to make concentrates instead.
(1682) Dr Murray of Newcastle RTC, wrote to Dr Maycock on 13 March 1975 saying he did not believe that clinicians would be satisfied with half the present amount of cryoprecipitate however much AHG was supplied. Letter from Dr Murray to Dr Maycock 13 March 1975 DHSC0002359_049. As to demand for cryoprecipitate growing see Minutes of Regional Transfusion Directors meeting 21 July 1976 pp6-7 NHBT0017095. On 11 July 1975 Dr Owen was provided with an update on what had been prolonged negotiations. He was told that the regions would produce the plasma required. They had finally come to terms with their allocations. Four centres required extensive alterations, taking between 6 and 21 months to achieve. Two regions had still not committed to providing plasma: Northern, and West Midlands. Memo from Donald Jackson to Michael Lillywhite 11 July 1975 DHSC0001774. The former was offered increased capital, and the latter an increased revenue allocation. Memo from P Lawrence to Donald Jackson 29 August 1975 DHSC0002177_094
(1683) Roughly one eighth of the money (£58,000) was allocated to BPL for the purchase of additional equipment. Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 p38 CBLA0000005_002
(1684) Letter from Thomas Dutton to Divisional Head (General Administration, North West Thames RHA) 21 June 1976 DHSC0103283_102
(1685) Chronological Presentation on the Domestic Supply of Blood Products in England and Wales Appendix 3: The Expenditure of the £500,000 Special Allocation p70 INQY0000334
(1686) Minutes of Regional Transfusion Directors meeting 6 October 1976 p5 NHBT0016475
(1687) Hansard written answers on Haemophilia 7 December 1978 HSOC0015198
(1688) BPL and PFL in Elstree and Oxford, England; PFC in Scotland.
(1689) It is unclear whether this includes an amount kept back for further testing and product development.
(1690) Appendix 4 Factor VIII: Capacity, Production and Demand 1973-1990 CBLA0000004_010
(1691) See the section in this chapter Introduction: leading up to 1973.
(1692) He moved from Edinburgh to Elstree in 1969. Gunson and Dodsworth Fifty Years of Blood Transfusion Transfusion Medicine 1996 p52 NHBT0000028
(1693) Note to Dr Maycock 30 June 1976 pp6-7 CBLA0002537. Dr Lane commented that the picture was of a facility which had some limited potential to improve production (if yield could be increased), but very little scope without further expenditure to manage a significant increase. Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 p48 CBLA0000005_002
(1694) Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 p48 CBLA0000005_002
(1695) Emphasis added. Report of Working Group on Trends in the Demand for Blood Products December 1977 p5 DHSC6887728_014
(1696) Minutes of Haemophilia Centre Directors meeting 13 January 1977 p16 PRSE0002268. Dr Lane did not believe SHHD’s claim. Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 pp55-56 CBLA0000005_002
(1697) Hansard written answers on Haemophilia 26 June 1978 DHSC0000291
(1698) Report to Advisory Sub-Committee on Blood Products and Blood Group Reference Laboratories of the Central Committee of NBTS September 1977 p12 CBLA0000664
(1699) Report to Advisory Sub-Committee on Blood Products and Blood Group Reference Laboratories of the Central Committee of NBTS September 1977 p8 CBLA0000664
(1700) This is, in essence, the principle that because the Crown (the State) conducts an operation, that operation may claim to be above the law which would apply only to operations not themselves conducted by the State. The Crown Proceedings Act 1947 made some modifications to that, but Crown immunity operated in particular in respect of the Health Service. Until waived, it meant that products from BPL did not require to be licensed by the Licensing Authority.
(1701) Report to Advisory Sub-Committee on Blood Products and Blood Group Reference Laboratories of the Central Committee of NBTS September 1977 p1 CBLA0000664
(1702) Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 p61 CBLA0000005_002
(1703) Evidence that the inspection was anticipated at this time was that reference was made to it in the annual report of BPL for 1976. Report to Advisory Sub-Committee on Blood Products and Blood Group Reference Laboratories of the Central Committee of NBTS 6 September 1976 p7 BPLL0001441, Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 para 112 CBLA0000005_002
(1704) See Lowe The Welfare State in Britain Since 1945 2005 pp317-318 RLIT0002232, Extract of Britton Macroeconomic Policy in Britain 1974-1987 1994 RLIT0002209, which records that there had been a significant expansion in the economy in the early 1970s, but that policy became contractionary in mid 1973, mainly affecting 1974-75. Public investment had been very heavy in the early 1970s, for instance, in extensive road building. It was cut very sharply back by governments of both political persuasions, though it was later to recover.
(1705) Extract of Public Policy and Economy Since 1900 1993 RLIT0002210
(1706) Written Statement of Dr Diana Walford paras D.5-D.6 WITN4461001
(1707) Minutes of NBTS meeting 25 October 1977 p1 CBLA0000682
(1708) Minutes of NBTS meeting 25 October 1977 pp1-2 CBLA0000682
(1709) By Department of Health and Social Care (“DHSC”) and NHS Blood and Transplant (“NHSBT”). Closing Submissions on behalf of the Department of Health and Social Care and associated bodies from the DHSC Legal Team 16 December 2022 para 1.22, para 2.70 SUBS0000057, NHSBT Closing Submissions to Infected Blood Inquiry 16 December 2022 para 2.3, para 6.22 SUBS0000062
(1710) Expert Report to the Infected Blood Inquiry: Public Health and Administration August 2022 p29 EXPG0000048, Written Statement of Peter Wormald para 14.11 WITN6934001, Written Statement of Dr Diana Walford para D.5 WITN4461001
(1711) Tomlinson Public Policy and the Economy Since 1900 1990 p321 RLIT0002210. See also: Crafts and Woodward The British Economy since 1945 1991 (in particular The British Economy since 1945: Introduction and Overview) and Hatton and Crystal The Budget and Fiscal Policy 1991, Cairncross The British Economy Since 1945 1995 (in particular The 1970s), Britton Macroeconomic Policy in Britain 1974-1987 1991 pp16-60 RLIT0002209, Clark and Dilnot The Cambridge Economic History of Modern Britain Volume 3 2004 (in particular British fiscal policy since 1939), Harris The Cambridge Economic History of Modern Britain Volume 2 2014 (in particular Health and Welfare) and Morys Cycles and depressions)
(1712) Whether to provide money or not is a choice – it can almost always be found if there is sufficient support for it.
(1713) Though the general financial position was “the elephant in the room”, there is no direct evidence that financial constraints were relied on at the time as a justification for not providing better facilities earlier than was done.
(1714) David Smart, who had valuable experience in the pharmaceutical industry, and became heavily involved in the redevelopment of BPL which later took place, considered that the capital cost would be recovered in around 15 months by the savings to be made if commercial products no longer need to be bought. Blood Products Laboratory: Redevelopment May 1979 p4 CBLA0001004_004
(1715) See for example Dr Maycock identifying in March 1973 that the requirement was for more than the fractionation capacity of the three plants after building operations were completed, even assuming some further increase in capacity. Present Sources of Materials for Treatment of Haemophilia and Potential Future Sources March 1973 DHSC0100005_132
(1716) Minutes of NBTS meeting 25 October 1977 p3 CBLA0000682
(1717) This is considered later in relation to safety.
(1718) Report to Advisory Sub-Committee on Blood Products and Blood Group Reference Laboratories of the Central Committee of NBTS p2 CBLA0000840
(1719) Dr Diana Walford Transcript 19 July 2021 pp166-167 INQY1000136
(1720) In a hand-over memo of August 1979, Dr Waiter said this: “It is accepted [ie by the DHSS] that in order to meet the anticipated demand for the principal plasma fractions (factor VIII and protein solutions – mainly albumin) new plant, in addition to that already available in the UK, must be acquired. With this in mind plans for the future development for the Blood Products Laboratory have been drawn up. In addition to increasing production it will be necessary to upgrade existing plant to meet the requirements of the Medicines Act. Needless to say any new plant will have to be built to the same specification.” Memo from Dr Waiter to Dr Ronald Oliver 23 August 1979 p1 CBLA0000042_105
(1721) Minutes of NBTS Scientific and Technical Committee for the Central Blood Laboratories meeting 26 March 1979 p3 BPLL0008430_001
(1722) Blood Products Laboratory: Redevelopment May 1979 p4 CBLA0001004_004
(1723) Dr Diana Walford Transcript 19 July 2021 p178 INQY1000136
(1724) Conclusions and Recommendations of Medicines Division DHSC0001812. The Report itself is BPL Inspection Report 23 July 1979 DHSC0002193_093
(1725) Minutes of NBTS Scientific and Technical Committee for the Central Blood Laboratories meeting 7 June 1979 p4 SBIN0000952
(1726) DHSS was divided into a number of divisions. Health Services dealt with policy issues. There was a general divide between the medical divisions, of which Dr Walford formed part and the administrative side which dealt with policy, and of which John Harley was part as an Assistant Secretary (senior civil servant, Grade 5). It was he who expressed the approach which the DHSS was taking to redevelopment.
(1727) This did not mean that no money was available for one or the other, but rather that a decision needed to be made as to which it would be. Letter from John Harley to Dr Lane 13 July 1979 CBLA0000955. The letter states: “It is, as you know, likely that a report by Medical Inspectors will require at the very least some up-grading of the facilities at the Blood Products Laboratory. You also know that no money has been allocated for this purpose. We do not of course know at the moment what the cost of up-grading may be, but we could find ourselves in a situation where we should have to choose between up-grading and going ahead with the ‘Stop-gap’ programme. I therefore think it would be advisable to avoid incurring any further Stop-gap expenditure until the financial position has been clarified. I need hardly say that this applies also to expenditure on the planning of the phased redevelopment of the BPL. I know what a disappointment this must be to you, but I’m sure you will agree it is the wisest course.” Dr Walford said: “even looking back on this as now I must, it’s really hard to understand why that instruction … was issued, because it did hold things up and it didn’t need to in my opinion.” Dr Diana Walford Transcript 19 July 2021 p188 INQY1000136
(1728) Conclusions and Recommendations of Medicines Division p2 DHSC0001812. The underlying report is: BPL Inspection Report 23 July 1979 DHSC0002193_093
(1729) This seems to be an acceptance that commercial products potentially carried significant risk to recipients, and that if the NHS had good production facilities, better and safer products than such alternatives could be achieved.
(1730) It observed this was “of very dubious comfort however, as we were advised that blood transfusions commonly cause side effects and it is unlikely that investigation would be pursued as to the precise cause.” It also added as a postscript that there were “serious doubts about the adequacy of measures intended to ensure staff safety [from the risk of hepatitis].” Letter from J Brown to Mr Williams 7 September 1979 pp2-3 DHSC0002195_077
(1731) Minutes of NBTS Scientific and Technical Committee for the Central Blood Laboratories meeting 26 September 1979 pp2-4 CBLA0001005
(1732) Memo from John Harley to Thomas Dutton 11 October 1979 DHSC0002195_050. He was a senior civil servant responsible for the section working on blood products policy.
(1733) This was already over two years since Roland Moyle, though re-affirming the policy of self-sufficiency, had recognised that BPL and PFL were already working to capacity, and the Trends Working Group had forecast significant increases in the demands which needed to be met.
(1734) Memo from Dr Harris to D Brereton and Zoe Spencer 21 December 1979 DHSC0002307_048, Submission to ministers on BPL p5 DHSC0002307_050
(1735) Memo from J Knight to Dr Harris 7 January 1980 DHSC0002307_047
(1736) Minutes of NBTS Joint Management Committee (DHSS/North West Thames RHA) for the Central Blood Laboratories meeting 20 February 1980 p3 CBLA0001068
(1737) Minutes of NBTS Joint Management Committee (DHSS/North West Thames RHA) for the Central Blood Laboratories meeting 20 February 1980 p3 CBLA0001068. Dr Lane proved to be more accurate.
(1738) Minutes of NBTS Scientific and Technical Committee for the Central Blood Laboratories meeting 23 April 1980 p3 CBLA0001093. See also Letter from Dr Lane to John Harley 22 May 1980 p1 CBLA0001107
(1739) MARP stands for Medicines Act Rehabilitation Project. Essentially, this was to remedy the specific defects the Inspectorate had identified, but not providing any further funds for increasing production. Letter from Dr Lane to John Harley 22 May 1980 CBLA0001107
(1740) Note of meeting to discuss expenditure on the upgrading of BPL 11 June 1980 p1 CBLA0001112
(1741) Memo from J Knight to Peter Wormald 29 July 1980 DHSC0002307_023, Memo from Peter Wormald to J Knight 24 July 1980 WITN4461036
(1742) North West Thames Regional Health Authority. Letter from Gordon Collins to Dr Lane 2 February 1981 CBLA0001256, Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 pp115-116 CBLA0000005_002
(1743) Minutes of NBTS Scientific and Technical Committee for the Central Blood Laboratories meeting 23 January 1980 p2 CBLA0001052
(1744) Note of meeting on the future of BPL 21 March 1980 p1 DHSC0002307_041
(1745) Dr Diana Walford Transcript 20 July 2021 p44-45 INQY1000137
(1746) Minutes of NBTS Scientific and Technical Committee for the Central Blood Laboratories meeting 17 September 1980 CBLA0001171
(1747) Submission to ministers on BPL’s possible takeover by industry SCGV0000127_025
(1748) Memo from Dr Walford to John Harley 15 September 1980 p1 WITN0282008
(1749) Memo from Peter Wormald to T Nodder, Dr Harris and J Knight 14 November 1980 p2 DHSC0002307_069. Peter Wormald was the Under-Secretary in charge of the DHSS Health Service Division (1978-81).
(1750) DHSS Press Release No Commercial Management of Blood Products Laboratory 25 November 1980 p1 WITN4461107. It was not accurate to describe this as “bringing in commercial management” when the possibility under consideration was not simply providing different managers but had been the replacement of BPL by a commercial enterprise. Dr Diana Walford Transcript 20 July 2021 p68 INQY1000137
(1751) Memo from J Knight to John Harley 8 January 1981 WITN4461046
(1752) Dr Dunnill was a member of the Scientific and Technical Committee who had written in confidence to Dr Vaughan, noting that he had been part of a US task force that undertook a review of fractionation worldwide for the US National Institutes of Health and saying: “I have been told verbally that you accept responsibility. Unfortunately that does not reduce my ethical responsibility as a chartered engineer and scientist and I have accepted the situation in the short term only from consideration of the need to maintain plasma fraction supply.” Letter from Dr Dunnill to Dr Vaughan 13 May 1980 pp10-11 WITN4461048
(1753) Dr Diana Walford Transcript 20 July 2021 p76 INQY1000137
(1754) Minutes of Policy Steering Group for the Redevelopment of BPL meeting 19 October 1981 CBLA0001474
(1755) Minutes of Joint Management Committee (DHSS/North West Thames RHA) for the Central Blood Laboratories meeting 23 October 1981 p4 DHSC0002211_063
(1756) David Smart’s view is recorded in the Minutes of Joint Management Committee (DHSS/North West Thames RHA) for the Central Blood Laboratories meeting 23 October 1981 p3 DHSC0002211_063: “[The Policy Steering Group’s] work was hampered to an extent by the lack of Ministerial decision on long-term management arrangements”.
(1757) Minutes of Policy Steering Group for the Redevelopment of BPL meeting 1 March 1982 p2 DHSC0002215_087
(1758) An Appraisal of Redevelopment Options for the Blood Products Laboratory p9 CBLA0001606
(1759) It had by now been three and a half years since the inspection by the Medicines Inspectorate condemning BPL’s facilities. Memo from Stanley Godfrey to John Harley and Janet Walden 22 September 1982 DHSC0002309_017
(1760) Letter from Jeremy Colman to Douglas Harris 11 November 1982 DHSC0002319_013
(1761) Dr Diana Walford Transcript 20 July 2021 pp91-92 INQY1000137. It may be that the failure to have a more independent management structure prior to this was a contributory reason to the delays which had occurred.
(1762) Conclusions and Recommendations of Medicines Division pp2-4 DHSC0001812
(1763) Minutes of NBTS Scientific and Technical Committee for the Central Blood Laboratories meeting 23 January 1980 p2 CBLA0001052, Letter from J Brown to Mr Williams 7 September 1979 DHSC0002195_077, Submission to ministers on BPL DHSC0002307_050. Part of the flexibility was waiting to make changes while a decision was being taken as to the long term future of BPL.
(1764) Phased Redevelopment of Blood Products Laboratory Requirements for Capital Planning4 February 1986 p4 CBLA0002298
(1765) Position Paper on the Construction of the New Blood Products Laboratory 12 June 1986 p1 DHSC0002303_018
(1766) Hansard written answer on Blood Products 28 November 1984 DHSC0002251_014
(1767) Hansard written answer on National Blood Transfusion Service: Factor VIII 19 February 1985 DHSC0003997_073
(1768) Written Statement of Lord David Owen paras 42-43 WITN0663001
(1769) Memo from Malcolm Harris to Strachan Heppell 29 December 1986 pp1-2 WITN0771066. From the data set out in figure 1 it can be seen it was not achieved until around 1990.
(1770) Memo from Gwen Watson to Strachan Heppell 13 August 1986 WITN0771060
(1771) Memo from Michael O’Connor to Strachan Heppell 14 August 1986 WITN0771061
(1772) Written Statement of Lord Norman Fowler para 4.82 WITN0771001
(1773) Lord Norman Fowler Transcript 21 September 2021 pp117-118 INQY1000144
(1774) Written Statement of Lord Norman Fowler para 4.82 WITN0771001
(1775) Letter from Christopher France to J A Doran 7 November 1984 DHSC0003964_029, Written Statement of Lord Norman Fowler para 4.83 WITN0771001
(1776) Memo from Malcolm Harris to Strachan Heppell 29 December 1986 p2 WITN0771066
(1777) Written Statement of Lord Norman Fowler para 4.61 WITN0771001
(1778) Lord Norman Fowler Transcript 21 September 2021 pp116-118 INQY1000144, Written Statement of Lord Norman Fowler para 4.81 WITN0771001
(1779) Note on Central Committee for the National Blood Transfusion Service meeting October 1976 pp2-6 DHSC0002181_045
(1780) Hansard written answers on Haemophilia 26 June 1978 p1 DHSC0000291
(1781) A target which, according to Thomas Dutton’s minute of 1976, had long since been recognised as too low. Note on Central Committee for the National Blood Transfusion Service meeting October 1976 p2 DHSC0002181_045
(1782) Dr Diana Walford Transcript 20 July 2021 pp1-2 INQY1000137
(1783) Dr Diana Walford Transcript 20 July 2021 p3 INQY1000137
(1784) Written Statement of Peter Wormald para 5.1 WITN6934001
(1785) It is in general desirable to use blood as locally as possible to its source, since the prevalence of diseases will vary from territory to territory, and with that, often the ability of the population within a territory to have greater resistance to such an infection than if the infection is newly introduced.
(1786) As they understood them from practical experience as users: they were in general not told sufficient about the attendant risks to be in a position to make a properly informed choice. See the observations of Mr M who gave evidence in Leeds. Mr M Transcript 14 June 2019 pp9-15 INQY1000020
(1787) Dr Diana Walford Transcript 20 July 2021 p76 INQY1000137
(1788) Dr Diana Walford Transcript 20 July 2021 p29 INQY1000137
(1789) And whether or not product was manufactured in the UK or had to be purchased from abroad, the latter being seen at the time as a very expensive option.
(1790) This is considered more fully below.
(1791) Closing Submissions on behalf of the Department of Health and Social Care and associated bodies from the DHSC Legal Team 16 December 2022 para 2.53 SUBS0000057
(1792) From Figure 3 of this chapter it can be seen that the upper estimate of the MRC Working Party would, if met, have been sufficient to cater for the whole usage of Factor 8 in England and Wales until 1980.
(1793) Closing Submissions on behalf of the Department of Health and Social Care and associated bodies from the DHSC Legal Team 16 December 2022 paras 2.54 - 2.74 SUBS0000057
(1794) SNBTS Plasma Fractionation in Scotland 2008 p1 PRSE0001732
(1795) See in particular Extract from Minutes of Technical Committee of the Blood Transfusion Service meeting 5 April 1949 SCGV0001182_310, Letter from Drummond Ellis to Dr Smith 17 December 1954 SCGV0001182_173, Letter from Dr Cumming to Dr Gordon 28 June 1957 pp2-3 SCGV0001182_081, leading to Letter from SHHD to Dr Maycock 4 February 1965 SBTS0000284_060, Letter from Dr Cumming to Dr Biggs 14 December 1967 OXUH0003778_008
(1796) As well as other plasma derivatives. Letter from Dr Maycock to Elisabeth Hirst 17 February 1965 p1 DHSC0103209_177, Blood Transfusion Public Expenditure Survey Committee Report 13 April 1965 SCGV0001192_005
(1797) Protein Fractionation Centre Liberton and the arrangements with the NBTS (undated) DHSC0003715_171
(1798) Letter from Dr Maycock to Elisabeth Hirst 27 March 1969 DHSC0103209_151
(1799) The “Joint” in the title represents the combination of England (with Wales) and Scotland.
(1800) Minutes of Joint Steering Committee on Blood Products Production meeting 20 June 1973 p2 PRSE0004359
(1801) Letter from John Brotherston to Dr Reid 31 January 1974 DHSC0103209_086. His letter goes on to say: “Granted that we would not want to withhold demonstrably better treatment from patients, nor to place unreasonable constraints on clinicians as to which therapeutic agents they should use, the most obvious way of stemming the trend towards trade in human blood products is to try to meet all reasonable needs through the Blood Transfusion Services. Here is the rub. The Blood Transfusion Service in Scotland has consistently planned to provide substantially greater quantities of blood products per head of population than the Service in England. The quantities proposed in Scotland have sometimes initially seemed fairly liberal, but where events have overtaken us, as in the case of Factor VIII, have proved to be about right. The implications of these levels of production have been known to our Regional Directors for some time and they are confident that there will be a sufficient supply of plasma available to meet them. While we are by no means complacent, we believe that once the new Protein Fractionation Centre at Liberton goes into production later this year we shall be able to supply virtually all Scotland’s needs for blood products.” Emphasis added. So it proved. For those prepared to listen, this letter could be seen as one from a critical friend and knowledgeable observer adding weight to calls in the early 1970s to provide adequate production facilities at BPL.
(1802) Eight litres would equal the product of approximately forty donations. Minutes of Edinburgh Regional Blood Transfusion Centre meeting 9 May 1968 p2 WITN3530076
(1803) This was said to be within the estimated maximum capacity of the plant as envisaged.
(1804) At this stage, therefore, agreement on a fully collaborative approach. Minutes of Edinburgh Regional Blood Transfusion Centre meeting 9 May 1968 p4 WITN3530076
(1805) Letter from Andrew Mitchell to Malcolm Widdup 30 May 1968 DHSC0103209_172
(1806) Minutes of Blood Products Laboratory meeting 1 November 1968 p1 WITN3530077
(1807) Anglo-Scottish Cooperation in Blood Products Production p1 DHSC0103209_026
(1808) Minutes of Edinburgh Regional Blood Transfusion Centre meeting 14 March 1969 p2 PRSE0002199
(1809) Letter from W Lawrie to J Patterson 2 December 1969 p5 DHSC0103209_139, Letter from J Patterson to W Lawrie December 1969 DHSC0103209_140
(1810) Written Statement of Dr Peter Foster pp23-24 WITN6914001
(1811) Minutes of Expert Group on the Treatment of Haemophilia meeting 20 March 1973 p4 PRSE0004706, Minutes of Joint Steering Committee meeting on 20 June 1973 CBLA0000152. PFC, once operational, would play a key role in UK wide production of blood products.
(1812) Of this plasma, it was expected, at the 1,500 litre level, to process 200 litres of fresh plasma with the balance being outdated or partly aged plasma. At the level of 3,000 litres per week, it was expected that 1,000 litres would be provided as fresh plasma. The plasma was expected to come on a contract basis.
(1813) 1975
(1814) Letter from John Watt to Dr Jack O’Riordan 11 November 1975 p1 WITN6914007
(1815) Dr Peter Foster Transcript 24 March 2022 p114 INQY1000197. Dr Peter Foster was the head of the R&D Department at PFC (1974-2009).
(1816) Letter from Thomas McLean to M Draper 11 August 1975 SCGV0000074_010
(1817) Letter from M Draper to Thomas McLean 7 November 1975 SCGV0000074_007
(1818) Minutes of DHSS meeting 11 March 1976 p2 CBLA0000343
(1819) Minutes of Haemophilia Centre Directors meeting 13 January 1977 p16 PRSE0002268. Dr Lane later asserted that the SHHD figure “was nonsense, but was not apparently challenged”. Draft Proof of Evidence of Dr Lane for HIV Haemophilia Litigation 10 December 1990 para 137 CBLA0000005_002
(1820) Minutes of SNBTS Directors meeting 12 July 1977 p3 PRSE0004548
(1821) There was nonetheless a proposal that PFC should fractionate a limited amount of the English plasma for around two weeks, to establish yield and costs. This would be carried out on the basis of an extended working day, pending possible agreement on shift working. Minutes of SNBTS Directors meeting 17 January 1978 pp1-2 PRSE0004707
(1822) By June 1978, a fifth of the stored plasma had been processed. John Watt attempted to process more without shift working but this was unsuccessful. Letter from John Watt to Dr Bert Bell 7 June 1978 DHSC0003715_155
(1823) These blood products would largely be immunoglobulins and albumin at that stage.
(1824) Which was purely English and Welsh.
(1825) The DHSS had budgeted to pay Scotland for the extra costs of processing “about 30,000 bottles of plasma protein fraction and anti-haemophilic globulin from 10,000 bottles of blood” annually for the four years 1975/6 - 1978/9, “But because no plasma was fractionated at PFC the money was used instead to fund BPL activities. Even the 1978/79 allocation has already been earmarked for BPL purposes at Elstree and will in fact need to be spent for these purposes.” Protein Fractionation Centre Liberton and the Arrangements with the NBTS DHSC0003715_171
(1826) Letter from Dr Maycock to Thomas Dutton 26 July 1977 DHSC0003715_194
(1827) This is not, and has no direct connection with, Factor 8.
(1828) Minutes of Joint DHSS/SHHD meeting 22 August 1977 p1 SBTS0000283_006
(1829) The minutes record that PFC had been planned to cater for plasma products for England. Thus, both SHHD and DHSS were answerable to ministers for making the best and most economic use of the facility. It was reported to the meeting that the combined capacity of BPL/PFL and PFC was approximately 34 million international units which was “well on the way towards the 50 million seen as the minimum national requirement.” Minutes of Joint DHSS/SHHD meeting 22 August 1977 pp2-3 SBTS0000283_006. Of that, Dr Maycock estimated BPL/PFL’s contribution at about 17.5 million international units per annum (roughly half). Minutes of DHSS/SHHD Joint meeting 22 August 1977 DHSC0003733_045. There were problems in arranging continuous 24 hour production at PFC, using shift work, because the NHS working arrangements were subject to regulation by Whitley Council terms and conditions. These did not allow for overtime payments for unsociable hours/night shift working. The trade union was not prepared to agree that its members should work night shifts without the additional payments they might expect in other employments. A possible compromise was proposed by which PFC might be taken out of the scope of the Whitley Council arrangements by regarding it as a pharmaceutical factory type development. In the event, this did not happen. Note of Joint DHSS/SHHD meeting 22 August 1977 p2 WITN6914043, Written Statement of Dr Peter Foster para 66.3 WITN6914001, Dr Peter Foster Transcript 24 March 2022 pp119-124 INQY1000197
(1830) Letter from John Watt to Robert Roberts 22 September 1977 p1 SBTS0000284_041
(1831) Letter from John Watt to Robert Roberts 22 September 1977 p3 SBTS0000284_041
(1832) Letter from David Stevenson to A Eason 28 October 1977 SCGV0000001_184
(1833) Letter from Alec Parrott to Susan Maunsell 1 November 1977 DHSC0003715_176
(1834) Hansard written answers on Haemophilia 26 June 1978 p1 DHSC0000291
(1835) He described John Watt’s views as to the yield he anticipated as being “frankly, ludicrous on any view”; that where it came to Scotland he was “again trying to go one better” by suggesting that Scottish product was likely to be cheaper than BPL product and that the decision to redevelop BPL was “not helped by exaggerated claims made by the Director of PFC Liberton [ie John Watt] for its operational capacity.” Draft Proof of Evidence of Dr Lane for HIV Haemophilia Litigation 10 December 1990 p47 CBLA0000005_002. His view was “that there appears to be a disproportionate amount of money spent on the Scottish Blood Transfusion Service, and this discrepancy in funding is exemplified on page of the submission. In 1975/76, expenditure on the National Blood Transfusion Service in England and Wales … £15.8 million for a population of some 49 million, compared with expenditure of £3.5 million in Scotland, where the population was only 5.5 million.” Draft Proof of Evidence of Dr Lane for HIV Haemophilia Litigation 10 December 1990 p58 CBLA0000005_002
(1836) See Memo from Dr Archibald McIntyre to Angus Macpherson 24 September 1980 SCGV0000127_039
(1837) Written Statement of Peter Wormald paras 43.6-43.8 WITN6934001
(1838) Written Statement of Peter Wormald para 43.9 WITN6934001. In May 1980 Mr Wormald took an opportunity to discuss this with A Macpherson of SHHD, and on 2 June 1980 wrote him a lengthy letter. In principle, he favoured expansion of PFC as well as rebuilding Elstree, so as to “secure something approaching an equal division of output between the two”, but noted “this view may not be shared by other English interests”. Letter from Peter Wormald to A Macpherson 2 June 1980 DHSC0002313_044
(1839) Memo from Dr Walford to John Harley 15 September 1980 WITN4461069
(1840) Notes on Feasibility Exercise Performed at Protein Fractionation Centre Liberton 15 December 1981 CBLA0001528
(1841) Blood products – the battle against private interests goes on October 1981 SBTS0001455_012
(1842) Letter from John Watt to Robert Roberts 22 September 1977 p3 SBTS0000284_041
(1843) He described how there was a sequence of three precipitation steps. The equipment needed for each was fitted into a module. Written Statement of Dr Peter Foster para 66.1 WITN6914001. In oral evidence he described that “there were what I called upstands in this process cold room – which had provision of services where you could plug in the module, plug it into the computer, into power supplies, into supplies of ethanol and so on and each module would obtain these supplies from the basement … and each upstand could accommodate two modules … There were 7.5 upstands so there was room for 15 modules. But to meet Scotland’s needs, we actually needed to run three modules on a nine-to-five working day. One of the reasons for that was that when I redesigned John Watt’s process, I was able to increase the throughput by a factor of three. So, in fact, it became even more productive than he had designed it. And because we’d been initially supplied with enough modules to handle Scotland, we’d been given six modules but we only needed three on a nine-to-five basis until 1984, and then we brought the other three into use, and we ran six modules on a nine-to-five basis. But we never used the full capability of a system on a 24-hour basis other than for a short shift experiment.” In short, after the redesign which Dr Foster oversaw, which he described had enabled the plant to have a flow-rate of 45 litres per hour rather than the 15 litres per hour initially achieved, the plant had potential to produce five times as much as was needed for Scotland, provided that sufficient storage and warehouse facilities and staffing were made available. Dr Foster gave the figure of 400,000 litres per annum if nine modules were operated fully continuously. Dr Peter Foster Transcript pp47-48 INQY1000197
(1844) A common pattern of work at the time in many productive industries.
(1845) There were otherwise not enough trained staff to cope with three eight-hour shifts. Notes on Feasibility Exercise Performed at Protein Fractionation Centre Liberton 15 December 1981 pp1-2 CBLA0001528
(1846) Production Manager, BPL.
(1847) Five days at 24 hours: this was the period for which David Wesley had observed the operation. Notes on Feasibility Exercise Performed at Protein Fractionation Centre Liberton 15 December 1981 p5 CBLA0001528
(1848) These were the two weeks earmarked for the operation of the CSVM plant in production: the other weeks were given to the preparatory stages and post-production stages which are a necessary part of overall production.
(1849) Notes on Feasibility Exercise Performed at Protein Fractionation Centre Liberton 15 December 1981 p7 CBLA0001528
(1850) Minutes of Policy Steering Group for the Redevelopment of BPL meeting 18 December 1981 p2 CBLA0001517
(1851) Letter from Professor John Cash to Hamish Hamill 11 January 1990 SBTS0000187_047
(1852) He acknowledged, however, that based on the trial it would have been necessary to complete additional works before the product could be produced in sufficient quantity for the whole of England.
(1853) It had apparently been produced, but as part of normal production, not as part of the trial.
(1854) Draft Proof of Evidence of Dr Richard Lane 10 December 1990 para 292 CBLA0000005_002
(1855) Letter from Angus MacPherson to John Harley 11 January 1982 CBLA0001532
(1856) Letter from John to Angus Macpherson 4 March 1982 SCGV0000002_024
(1857) Letter from John Walker to John Cashman 15 September 1982 DHSC0002333_018
(1858) This seemed to Dr Walford to be “a sort of bitter blow”.Dr Diana Walford Transcript 20 July 2021 pp104-105 INQY1000137
(1859) Briefing on Blood Products Laboratory Redevelopment January 1982 WITN6914044
(1860) Memo from Stan Godfrey to John Harley and Janet Walden 22 September 1982 WITN4461060
(1861) Briefing on Blood Products Laboratory Redevelopment January 1982 p3 WITN6914044
(1862) Dr Peter Foster Penrose Inquiry Transcript 10 May 2011 p81 PRSE0006022
(1863) Written Statement of Dr Peter Foster 7 March 2022 pp155-157 WITN6914001
(1864) The options were said to be £18.6 million if BPL were to process 200,000kg per annum, as contrasted with £21.03 million for 400,000kg (the option eventually chosen). Blood Products Laboratory: Redevelopment 1 January 1982 p2 DHSC0002309_108
(1865) Written Statement of Dr Peter Foster p156 WITN6914001
(1866) As it happened, the construction costs of BPL eventually were around three times as much as the £21.03 million first estimated. He also pointed out that land was known to have been readily available at Liberton upon which any extension needed to the PFC buildings could have been erected. Written Statement of Dr Peter Foster p156 WITN6914001
(1867) Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 p61 CBLA0000005_002
(1868) ie one fractionating 200,000kg rather than 400,000kg per annum.
(1869) Written Statement of Dr Peter Foster p158 WITN6914001
(1870) Had there been sufficient plasma fractionated by BPL in 1973 to 1975 to meet the demands of haemophilia clinicians at that time, it is difficult to think that regional treasurers would have funded any significant purchases of commercial product.
(1871) By contrast, the expense of commercial products was met as a recurrent expense to be met largely by the regions and so only indirectly by the government. It was not a one-off capital commitment, which would have to be met directly by the government.
(1872) Two examples of this: the first is Professor Edward Tuddenham who expressed this view in 1987. Commenting on a legal opinion to the Haemophilia Society, he wrote: “Would the provision of home produced concentrate have reduced the number of HIV infected patients? The answer here must very clearly be ‘yes’ despite the over-cautious remarks of Professor Bloom in his Lancet editorial of 1984. He would himself now I am sure agree that we would have half or less of the antibody positive cases that we have now had UK Factor VIII sufficiency been reached in 1977 as promised by the Government of the day.” Letter from Professor Tuddenham to David Watters 5 March 1987 HSOC0029583. He was asked in his oral evidence to the Inquiry: “Does that remain your view?” He answered “Yes.” Professor Edward Tuddenham Transcript 22 October 2020 p142 INQY1000067. The second is Professor Michael Makris: “I believe that, had the UK been self-sufficient in concentrates, the number of HIV infections in haemophilia patients would have been a lot less. The main reason I say this, is the low prevalence of HIV infection in the UK blood population during the 1980-1984 period.” Written Statement of Professor Michael Makris para 38.3 WITN4033001. These views are consistent with the repeated views of the UK Haemophilia Centre Doctors’ Organisation in calling for self-sufficiency and comparing commercial concentrates unfavourably with NHS concentrates with respect to rates of infection, and the position of The Haemophilia Society. See the chapters on Haemophilia Centres: Policies and Practice and Haemophilia Society.
(1873) Written Statement of Dr Morris McClelland para 11 WITN0892006
(1874) The Belfast Centre was included in the UKHCDO Oxford supra-region until 1981. Counsel Presentation on Belfast Haemophilia Centre March 2021 para 5 INQY0000246, Minutes of UK Haemophilia Centre Directors meeting 26 February 1980 p6 HCDO0000405
(1875) Written statement of Dr Morris McClelland para 7b WITN0892001
(1876) Table 5.3.1 showing annual consumption of CFC 1976 to 1994 WITN3826017
(1877) Dr Morris McClelland Transcript 1 February 2022 pp56-57 INQY1000179
(1878) Written Statement of Dr Morris McClelland para 10 WITN0892006
(1879) Some commercial concentrates were used in Scotland, in particular at Yorkhill Hospital for the treatment of children with haemophilia – but that usage largely reflected the choice of the clinicians rather than a lack of domestic product.
(1880) Cumming The Voluntary Blood Donor 1975 p7 SBTS0000605_005
(1881) Written Statement of Dr James Smith paras 164-165, 168 WITN3433001. Dr Smith was chief chemist at PFC in Edinburgh (1968-1975) and then scientist in charge of fractionation at PFL in Oxford (1975-1992) and also head of coagulation factor production at BPL in Elstree (1979-1982).
(1882) Dr Terence Snape Transcript 30 March 2022 p174 INQY1000200
(1883) Lord David Owen Transcript 22 September 2021 p162 INQY1000055
(1884) Which is why he had to ask to see a copy, as described in the text.
(1885) Chiron clones Hepatitis Non-A, Non-B Virus which may allow screening for previously undetectable disease 10 May 1988 NHBT0000072_006
(1886) Testing for non-specific markers was possible. See the chapter Hepatitis C Surrogate Screening.
(1887) Serum hepatitis was understood to be viral, but it was possible that more than one virus might cause it. Though this possibility became known as a probability in the early 1970s some voices had suggested it before Hepatitis B became recognisable.
(1888) This did not apply to all proteins in the blood. Factor 8 could be more easily destabilised by heat than albumin could be. The principal challenge in applying heat to Factor 8 concentrates was that the levels of heat necessary to destroy the virus were for a long time thought likely also to destroy or inactivate the Factor 8 protein itself, which was regarded as a “labile” protein, so that heat treatment was thought to be self-defeating.
(1889) By the appropriately named Dr Murray Luck. SNBTS Briefing Paper on the Development of Heat Treatment and Coagulation Factors November 2010 p11 PRSE0002291
(1890) SNBTS Briefing Paper on the Development of Heat Treatment and Coagulation Factors November 2010 p11 PRSE0002291. It proved effective at the time even though over 20 years was to pass before tests were available to identify the presence of Hepatitis B in blood, and over 40 before tests could show the presence of Hepatitis C.
(1891) Gunson et al Fifty Years of Blood Transfusion Transfusion Medicine 1996 p47 NHBT0000028
(1892) World Health Organization Expert Committee on Hepatitis March 1952 p19 RLIT0000215. This section of the WHO Expert Committee report refers back to an earlier section in which it is clear that observation showed that serum hepatitis was inactivated by heating human albumin at 60°C for ten hours, but not for one hour. World Health Organization Expert Committee on Hepatitis March 1952 p10 RLIT0000215
(1893) There is an intermediate form, in which a solvent is added to dried concentrate before it is heated; and one system used a steam spray.
(1894) In Commercially obtained blood and serum hepatitis, published in 1970, he showed that the hepatitis risk from commercially obtained blood was markedly higher than that of blood from unpaid donors. He observed that the enormous differences between the safety of blood from volunteers and that commercially obtained “have been repeatedly pointed out by this laboratory during the past decade”. Garrott Allen Commercially Obtained Blood and Serum Hepatitis Surgery, Gynecology and Obstetrics August 1970 p3 RLIT0002180. See also Garrott Allen Our Commercial Blood Program and Serum Hepatitis Annals of Surgery November 1970 RLIT0002194, Walsh et al Posttransfusion Hepatitis After Open-Heart Operations Journal of the American Medical Association 12 Jan 1970 RLIT0000073. Richard Titmuss in his book, The Gift Relationship, made a point of these risks in his critique of the commercial market in blood and blood products. Titmuss The Gift Relationship 1970 pp142-157 HSOC0019917
(1895) It seems unlikely to have been a desire to prevent other commercial companies stealing a march on it, because at this stage pharmaceutical sales of factor concentrates were growing almost exponentially across the world, and any challenge to market share of any individual major producer was likely to arise only in the longer term. It might have been because Cutter were concerned they might lose market share if their products were identified as particularly likely to lead to hepatitis. Professor Garrott Allen wrote to say as much to Dr William Maycock on 6 January 1975, beginning: “As you know” Cutter’s Konyne (sourced “100 percent from Skid-Row derelicts”) was “extraordinarily hazardous”. He claimed that there was a 50-90% rate of icteric hepatitis developing from it. Also, half if not more of post-transfusion hepatitis was being caused by an agent which was neither Hepatitis A nor Hepatitis B. Letter from Professor Garrott Allen to Dr Maycock 6 January 1975 p1 CBLA0000249. Dr Milton Mozen, director of Biochemical Research and Development at Cutter, said that “Concern about hepatitis transmission” was the reason for experiments with heat treatment in the early 1970s. Deposition of Dr Milton Mozen 2 May 1989 p102 MULL0000567_007
(1896) Biochemical Research Department Quarterly Progress Report 1972 p3 BAYP0003708
(1897) The use of the names “Armour”, “Cutter”, “Travenol”, “Baxter”, “Hyland”, “Immuno” and “Alpha” are for easy readability. It should be remembered that the licensing, supply and distribution of blood products in the UK from commercial companies was through UK companies which were different corporate entities. See the preface to the chapter on Pharmaceutical Companies.
(1898) In the memo the observation was made, summarising the 1972 work by Dr Wada, that “We have already shown with model viruses that dry heat at 60° for 48 hours is equivalent for Konyne with wet heat at 60° for 10 hours. We expect that a total of six-nine months will be necessary to take us to approval [by the Bureau of Biologics].” Letter from Dr Sternberg to Dr Schaeffler and others 24 May 1983 p3 CGRA0000412
(1899) Dr Duane Schroeder and Dr Mozen. Shohachi Wada Transcript in US litigation 16 March 1995
(1900) Shohachi Wada Transcript in US litigation 16 March 1995 p19 JEVA0000104
(1901) Shohachi Wada Transcript in US litigation 16 March 1995 p11 JEVA0000104
(1902) Shohachi Wada Transcript in US litigation 16 March 1995 p19 JEVA0000104
(1903) They were model viruses: bovine rhinotracheitis and blue tongue; neither was hepatitis.
(1904) Shohachi Wada Transcript in US litigation 16 March 1995 p26 JEVA0000104
(1905) The time he spent was as directed by his senior managers, and not at his own discretion. Shohachi Wada Transcript in US litigation 16 March 1995 p21 JEVA0000104
(1906) Shohachi Wada Transcript in US litigation 16 March 1995 p22 JEVA0000104
(1907) The Guardian Drug could aid clotting 24 May 1966 MDIA0000001
(1908) Weinberg and Shaw Blood on their hands 2017 pp121-123 RLIT0002228
(1909) DePrince Cry Bloody Murder, A Tale of Tainted Blood 1997 p33 MULL0002367. A similar account is given by Douglas Starr who comments: “Once AIDS became an acknowledged reality, the drug firms quickly developed screening tests and virus-killing technologies … If they had heeded the warnings of Factor VIII pioneer Ed Shanbrom and others who issued early warnings about viruses, they would have abandoned the high-risk collection centers sooner and worked more intensively on virus-killing technology.” Starr Blood, An Epic History of Medicine and Commerce 1998 p361 HSOC0019915
(1910) The Advocate Researcher says firms rejected virus preventer 7 June 1993 p2 CGRA0000496_005
(1911) Constitutionally therefore not itself part of the NHS, but independent of it, though producing blood products for the NHS without charge from plasma supplied to it by the NHS, again without charge.
(1912) Written Statement of Dr Peter Foster para 43.1(ii) WITN6914001. See also: Memo from Milt Mozen Visit to SNBTS PFC 4-5 August 1975 pp2-3 BAYP0003775
(1913) eg by forms of filtration.
(1914) Gerety and Barker Viral Antigens and Antibodies in Hemophiliacs Food and Drug Administration 1976 p4 BAYP0000020_004. This suggests that from the mid 1970s interest had begun to pick up amongst commercial manufacturers.
(1915) Who was later to receive the Nobel prize for his work in relation to Hepatitis C.
(1916) Emphasis added. Alter How Frequent is Posttransfusion Hepatitis after the Introduction of 3rd generation Donor Screening for Hepatitis B? What is its Probable Nature? Vox Sanguinis 1977 p2 NHBT0000092_002
(1917) Written Statement of Professor Michael Makris para 38.17 WITN4033001
(1918) Dr Spero was a haematologist at the University of Pittsburgh. Spero et al Asymptomatic Structural Liver Disease in Hemophilia New England Journal of Medicine 22 June 1978 p6 PRSE0002523
(1919) Memo from Lee Kriley to Distribution 14 June 1979 p2 CGRA0000220
(1920) February 1979. Memo from Robert Taub to H Terreer and others 2 February 1979 p2 CGRA0000218. This inferentially supports the section above on the Early 1970s to the effect that pharmaceutical companies had little commercial incentive in the early 1970s to conduct research into making their products free from hepatitis because they could sell all or most of what they could produce without the complications of doing so. It would demand some expenditure or research, together with marketing costs, and it might be expected to reduce the yield from each batch of plasma, in effect causing raw materials costs to rise as a proportion of the costs of a product.
(1921) Memo from Lee Kriley to Distribution 14 June 1979 p3 CGRA0000220. Improving patient safety is not explicitly mentioned, but is the underlying context for expecting these commercial results.
(1922) Memo from Lee Kriley to Distribution 14 June 1979 p2 CGRA0000220
(1923) Dr Ernst Weidmann, the Behringwerke clinical research project manager: Ernst Weidmann Transcript in Anon and Others v Alpha Therapeutic Co and Others 4 November 1993 p696 MULL0000269
(1924) Described as “all sorts of experiments”by Dr Victor Cabasso, Cutter Director of Research and Development. Deposition of Dr Victor Cabasso in Factor VIII or IX Concentrate Blood Products Litigation 29 March 1995 pp148-150, pp151-155 MULL0000143. Although he said this in American litigation against the firm, Cutter’s lawyers were unable to document the work actually done between 1972 and 1978, so what he was describing is probably best seen as describing an approach to improving products across the board. It was in 1978 that Cutter extended its research, and then identified stabilising compounds which would permit the heating of Factor 8 to a temperature of 60°C for ten hours without losing unacceptably high levels of clotting activity. Expert report of Dr Milton Mozen 5 October 1994 p23 WITN6407003
(1925) Foster and Bienek Fractionated Products Transfusion Microbiology 15 February 2008 p13 WITN6914003. Peter Fernandes Transcript in Anon and Anon v Armour Pharmaceutical Corp et al 12 and 13 February 1997 p50, p82, p88, p95 MULL0000005
(1926) Expert report of Dr Milton Mozen 5 October 1994 p20 WITN6407003
(1927) As the later US Institute of Medicine Committee report noted: “the very nature of the competitive world of business is one that normally would cause a company to preserve manufacturing processes and research results for its own benefit, to enable the marketing of products at a competitive advantage”. Committee to Study HIV Transmission Through Blood and Blood Products, Institute of Medicine, Leveton et al HIV and the Blood Supply: An Analysis of Crisis Decisionmaking 1995 p109 JREE0000019
(1928) See for example his comments on commercial sensitivity. Dr Peter Foster Transcript 25 March 2022 pp57-59, p131 INQY1000198
(1929) Berntorp et al A systematic overview of the first pasteurised VWF/FVIII medicinal product, Haemate P/Humate-P: History and clinical performance European Journal of Haematology 2008 p8 JREE0000008. The product later became known as Haemate P.
(1930) Memo from Robert Taub to H Terreer and others 2 February 1979 CGRA0000218, Memo from Lee Kriley to G Phelps 22 May 1979 CGRA0000219
(1931) Memo from Lee Kriley to G Phelps 22 May 1979 CGRA0000219
(1932) The HT standing for heat-treated.
(1933) Memo from Lee Kriley to Distribution 14 June 1979 p3 CGRA0000220, which notes “Behringwerke and Immuno are reportedly working actively on the development of a Factor VIII replacement product that is ‘safe’ from the risk of Hepatitis. We have information to the effect that Behringwerke is approaching the completion of the clinical evaluation of its product … The significant demonstrable product differentiation that will be accomplished by the development and implementation of a Hepatitis Infectivity-Free Hemofil will result in dramatic increases in unit sales and in average selling price … projected effect on gross profit, $87,370,000 from 1981 through 1983”.
(1934) Cutter initially opted for a wet heat process but found it was difficult reliably to scale it up for production in sufficient quantities, so changed focus to its work on dry heating.
(1935) Ernst Weidmann Transcript in Anon and Others v Alpha Therapeutic Co and Others 4 November 1993p1273 MULL0000269
(1936) Letter from Dr Sternberg to Dr Schaeffler and others 24 May 1983 p1 CGRA0000412, Mozen The Development and use of the Coagulation Concentrates Factor IX [Konyne] and Factor VIII (Koate TM) Treatment of Bleeding Disorders 1980p8 BAYP0000021_031
(1937) Heimburger et al Factor VIII Concentrate – now free from hepatitis risk: progress in the treatment of haemophilia Die Gelben Hefte 1980 PRSE0004058
(1938) Director of the Scottish National Blood Transfusion Service. He also wrote to John Watt of PFC, plainly moved by the surprise and the importance of what had been described. Letter from Dr Cash to Dr Watt 27 October 1980 PRSE0003704
(1939) Written Statement of Dr Peter Foster paras 33.1i and 43.1 WITN6914001. His view had been shared by many fractionators. Dr Smith put it graphically when he said that “The truth is that heat treatment was one of the least likely candidates, from the universal experience of all who worked with coagulation factors … If the product experienced slight over-heating … we would be left with insoluble brown toffee”. Written Statement of Dr James Smith para 49 WITN3433001
(1940) Heimburger et al Factor VIII Concentrate – now free from hepatitis risk: progress in the treatment of haemophilia Die Gelben Hefte 1980 p1 PRSE0004058
(1941) Memo from David Castaldi to Distribution 3 June 1981 p1 MULL0001939_058. “The rationale for proceeding with the present heat treatment process is based on the following factors:
The present product seeded with hepatitis might successfully avoid transmission of hepatitis in a chimp study.
In any event, there is a very high probability that product subjected to the present heat process is substantially improved in terms of its hepatitis virus transmission characteristics and that we should move forward toward making the product available to patients.
The business need in Germany is great.”
(1942) Leveton et al HIV and the Blood Supply: An Analysis of Crisis Decisionmaking 1995 p106 JREE0000019. For the UK licence dates, see the chapter on Regulation of Commercial Factor Concentrates. Immuno of Vienna concentrated on a virucidal process (a form of chemical treatment) to try to inactivate hepatitis viruses. This was announced to many of the UKHCDO directors and Dr John Craske on 24 January 1983 in a day long meeting at the Excelsior Hotel, Heathrow, and early results were said to have been successful. It does not feature further in this account. Notes of Immuno meeting 24 January 1983 PRSE0002647
(1943) Food and Drug Administration (“FDA”)
(1944) Ernst Weidmann Transcript in Anon and Others v Alpha Therapeutic Co and Others 4 November 1993 p264 MULL0000269
(1945) Ernst Weidmann Transcript in Anon and Others v Alpha Therapeutic Co and Others 4 November 1993 pp276-277 MULL0000269
(1946) Ernst Weidmann Transcript in Anon and Others v Alpha Therapeutic Co and Others 4 November 1993 p290 MULL0000269
(1947) In early 1984 the Alpha product was the one which Dr (later Professor) Eric Preston in Sheffield, Professor Geoffrey Savidge at St Thomas’ in London, Dr (later Professor) Samuel Machin at the Middlesex and Dr Mark Winter in Kent decided to give to their patients on a named patient basis, because they thought it would have a better chance of being free of the risk of AIDS. Written Statement of Dr Winter paras 35.5-35.9 WITN3437002
(1948) Ernst Weidmann Transcript in Anon and Others v Alpha Therapeutic Co and Others 4 November 1993 pp270-271 MULL0000269. The process was indeed different. It removed fibrinogen with a polyethylene glycol solution, and did not dissolve the freeze-dried product. Their factor proteins were suspended in liquid which was then heated. The process did not use stabilisers. Ernst Weidmann Transcript in Anon and Others v Alpha Therapeutic Co and Others 4 November 1993 p292 MULL0000269
(1949) 2 September 1981. SNBTS Briefing Paper on the Development of Heat Treatment and Coagulation Factors November 2010 p32 PRSE0002291
(1950) Written Statement of Dr Peter Foster para 43.2 WITN6914001
(1951) Preliminary Studies on the Heat Treatment of PFC FVIII Concentrate 10 February 1982 PRSE0001549
(1952) Draft Proof of Evidence of Dr James Smith for HIV Haemophilia Litigation 1 November 1990 p20 CBLA0000016_034. Dr Smith was chief chemist at PFC in Edinburgh (1968-1975) and then scientist in charge of fractionation at PFL in Oxford (1975-1992) and also head of coagulation factor production at BPL in Elstree (1979-1982).
(1953) Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 p394 CBLA0000005_002
(1954) Proposal for research project on the development of methods for the production of coagulation factor concentrates with reduced hepatitis transmission 27 February 1981 p1 CBLA0001291
(1955) Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 p389 CBLA0000005_002
(1956) Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 p389 CBLA0000005_002, Minutes of Scientific and Technical Committee for the CBLA meeting 4 March 1981 p3 CBLA0001299
(1957) Note of Dr Michael Harvey and Dr Smith discussion 14 September 1981 pp6-7 CBLA0001446. A number of other possibilities for reducing the risk of hepatitis were canvassed by BPL in the second half of 1981. They were: more specific sensitive screening of blood donations intended for fractionation; limiting the size of plasma pools; neutralisation or absorption of virus with an excess of hepatitis antibody; vaccination of recipients (for Hepatitis B); selective removal of viruses during fractionation (eg by precipitation with PEG (polyethylene glycol)); inactivation of virus eg with B-propiolactone or by heating in the presence of reagents preserving the biological activities of plasma proteins. Minutes of Scientific and Technical Committee for the Central Blood Laboratories 24 November 1981 p5 CBLA0001506
(1958) See generally Dr Lane’s account: Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 pp389-394 CBLA0000005_002
(1959) Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 p391 CBLA0000005_002. He complains in his draft proof of evidence for the HIV haemophilia litigation that “DOH [Department of Health] policy was that Regional Health Authorities were to all intents and purposes responsible for allocation of budgets, and the DOH would not intervene in the exercise of their discretion. However, at the same time, BPL and PFL were funded directly by the DOH which closely controlled all but very minor expenditure.” This part of his proof speaks of the position in 1973. Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 p27 CBLA0000005_002
In 1978 it changed, following the withdrawal of Lister from the Elstree operation: it now became a Joint Management Committee (“JMC)”, a joint committee of the DHSS and North West Thames regional health authority, that according to Dr Lane handled “financial affairs”. The Scientific and Technical Committee and a Finance Sub-Committee were set up in 1979. Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 p5, p77 CBLA0000005_002
Capital funding was still, however, the preserve of central government, which in 1980 considered that so far as the laboratory at BPL was concerned “expenditure on up-grading should be reviewed and minimised pending a decision on the laboratory’s future.” Minutes of Scientific and Technical Committee for the CBLA meeting 23 April 1980 p3 CBLA0001093 quoted at Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 p104 CBLA0000005_002. Dr Lane’s account of 1981 is one of his battle to secure a commitment from the government to redevelop BPL, and to fund the improvements necessary following an adverse Medicines’ Inspectorate report. Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 pp120-140 CBLA0000005_002. In summary, he seems to blame the DHSS (or the JMC) for not giving him funds which he could apply at his discretion to support research.
(1960) Minutes of Scientific and Technical Committee for the CBLA meeting 4 March 1981 p3 CBLA0001299
(1961) Notes on experiments relating to Factor IX Solution Heating and Factor IX Project 9H p2 CBLA0002456
(1962) Transfusion is a journal intended for fractionators, amongst others.
(1963) “It is reasonable to be optimistic concerning stabilization to heat of most high-risk plasma derivatives in the near future. Theoretically, heating of stabilized high-risk plasma derivatives could inactive HBV as well as the agent of non-A, non-B hepatitis, which has also been shown to be inactivated by heating at 60°C for 10 hours.”Gerety and Aronson Plasma derivatives and viral hepatitis Transfusion 1982 p4 BPLL0011656. Drs Gerety and Aronson were well placed to make this observation: they worked in the Hepatitis and Coagulation Branches of the Division of Blood and Blood Products of the Office of Biologics of the FDA.
(1964) Memo from Dr Walford to Dr Leslie Fowler 22 December 1982 p1 DHSC0003722_029
(1965) Written Statement of Dr James Smith para 56 WITN3433001
(1966) Proposal to Develop a “Hepatitis Safe” Factor VIII Concentrate CBLA0001781. The date of this is given by Dr Lane as February 1983: Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 p411 CBLA0000005_002. The proposal notes in a comment which supports the conclusions of this report expressed elsewhere in respect of the appreciation of risk, that “NANBH causes increasing concern, less on account of its acute effects (although deaths have been reported) than because of its association with chronic active hepatitis in later life”, and that AIDS was “not yet proven to be of viral origin, but this is strongly presumed”. Note the date. Proposal to Develop a “Hepatitis Safe” Factor VIII Concentrate p1 CBLA0001781
(1967) Leveton et al HIV and the Blood Supply: An Analysis of Crisis Decisionmaking 1995 p106 JREE0000019 (Factorate HT).
(1968) Leveton et al HIV and the Blood Supply: An Analysis of Crisis Decisionmaking 1995 p106 JREE0000019 (Ultimately, this product was not brought to market even though licensed.)
(1969) Leveton et al HIV and the Blood Supply: An Analysis of Crisis Decisionmaking 1995 p106 JREE0000019 (Profilate HT).
(1970) Leveton et al HIV and the Blood Supply: An Analysis of Crisis Decisionmaking 1995 p106 JREE0000019 (Koate HT).
(1971) Memo from Dr Smith to Dr Lane and others 3 January 1984 p13 CBLA0001786
(1972) Memo from Dr Smith to Dr Lane and others 3 January 1984 p1 CBLA0001786. Dr Lane in his draft proof of evidence for the HIV Haemophilia Litigation, produced 10 December 1990, wrote “The reference above to our ‘late start’ is not to be misunderstood. The documentation I have discussed above indicates our intention to define a heat treatment process capable of full virus inactivation, probably requiring more severe heating than was currently recognised.”Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990p423 CBLA0000005_002. If this is intended to say that the words “late start” (which are not in inverted commas in Dr Smith’s proposal) does not mean that the UK lagged behind other countries in developing a form of viral inactivation, I cannot accept it. First, the words are Dr Smith’s – they are not Dr Lane’s. They should therefore be taken at face value unless there were evidence from Dr Smith that they had some other force.
Second, to compare products which had finished trials so as to have gained US licences, or be on the point of doing so, with what he said in the UK was “our intention”, is to compare an achievement (by US producers) with an idea (on the part of BPL in England). The idea is plainly well behind the achievement. Thus BPL made a late start in this sense. Third, in context it bears the meaning that the text sets out: the pharmaceutical companies were ahead of BPL to such an extent that there was a risk that patients in the UK not previously treated, or only lightly treated, would be recruited into trials for commercial products. Numbers of such patients were limited: and if recruited by commercial companies for that purpose they could no longer be approached by BPL to ask if they would participate in testing BPL’s heat-treated product. A consequence would be that when the idea of heat treatment was translated into the achievement of an actual product by BPL, it would lack any means of showing regulatory authorities, patients and clinicians that its product was reasonably safe for use.
If the “misunderstanding” to which Dr Lane refers relates to some other matter, he does not spell it out. The view expressed here is further supported by what Dr Smith had said in February 1983: that it was necessary “to avoid a duplication of effort with other trustworthy laboratories”going on to say “Since we start from some way behind, a modest stance will be quite appropriate. We should envisage the possibility of having to use, and pay for, proprietary information e.g. through a licence arrangement … The Production Department should, therefore, perhaps budget for possible royalty payments … while hoping that in-house work will save these costs.”Emphasis added. Proposal to develop a hepatitis safe Factor VIII Concentrate p10 CBLA0001781. Dr Lane’s words thus had the appearance of seeking to explain away something which it would be embarrassing to admit. It has however to be remembered that they appear in a draft proof of evidence, which may not have come to its final form with these words in it; but the truth appears to be that BPL had allowed itself to fall further behind the rest of the pharmaceutical world.
(1973) Memo from Dr Smith to Dr Lane and others 3 January 1984 p1, p5 CBLA0001786
(1974) Colvin et al Heat-treated NHS Factor VIII concentrate in the United Kingdom - a preliminary study Clinical & Laboratory Haematology 1986 p3 PRSE0000608
(1975) Minutes of Central Committee for Research and Development in Blood Transfusion meeting 28 February 1984 p3 PRSE0001972
(1976) Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 p435 CBLA0000005_002. It began “activities leading to the establishment of the 8Y process” in earnest in May 1984, according to Dr Terence Snape. Draft Written Statement of Dr Snape for the Tribunal of Inquiry into Infection with HIV and Hepatitis C of Persons with Haemophilia and Related Matters p12 NHBT0004065_003
(1977) Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 pp429-431 CBLA0000005_002
(1978) By contrast, a solvent/detergent method of inactivation would be effective only against virus particles which had a lipid (fatty) coat. It was unknown at this stage whether either non-A non-B Hepatitis or the viral cause of AIDS – assuming that it had a viral cause – would have such a coating. There might also be other as yet unknown viruses or pathogens in blood which would be susceptible to heat.
(1979) At Sheffield, St Thomas’, the Middlesex and Margate. Written Statement of Dr Mark Winter paras 35.6, 35.9 WITN3437002. There was a fear that the heat would create “neo-antigens”. There was also concern that using stabilisers to protect Factor 8 or 9 proteins from degradation might also stabilise the viral particles which the heat was intended to destroy.
(1980) Emphasis added. Levy et al Recovery and Inactivation of Infectious Retroviruses added to Factor VIII concentrates The Lancet 29 September 1984 p1 CBLA0001898
(1981) Morbidity and Mortality Weekly Report Acquired Immunodeficiency Syndrome in Persons with Hemophilia 26 October 1984 p3 BART0002308
(1982) 2 November 1984. Written Statement of Dr Peter Foster para 43.5xi WITN6914001
(1983) One example is from Canada, where on 16 November 1984 the Bureau of Biologics issued a statement that further reliance on AHF products which had not been heat treated could not be justified. It called for replacement of unheated product by heat-treated product “because heat treatment of antihemophilic factor, human, dried (AHF) products has been shown to inactivate some viral agents that may cause serious disease, further reliance on AHF products that have not been heat-treated cannot be justified. The Bureau of Biologics therefore recommends that use of untreated AHF be replaced as soon as possible with AHF products that have been heat-treated.” Telex from Dr David Pope to Dr Robert Perrault 16 November 1984 CBLA0000056_063
(1984) Letter from Dr Lane to Dr Harris 12 October 1984 CBLA0001907
(1985) Letter from Dr Harris to Dr Lane 8 November 1984 CBLA0001916. The universal introduction of a screening test did not occur until 14 October 1985, almost a year later. It might have been anticipated at this stage, reasonably, that it would come much sooner than that (and indeed the Inquiry has found that it should have done: see the chapter on HIV Screening), but on analysis Dr Harris’ position depended upon such a test having 100% sensitivity. To the extent it did not, some HIV/HTLV-3 virus could still enter the plasma pools from which concentrate was made at BPL. Pooling would spread the risk that virus posed to anyone receiving concentrate from the pool. Yet Dr Harris knew, or should have known, that the recent history of Hepatitis B screening was that initial tests detected only about one third of viral samples, and even the next generation still left one third undetected. It would have been a leap of optimistic faith, rather than the application of experience, to have relied upon it. Dr Harris did refer the matter for an expert advisory group to consider – whether universal screening was the answer to whether blood products would be infective, or whether viral inactivation treatment of the finished product was the solution, with a third option being to use both. Each had its own cost implication. By way of comment, whichever solution was preferred ought in this context to have placed the safety of the patient as an overriding consideration. However, it was nearly three weeks before the working group discussed this issue. As will be seen in the text which follows it took the view that the third option – “belt and braces” – was appropriate. For the reasons given above, this was plainly right.
(1986) Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 p432 CBLA0000005_002
(1987) It is clear that it did not stall or deter Dr Lane from seeking to push forward, however – see the next paragraph.
(1988) Minutes of Central Committee for Research and Development in Blood Transfusion meeting 9 November 1984 pp2-3 CBLA0001919
(1989) Memo from Mr David Wesley to Dr Lane and others 19 November 1984 p2 CBLA0001923
(1990) Dr Alison Smithies updated the Secretary of State on the same day and the CMO the following day. Note from Dr Smithies to Dr George Godber 19 November 1984 p3 DHSC0002309_053, Memo from Dr Smithies to Dr Richard Alderslade 20 November 1984 DHSC0002249_034
(1991) The Times Treated blood cuts Aids risk to haemophiliacs 20 November 1984 HSOC0016001. Both The Times and the Daily Express reported that the CBLA announcement that blood products would be heat treated to reduce the risk of AIDS followed Terence McStay’s death, which had been reported on Sunday 18 November. Daily Express Twin bid to curb killer AIDS peril 20 November 1984 HSOC0015994. The articles followed the Daily Mail’s front page of Monday 19 November which read “AIDS Virus kills man in Britain” HSOC0015992
(1992) Letter from Professor Bloom to Dr Smithies 21 November 1984 DHSC0001211. His tone at this point is one of slightly grudging acceptance of the need to do so: “It looks very much that we are going to be driven into using heat treated concentrates.”
(1993) From 18 November 1984. PFC repurposed the spray cabinet used to pasteurise albumin pending the purchase of specialist ovens and had conducted a test of the concept on 14 November 1984. Written Statement of Peter Foster for the Penrose Inquiry 29 June 2011 p28 PRSE0003349. It is not known whether this might have also been done at BPL.
(1994) Presumably from the viewpoint of the DHSS. Memo from Dr Michael Abrams to Dr Harris 27 November 1984 p1 DHSC0002251_011. The alternative view is examined in the chapter on HIV Screening.
(1995) Memo from Dr Abrams to Dr Harris 27 November 1984 p2 DHSC0002251_011. In relation to the latter suggestion, see the chapter on Regulation of Commercial Factor Concentrates.
(1996) In answer to his letter of 21 November: Letter from Professor Bloom to Dr Smithies 21 November 1984 DHSC0001211, Letter from Dr R D Mann to Professor Bloom 29 November 1984 DHSC0002251_021
(1997) PFC had produced 11 pilot batches of “ZHT” (a pasteurised heat-treated product) between February 1983 and September 1984, and tested the clinical validity of this product in late 1983. Although Dr Foster thought the more promising route in the longer term was pasteurisation, by late 1984 the data presented at Groningen showed that heat treatment could inactivate HTLV-3, and the desirability of a prompt response to meet the threat of AIDS led to Dr Cash, who headed up SNBTS, accepting a recommendation that the service should dry heat its Factor 8 products as soon as possible. Pasteurisation would have to wait. PFC realised that its existing product would tolerate heat at 68°C for two hours, and started to heat it in mid November 1984. Written Statement of Dr Peter Foster para 69, para 86 WITN6914001
(1998) SNBTS Briefing Paper on the Development of Heat Treatment and Coagulation Factors November 2010 p33 PRSE0002291
(1999) Dr Snape (Head of Quality Control at BPL) would write to haemophilia centre directors on 24 January 1985 to inform them that “limited supplies” of a heated Factor 8 concentrate would be available in early February and that would be “the product generally available for the next three to four months, the amounts being 50-60% of what would otherwise have been supplied as unheated concentrate.” Then “an improved higher purity concentrate, designed specifically with anti-viral treatment in mind [8Y] … initially in limited quantity” would be introduced from April onwards. Letter from Dr Snape to Haemophilia Centres 24 January 1985 p1 CBLA0001998. Dr Smith explained in his written statement that 8Y was available on clinical trial from April 1985 for those with no prior exposure to concentrates, or minimal exposure to cryoprecipitate. From August or September 1985, all patients became eligible, subject to availability, and the intermediate product was not issued after September 1985. Heat-treated Factor 9 became routinely available in October 1985. Written Statement of Dr James Smith para 56 WITN3433001. PFC routinely issued heat-treated Factor 9 from August 1985. SNBTS Briefing Paper on the Development of Heat Treatment and Coagulation Factors November 2010 p34 PRSE0002291
(2000) Memo from Dr Smith to Dr Lane and others 20 November 1984 p2 CBLA0001926
(2001) Minutes of Haemophilia Reference Centre Directors meeting 10 December 1984 pp8-9 HCDO0000394_117. On the equipment ordered, he explained: “three ovens are required, one is already in use, and two are expected in March.”
(2002) Minutes of Haemophilia Reference Centre Directors meeting 10 December 1984 p4 HCDO0000394_117
(2003) Blood transfusion, haemophilia and AIDS The Lancet 22/29 December 1984 p2 CBLA0001964
(2004) Batches manufactured as early as October 1983 were heat treated.
(2005) Written Statement of Dr Peter Foster paras 43.5xviii and 43.6iii WITN6914001
(2006) Letter from Dr Perry to Transfusion Directors 6 December 1984 PRSE0002675
(2007) Cutter UK Year End Review and Reports January 1985 p5 CGRA0000554
(2008) The 10 December meeting of UKHCDO reference centre directors clearly implies these were readily available even though not yet licensed. Minutes of Haemophilia Reference Centre Directors meeting 10 December 1984 p7 HCDO0000394_117. Dr Smith had said the same in his memo of 20 November 1984 to Dr Lane: “US companies say they can provide UK with more than enough heated product, today.” Memo from Dr Smith to Dr Lane and others 20 November 1984 p2 CBLA0001926
(2009) Haemate P, produced by Behringwerke, was also licensed but was not actively marketed in the UK and so was effectively unavailable. Counsel Presentation on the Overview Chronology of the Licensing of Commercial Blood Products in the United Kingdom during the 1970s and 1980s 6 December 2022 pp29-30 INQY0000411. See the chapter on Regulation of Commercial Factor Concentrates for more detail.
(2010) The description Dr Smith had given it, but which Dr Lane did not appear readily to accept: see footnote 1972.
(2011) Minutes of Executive Committee of the Haemophilia Society meeting 10 January 1985 p2 HSOC0029476_044
(2012) Letter from Dr Snape to Dr Mary Duncan 28 February 1985 p2 CBLA0002074
(2013) By this, he plainly meant consumption within England and Wales, and it is a very broad approximation. It is also retrospective: for a consequence of heat treating the product available from BPL (before 8Y was produced in sufficient quantity) was that the yield of clotting factor available from a given quantity of plasma was reduced and hence Dr Snape’s reference to supplies of heat-treated NHS concentrate being 50-60% of what would otherwise have been supplied as unheated concentrate. Letter from Dr Snape to Haemophilia Centres 24 January 1985 p1 CBLA0001998. Since commercial products filled the vacuum left by the 40-50% shortfall, NHS production for a while covered only some 25-30% of domestic consumption. The inference is that the briefing for Kenneth Clarke did not take account of this.
(2014) Written answers to Parliamentary Questions on Blood Products 5 February 1985 CBLA0002020
(2015) Haemophilia Society Haemofact Release No622 April 1985 p2 HSOC0008753
(2016) Fax from Dr Snape to Dr Perry 26 August 1999 p4 PRSE0003122. HT1 (60°C for 72 hours) had initially been applied to some batches made by PFL but this was quickly modified to HT2 (70°C for 24 hours). Draft Expert Witness Statement of Dr Terence Snape for the Tribunal of Inquiry into Infection with HIV and Hepatitis C of Persons with Haemophilia and Related Matters p12 NHBT0004065_003
(2017) Minutes of Haemophilia Reference Centre Directors meeting 10 December 1984 pp9-10 HCDO0000394_117
(2018) Counsel Presentation on Pharmaceutical Companies: Response to Risk November 2021 pp73-75 INQY0000311
(2019) It has to be borne in mind that the replacement facilities for BPL were in mid-construction; by contrast, PFC had unused capacity.
(2020) Written Statement of Dr James Smith paras 105-106 WITN3433001, Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 p451 CBLA0000005_002, Written Statement of Dr Mark Winter para 35.6 WITN3437002. Other centres did, however, begin to use heat-treated concentrates as and when they could following the December 1984 UKHCDO meeting.
(2021) Demonstrated by the fact that a number of patients in Edinburgh (the “Edinburgh cohort”) who had received NHS concentrate had been infected with the HIV/HTLV-3 virus.
(2022) “Better the devil you know” may reflect this. Dr Brian Colvin told the Inquiry that “if it were to be the case that these commercial products which had been heat treated were not safe, from the HIV point of view, then all my HIV negative patients would become HIV positive, and I’d have an even bigger crisis on my hands.” Dr Brian Colvin Transcript 7 October 2020 pp209-210 INQY1000062
(2023) Minutes of Haemophilia Reference Centre Directors meeting 10 December 1984 pp4-5 HCDO0000394_117
(2024) Report on heat treated and untreated Koate HT and Koate 1985 p5 CGRA0000559
(2025) Letter from Chris Spry to Douglas Hague 14 December 1984 TYWE0000012
(2026) Memo of Newcastle Health Authority 12 December 1984 TYWE0000019, Letter from Dr Peter Jones to Dr Liam Donaldson 23 February 1988 BPLL0002848_001
(2027) “With recent developments in the UK it is possible that our current Koate inventory will not be saleable in that country due to the rapid conversion of several centers to heat-treated factor VIII preparations. Every effort is to be made to sell the regular product in the United Kingdom. Only after total conversion of heat-treated factor VIII preparations has been made in the United Kingdom will we consider selling this product at a reduced price in Eastern European markets.” Emphasis added. Memo from Jack Wood to Willi Ewald 10 December 1984 p3 CGRA0000557
(2028) Memo from Brian Dyos and Linda Frith to M Costi May 1985 p3 BAYP0000024_201. The product in question was Koate Ultra-Filtered, which was an unheated product. The reference to short-dated stock might be a reference to a sale to Dr Edward Tuddenham, where the expiry date of the product offered was June 1985. In March 1985 Cutter’s representative had discussed selling some unheated product with Dr Tuddenham at a knock-down price (not for use at the Royal Free Hospital but for a charity providing haemophilia care in Pakistan). Letter from Brian Dyos to Dr Tuddenham 14 March 1985 CGRA0000560
(2029) The report is expressly a reference to the UK position, from Cutter UK. It is possible, though, that although its text deals with the UK the sales might have been from the UK to overseas interests, as in the case of the batch offered to Dr Tuddenham. This would reconcile the apparent meaning of this report with the content of a letter of 13 March 1985 from Cutter International to Dr Savidge in which they told him that because of the “drastic changes” that had taken place in the UK regarding heat-treated products since the previous September: “we at Cutter feel it is prudent to no longer effect sales of non-heat-treated product for use in the United Kingdom.” Letter from Jack Wood to Dr Savidge 13 March 1985 BAYP0000024_113
(2030) Report on heat treated and untreated Koate HT and Koate 1985 CGRA0000559, Memo from Brian Dyos and Linda Frith to M Costi March 1985 BAYP0000024_090, Letter from Jack Wood to Dr Savidge 13 March 1985 BAYP0000024_113. Also from 13 March 1985: “The inventory of non-heat-treated Koate in the United Kingdom is in excess of 4 million units. These have been identified to Gary Mull, asking that every effort be made by Cutter USA to reallocate this stock to markets not yet converted to heat-treated factor VIII preparations ... Inventory that cannot be re-allocated by Cutter US, we are recommending be granted a one year extension from NIBS, allowing us to re-label and sell over the coming year into markets not yet converted to heat-treated factor VIII products.” Memo from Jack Wood to Willi Ewald 13 March 1985 p4 BAYP0000024_114
(2031) Letter from Professor Bloom to Dr Charles Rizza 9 May 1985 DHSC0002269_069. 69% of centre directors responded and the results would be published in the British Medical Journal. Bloom et al Correspondence discussing HTLV-III Haemophilia and Blood Transfusion British Medical Journal 22 June 1985 PRSE0001917
(2032) The inference is that this was for financial reasons.
(2033) Minutes of AIDS group of Haemophilia Centre Directors meeting 20 May 1985 p9 HCDO0000273_015. He also observed that “he felt that the UK was not facing up to the potentially large problem of AIDS. ARC [AIDS related complex] was much more multifaceted than previously thought. Sero+ individuals seemed to have a 5% chance of developing AIDS and 25% chance of developing ARC. Cerebral infection with the HTLVIII virus was a very important and worrying feature which might result in neurological and mental deterioration in the long term.” p5HCDO0000273_015
(2034) Minutes of AIDS Group of Haemophilia Centre Directors meeting 17 June 1985 p4 HCDO0000523. The advice carries the implication that some were still using unheated concentrates. As to the importance of using heat-treated products, quite why the advice now to be given by UKHCDO directors had not been determined at its previous meeting, when Dr Mortimer had called for it, is unclear. A second point is that the status of the advice could only be that of a recommendation, however persuasive: a mandatory requirement would need the intervention of the regulator. For comparison, Sweden – the country in which the first commercial concentrate had been produced for sale in the 1960s – withdrew all Swedish Factor 8 concentrate which had not been heat treated in February 1985. Haemophilia Litigation Report June 1990 p120 DHSC0001297. In the UK, PFC had formally recalled all non-heat-treated Factor 8 by the start of 1985. BPL never issued a formal recall for unheated Factor 8. It was not until 2 May 1985 that all supplies of its Factor 8 products were heat-treated and until October 1985 that all supplies of BPL and PFC Factor 9 were heat-treated. Fax from Dr Snape to Dr Perry 26 August 1999 p4 PRSE0003122. Whether a formal recall should have been issued is discussed in the text which follows.
(2035) This was not heat treated (in the UK).
(2036) This addressed the “better the devil you know” approach. Bloom et al Correspondence discussing HTLV-III Haemophilia and Blood Transfusion British Medical Journal 22 June 1985 PRSE0001917
(2037) An example is that an inventory for Alpha UK showed that just under 25% of its current stocks remained non-heat-treated at the start of September 1985. Fax from Kath Hatton to C Lawrence 2 September 1985 CGRA0000565
(2038) In practical terms, the DHSS: see the chapter on Regulation of Commercial Factor Concentrates. Nor did the CMO issue any letter amounting to an instruction to treating clinicians not to use non-heat-treated product.
(2039) Written Statement of Dr Terence Snape para 189 WITN3431001
(2040) By then, BPL had reached maximum output in its then premises. Letter from Dr Harris to Dr Smithies 15 August 1985 p2 DHSC0002489_110. This is despite the fact that Dr Smithies, whose responsibility in the DHSS was blood and blood products was present at the meeting of 10 December 1984 of UKHCDO directors, BPL staff, Dr Mortimer, Dr Tedder and Dr Craske at which those present are minuted as agreeing that heat-treated product “must” be given to HIV negative patients, and should if available be given to all patients including those who were HIV positive. Minutes of Haemophilia Reference Centre Directors meeting 10 December 1984 p4 HCDO0000394_117. Dr Walford, who had occupied the same role immediately prior to Dr Smithies taking it over, described the Medicines Division as effectively being the regulatory authority. The Licensing Authority did not take action to ensure recall of unheated concentrates.
(2041) So far as Factor 9 was concerned, unheated BPL Factor 9 was used until October 1985. Written Statement of Dr Terence Snape para 193 WITN3431001
(2042) Cutter’s results were in the 26 October 1984 MMWR. Morbidity and Mortality Weekly Report Acquired Immunodeficiency Syndrome in Persons with Hemophilia 26 October 1984 BART0002308
(2043) Alpha put their results in their patient information leaflet dated January 1985. Memo from Christopher Bishop to Dr Charles Swartz 3 July 1985 p2 ARMO0000414
(2044) Blood transfusion, haemophilia and AIDS The Lancet 22/29 December 1984 p2 CBLA0001964
(2045) Morbidity and Mortality Weekly Report Acquired Immunodeficiency Syndrome in Persons with Hemophilia 26 October 1984 p3 BART0002308
(2046) Morbidity and Mortality Weekly Report Acquired Immunodeficiency Syndrome in Persons with Hemophilia 26 October 1984 p3 BART0002308
(2047) Telex from Dr David Pope to Dr Robert Perrault 16 November 1984 CBLA0000056_063
(2048) Minutes of Haemophilia Reference Centre Directors meeting 10 December 1984 p5 HCDO0000394_117
(2049) With input from Dr Mortimer and Dr Craske, from their public health perspectives, and Dr Tedder from his virological standpoint.
(2050) Written Statement of Dr Terence Snape para 196 WITN3431001
(2051) There are two differences between the position in respect of Factor 8 and that in respect of Factor 9. First, there was insufficient heat-treated Factor 8 product of domestic origin to supply the needs of all patients requiring treatment; so either existing stocks of unheat-treated product would need to be used or commercial heat-treated products would have to be (whereas there was no need to use commercial products when domestic heat-treated Factor 9 became available, since domestic supply was adequate). Second, and tending the other way, there were greater fears in the case of Factor 9 than in the case of Factor 8 that heat-treated product might give rise to a greater risk of causing thrombosis. The Inquiry has not lost sight of either point.
(2052) The logic is that recall, to avoid the use of more dangerous products, should have been made as soon as reasonably possible. This might have varied depending upon the particular circumstances of individual regions, yet a recall, reasonably, should take place across the board. It might, perhaps, have been reasonable to wait until products were licensed and thus freely available without a need for named patient exemptions, and the link to the financial year is suggested to accommodate what may have been difficulties in some regional health authorities in meeting additional expense at the tail end of a financial year when that expense had not been budgeted for and could affect resources for the care of other patients. There is no obvious reason why it would be reasonable for it to have been any later.
(2053) Minutes of UK Haemophilia Centre Directors Hepatitis Working Party meeting 6 February 1985 p3 HCDO0000562
(2054) Memo from Dr Snape to Dr Lane 7 February 1985 p2 CBLA0002031
(2055) Bloom et al Correspondence discussing HTLV-III Haemophilia and Blood Transfusion British Medical Journal 22 June 1985 p1 PRSE0001917. The choice for the patient was not just that between heated and unheated concentrates: there was the option of FFP or no treatment, which was the patient’s prerogative (and was not unrealistic given that it was expected that heat-treated NHS Factor 9 would become available in the near future so that it would any change would be temporary).
(2056) Written Statement of Dr Terence Snape paras 191-198 WITN3431001, SNBTS Briefing Paper on the Development of Heat Treatment and Coagulation Factors November 2010 pp51-52 PRSE0002291
(2057) Written Statement of Dr Terence Snape para 196 WITN3431001
(2058) The concern that heated Factor 9 concentrates might cause thromboses was a real one, and sufficient for the Inquiry not to find that there should have been a recall of unheated product, or that unheated product should no longer have been used. Using it, however, did come with some risk – as Dr Snape had pointed out – of which the patient needed to know. Memo from Dr Smith to Dr Lane and Dr Snape 11 April 1985 p3 CBLA0002489
(2059) Notice of discontinuance of supply and product recall: Factor IX type 9D 7 October 1985 CBLA0002261, SNBTS Briefing Paper on the Development of Heat Treatment and Coagulation Factors November 2010 p52 PRSE0002291. Contrast the position in respect of Factor 8.
(2060) SNBTS Briefing Paper on the Development of Heat Treatment and Coagulation Factors November 2010 p52 PRSE0002291
(2061) In this chapter, it is important to remember that the companies licensing, marketing and distributing Armour product in the UK (both named Armour Pharmaceutical Company Limited in succession) were not the same companies as the company (Armour Pharmaceutical Company) that produced the product in the US. The first Armour UK had several changes of name and parent company. It was renamed Revlon Healthcare Limited in 1982, and subsequently Rorer Healthcare Holdings Limited in 1986. Finally it was dissolved in 2010. The second Armour UK was incorporated in 1982 and given the same name Armour Pharmaceutical Company Limited, a name which it held until the mid-90s. Written Statement of Samantha Silver paras 7-8 WITN3422001. Where this chapter uses the name “Armour” it is referring to the companies (depending on the relevant time/documentation) named Armour Pharmaceutical Company Limited, and not to the US company, unless the context necessarily requires otherwise. It uses “Armour” (rather than its full title) for convenience in reading the account.
(2062) The batch was Y69402. On 10 May 1985 Christopher Bishop (in his capacity as Armour’s Manager of the Plasma Division, Northern Europe) wrote to the centres which had received batch Y69402, asking if they still held any of it. The batch had been issued for use on a named patient basis to the haemophilia centres in Nottingham, Newcastle, Margate, Southampton, Belfast, Swansea, Lewisham and Sheffield. Letter from Christopher Bishop to Dr Andrew Bell 10 May 1985 ARMO0000379. The situation was discussed with the DHSS in a meeting on 10 May 1985 and on 31 May Armour provided to the DHSS details of the centres which had received the batch. Letter from Clive Collins to A Woodhead 31 May 1985 ARMO0000172. On 13 May 1985 the DHSS sent a letter informing all blood transfusion directors about the particular batch and that it had been recalled Letter from A Woodhead to Blood Transfusion Service Directors 13 May 1985 ARMO0000171
(2063) Letter from Robert Christie to Dr David Whitmore 17 July 1985 ARMO0000418
(2064) Letter from Dr Ricardo Landaburu to Clive Collins 10 January 1985 p3 ARMO0000343. The original CDC experiments on heat treatment had been conducted with Cutter’s and Alpha’s products and then Hyland asked CDC to conduct similar tests on their product, with similar results. Armour did not submit their product for CDC testing at that time but was aware of the CDC results. Evatt The AIDS epidemic in haemophilia patients II: pursuing absolute viral safety of clotting factor concentrates 1985–1988 Haemophilia 2012 p2 RLIT0002146, Letter from Dr Bruce Evatt to Dr Fred Feldman of Armour 29 November 1984 MULL0004337
(2065) Letter from Dr Prince to Dr Landaburu 24 January 1985 p1, p6 ARMO0000356. Dr Prince reported that “Higher inactivation process efficacy could not be demonstrated in this experiment due to the unexpectedly low titer of the virus stock employed.”
(2066) Presentation by Counsel to the Inquiry Pharmaceutical Companies: Response to Risk Appendix: The Prince Controversy para 9 INQY0000312
(2067) Safety of Blood Derivatives Pasteurized in the Dry State p4 PRSE0004828
(2068) Memo from Dr William Terry to the Record 8 November 1985 CGRA0000512. He did eventually produce a publication which revealed this, but since he was contractually unable to rely on the experiments he had conducted under contract to Armour, he had to repeat them in his own time in his laboratory facilities and draw conclusions based on this fresh, repeat work. Prince Effect of Heat Treatment of Lyophilised Blood Derivatives on Infectivity of Human Immunodeficiency The Lancet 31 May 1986 PRSE0002534
(2069) Proceedings of AIDS Conference 1986 p118 RLIT0001202, Note on post transfusion AIDS 13 February 1986 ARMO0000469. An Armour memo the following month described Dr Jones as having “recently had his wrists slapped for public statements.” Memo from Dr Harris to A Sheppard 14 March 1986 ARMO0000514. In his written statement to the Inquiry, Dr Jones explained that this was by the CMO, Dr Donald Acheson. Written Statement of Dr Peter Jones para 68.3 WITN0841038. Dr Acheson was reported in The Guardian as having said that “It was an error of judgment [sic] for him [Dr Jones] to go public on scanty and slender evidence.” Factor 8 Aids threat 14 February 1986 ARMO0000472. The same report recorded a DHSS spokeswoman as saying that the Netherlands case could be discounted. At that date the DHSS had little information about the Netherlands case, and Armour itself had not at that stage discounted the case, thus there was no proper basis for a DHSS spokeswoman to make this statement, assuming that it was accurately reported by The Guardian. (There is some evidence of there having been a conversation between the DHSS and the Dutch Ministry of Health at some point before 17 February – see the memo from Dr Smithies to Dr Harris – which suggests that “initial information” had been provided: Memo from Dr Smithies to Dr Harris 17 February 1986 p1 DHSC0002295_044). Dr Jones wrote to colleagues on 17 February 1986 enclosing a copy of his conference paper and explaining his decision to present the information about possible seroconversions at the conference: “My view was that because of the paucity of sero-negative cases on a variety of heat-treated materials and the time lag involved, that we could not afford to wait until sufficient ‘scientific’ evidence was available.”Letter from Dr Jones to medical professionals 17 February 1986p1 DHSC0002169
(2070) On 3 October 1985 Clive Collins, the regulatory affairs manager for Armour in the UK, wrote to Dr Duncan at the DHSS “in respect of the long term follow-up of patients who received the above batch of material prior to its withdrawal from the UK market.” His letter explained that they had not received written replies from all centres but were monitoring the situation “to the best of our ability.” The letter made no reference to the Lewisham patient, although he had been copied into the letter about the Lewisham patient in July. Letter from Clive Collins to Dr Duncan 3 October 1985 ARMO0000178. His statement effectively says that he remembers nothing and “Given the specialised medical nature of the problem it was appropriate that my Medical Department colleagues dealt directly with the DHSS Medical staff.” Written Statement of Clive Collins para 33e WITN7021001. When this criticism was put to him under the Inquiry Rules 2006 he responded that he communicated regularly with the DHSS and that the fact that a single memo did not mention a particular patient cannot be read to mean that there was no communication between Armour and the DHSS about the patient. Some information may have filtered through to the DHSS because Dr Smithies wrote to the CMO to inform him that there “is some hearsay evidence that haemophiliac patients are seroconverting to become anti HTLV III positive despite being given heat treated Factor VIII.”However Dr Smithies’ communication did not suggest any specific knowledge regarding the Armour product or the Lewisham patient. Letter from Dr Smithies to Kathy Doran 28 November 1985 DHSC0002295_047. It was only after Dr Jones’ intervention that Armour decided to report the Lewisham case to the DHSS. Robert Christie of Armour, in an internal memo to Dr Harris of Armour, described Dr Rotblat (DHSS) as “a valuable ally at the moment” and recorded that “I am now obliged to report Dr Whitmore’s patient who sero-converted following treatment with Factorate HT Y69402 (AIDS donor in pool) to her as Dr Whitmore has confirmed that the patient remains HTLV-III positive.” Memo from Robert Christie to Dr Harris 18 February 1986 p2 CGRA0000520, Letter from Dr Isaacs to Dr Harris 18 February 1986 p3 DHSC0002295_011
(2071) Which he followed up with a letter to the Committee on Safety of Medicines (“CSM”) on 18 February 1986 setting out his “personal opinion that, unless there is irrefutable evidence to the contrary, the Armour material should be withheld until its safety can be endorsed by the C.S.M.”Letter from Dr Jones to the Medical Assessor 18 February 1986 WITN5281047
(2072) The DHSS also requested information about the Dutch case. A file note from Dr Harris of Armour recorded that this patient had received Factorate from a batch known to have contained donations from a person who had been confirmed to have AIDS. In Germany, half the batch had been heat treated, the other half had not, and confirmation was to be sought that the batch used to treat the patient was from the heat-treated half. Note on post transfusion AIDS 13 February 1986 ARMO0000469. On 17 February Robert Christie provided information about the Dutch patient in a telephone discussion with Dr Rotblat. Memo from Robert Christie to Dr Harris 18 February 1986 CGRA0000520
(2073) Memo from Dr Harris 17 February 1986 p2 ARMO0000475
(2074) Memo from Robert Christie to Plasma Team 17 February 1986 p1 ARMO0000474. Robert Christie’s role was as Director of Clinical Services.
(2075) Christopher Bishop Transcript 4 November 2021 p127 INQY1000158. From 1981 to 1987 he was manager of the biologicals division at Armour UK, giving him oversight of a number of countries including the UK but also Ireland, France, Scandinavia, Belgium, Luxembourg and the Netherlands, and he became the managing director of Armour UK from 1987 to 1993.
(2076) This is despite the confirmation given by Dr Harris as mentioned in the text: there is, of course, a difference between holding stocks and making a routine supply which may be a reconciliation.
(2077) Minutes of Plasma Executive Committee meeting 20 February 1986 p2, p4 CGRA0000514
(2078) Minutes of Factorate meeting 27 February 1986 ARMO0000496. Christopher Bishop set out his understanding of the policy in a status report in early March 1986: “Unscreened product could be supplied if, e.g. potency requirements and the clinician deemed it necessary.” Memo from Robert Christie to Plasma Team 17 February 1986 p3 ARMO0000474
(2079) Letter from Dr Jones to Dr Harris 25 February 1986 ARMO0000489
(2080) Robert Christie said in his statement to the Inquiry that “Dr Whitmore had asked for confidentiality because he had some concerns about the patient’s lifestyle and did not want the report to be publicised until he had investigated the issue.” Written Statement of Robert Christie para 68d WITN7500001. The Inquiry has found no evidence to support this assertion. Although it is noted that on 17 July 1985 Robert Christie wrote to Dr Whitmore saying “Some additional information would be helpful in assessing the situation and perhaps a meeting to discuss these patients would also be valuable”, the record of Robert Christie’s visit to Dr Whitmore on 27 February 1986 “to follow up the history of two haemophiliacs who had sero-converted to HTLV-III positive following treatment with Heat Treated Factorate”records that “This patient is in no other risk group for AIDS”. Letter from Robert Christie to Dr Whitmore 17 July 1985 ARMO0000418, Memo from Robert Christie to Dr Harris 28 February 1986 p1 CGRA0000515
(2081) Emphasis added. Memo from Robert Christie to Dr Harris 5 March 1986 p2, p4 ARMO0000501. Present from the DHSS were Dr Rotblat, Dr Betts and Dr Isaacs. On the face of it, this appears like a dereliction of duty on the part of the DHSS. However this might be because the DHSS was itself in an uncomfortable position, since at this stage not all of the product made in the UK, or distributed by BPL or PFC, had been made from the plasma of donors who had been tested and had not shown positive for the presence of HIV. Despite this possible embarrassment, the fact is that the Armour product was suspected of causing seroconversions whereas the domestic products were not: the issue was the effectiveness of the heat treatment regime rather than the prevalence of infection in the donor base.
(2082) The safety of heat treated Factor VIII 4 March 1986 p5 DHSC0001172
(2083) The safety of heat treated Factor VIII 4 March 1986 p5 DHSC0001172
(2084) Minutes of CSM(B) meeting 5 March 1986 p3 DHSC0001801. There is no evidence to suggest that the patients themselves were made aware that their information was being shared with Armour and others, or to suggest that they were aware that “close surveillance” was to be maintained on them.
(2085) Dr Rotblat spoke to her paper at the EAGA meeting. The cases she discussed were the Dutch patient, the Lewisham patient (although Lewisham was not identified as the centre) and a US patient who was said to have seroconverted after being treated with Hyland products.
(2086) Minutes of EAGA meeting 11 March 1986 pp5-6 DHSC0001499. The statement was said to be subject to clearance in the light of discussions by the CSM.
(2087) Memo from Robert Christie to Dr Harris 28 February 1986 p1 CGRA0000515
(2088) Letter from Dr Harris to Dr Brian Colvin 13 March 1986 pp1-2 BART0000894, Draft letter from Dr Harris 13 March 1986 pp1-2 ARMO0000512
(2089) White et al HTLV-III Seroconversion associated with heat-treated Factor VIII concentrate The Lancet 15 March 1986 BAYP0000008_118. The report in The Lancet did not identify which concentrate was implicated but Dr Rotblat’s report of 4 March 1986 identified it as Hyland.
(2090) Letter from Dr Jones to the Medical Assessor 17 March 1986 PJON0000121_001
(2091) Minutes of CSM meeting 26 March 1986 p4 MHRA0036364_002
(2092) Although Dr Rotblat was aware of the letter and her paper was intended as a response to it. Memo from Dr Isaacs to Dr Rotblat 26 February 1986 p1 DHSC0041345_004 . Dr Isaacs wrote to Dr Jones on 16 April 1986 explaining that “This matter has been reviewed by the Committee on Safety of Medicines. After consideration of all the latest available data, the committee advised that there was insufficient evidence for action to be taken on any specific product. Please be assured that the CSM is keeping this matter under continued review and will consider any new evidence as it becomes available.” Letter from Dr Isaacs to Dr Jones 16 April 1986 DHSC0000769
(2093) Along similar lines, on 12 June 1986 Dr Smithies informed the CMO that she had been told by Dr Dale Lawrence of CDC that he was seeking a sample of blood from the Lewisham patient. Memo from Dr Smithies to William Leason 12 June 1986 DHSC0002303_015. The CMO responded by asking “Is there not a case to do something about Armour’s licence?” Memo from William Leason to Dr Smithies 18 June 1986 DHSC0000783. No action in relation to the licence was however taken until October.
(2094) Memo from Dr Rotblat to Dr Smithies 10 June 1986 DHSC0000780
(2095) Letter from Dr Harris to UK Haemophilia Centre Directors 11 July 1986 MHRA0000078_008
(2096) Letter from Dr Rodell to Blood Bank Directors and Hemophilia Centre Coordinator 23 June 1986 p2 ARMO0000540. An internal DHSS minute of 17 July referred to the letter to haemophilia centre directors, stating “As the product licence holder (Rorer Health Care Ltd) claim to be in compliance with their product licence this matter has not been treated as a product defect. The Company have been in close contact with Dr Rotblat who is fully aware of the position.” Memo from A Snelling to Mr Franks 17 July 1986 DHSC0002335_076
(2097) Memo from Christopher Bishop to Dr Harris 16 July 1986 CGRA0000527
(2098) Memo from Christopher Bishop to colleagues 18 July 1986 pp1-3 ARMO0000562
(2099) Memo from Dr Harris to Graham Thomas 25 July 1986 p1 CGRA0000570
(2100) Memo from Christopher Bishop to colleagues 7 August 1986 ARMO0000568. He advised colleagues on the “lines” to be used in response to queries about the new heat treating procedure: “We would emphasise again that this move does not imply any lack in confidence in our current procedure (60° for 30 hours) in terms of HIV elimination/inactivation, but is designed to improve still further the safety factor in the product in terms of total viral inactivation”. Emphasis in original.
(2101) Letter from Robert Christie to Dr Rotblat 22 August 1986 p1 ARMO0000812
(2102) Both had been treated in 1986 with Factorate HT made from plasma from unscreened donors. Memo from Robert Christie to Dr Harris and Christopher Bishop 29 September 1986 p2 ARMO0000585. There were two further seroconversions at Birmingham Children’s Hospital in late 1986/early 1987. Dr Hill, writing in 2007, understood there to have been three definite cases and one probable case amongst his patients. Letter from Dr Hill to the Department of Health 28 January 2007 DHSC0004232_014
(2103) File notes re Dr Rotblat 1-2 October 1986 ARMO0000590
(2104) File notes re Dr Rotblat 1-2 October 1986 ARMO0000590
(2105) Minutes of Rorer Healthcare and DHSS meeting 3 October 1986 pp1-2 ARMO0000510. It appears that if Armour refused a voluntary withdrawal, the DHSS proposed to suspend the licences on grounds of safety. Minute from D O Hagger to Mr O’Connor 3 October 1986 DHSC0003963_145
(2106) Note of Armour and DHSS meeting 6 October 1986 DHSC0003963_137, Letter from Dr N Randall to Dr Duncan Thomas 7 October 1986 ARMO0000602
(2107) There is no documentation that shows the case being reported to the DHSS. Whilst informal communication by telephone or in a meeting is a possibility, there is no contemporaneous material to suggest that was the case – such as a follow-up letter to a meeting or telephone conversation, as happened on other occasions.
(2108) Clive Collins in his statement to the Inquiry said that he did discuss the Prince study with Dr Duncan at the DHSS on 19 December 1984 but that the study was not yet complete; he also set out his understanding that “the study was flawed and would need to be repeated and thus at that point in time it had no specific implication for the efficacy of Armour’s heat treatment process.” The note of the meeting with the DHSS on 19 December records that Clive Collins reported that the studies were having to be repeated due to viral assay difficulties; a copy of the CDC data was provided to Dr Duncan. Written Statement of Clive Collins paras 28-30 WITN7021001, Notes on informal DHSS meeting 19 December 1984 ARMO0000337. Robert Christie told the Inquiry that his understanding was that Dr Prince’s study was flawed and the results were unreliable and that “In those circumstances, it was not considered appropriate to inform others of the study results.” Written Statement of Robert Christie paras 36-37 WITN7500001. In the report of the Krever Inquiry, Mr Justice Krever found that Armour chose not to inform the Canadian Bureau of Biologics about Dr Prince’s findings; in his view, “Armour’s obligation was to convey safety-related information about its products to the bureau promptly. It could have addressed risk, if any, of confusion by including in a timely report to the bureau all the contradictory and inconsistent data it believed qualified Dr Prince’s findings.” The Krever Report 1997 p529 KREV0000001. The judge hearing a subsequent criminal case in Canada came to a different conclusion: “This was a time of great uncertainty. In the face of this, and in light of the clearly articulated studies of the CDC, supported by the FDA, it would have been unreasonable, if not irresponsible, for Armour to have thrust such confusing, incomplete and inconclusive information into the community.” Her Majesty The Queen and Armour Pharmaceutical Company, Michael Rodell, Roger Perrault, Donald Wark Boucher and John Furesz Judgment 1 October 2007 para 90 MDUN0000020_250
(2109) A report prepared by Dr Rotblat in February 1986 for the CMO repeated Armour’s claim that they had done viral inactivation studies “and shown good inactivation”; the data was to be sent to her. This presumably did not include the Prince data. Letter from Dr Isaacs to Dr Harris 18 February 1986 p3 DHSC0002295_011
(2110) See the chapter on Regulation of Commercial Factor Concentrates.
(2111) It is right to note that on or around 17 February 1986 Dr Rotblat contacted the companies manufacturing Factor 8 concentrates to draw together information for the CMO regarding their viral inactivation processes. No particular action appears to have been contemplated beyond the information gathering exercise, and awareness of the Lewisham case does not appear to have prompted any particular concern. Letter from Dr Isaacs to Dr Harris 18 February 1986 DHSC0002295_011
(2112) A DHSS memo records that on 14 February 1986 Dr Jones phoned the DHSS “to apologise for making so public his announcement about heat treated Factor VIII being unsafe … Dr Jones emphasised that whilst he accepted CMO’s reprimand and agreed the Departmental line he knew that there was strong evidence for the transmission of HTLV III by the Armour heat treated Factor VIII used for treatment of a case in Holland”. The memo also reported that Dr Biekerk of the Dutch Ministry of Health had now informed Dr Sibellas of the DHSS that “contrary to his initial information there is evidence of a case of seroconversion in a haemophiliac following the use of heat treated Factor VIII.” Memo from Dr Smithies to Dr Harris 17 February 1986 DHSC0002295_044
(2113) Memo from Robert Christie to Dr Harris and Christopher Bishop 29 September 1986 ARMO0000585
(2114) It appears that Dr Hill had not at this stage informed the parents of the children who had seroconverted. Minutes of Rorer Healthcare and DHSS meeting 3 October 1986 p2 ARMO0000510
(2115) The difference is permitting influencing the content, on the one hand, (“participation”) and ensuring fairness in being able to correct errors in an otherwise concluded draft on the other.
(2116) Christopher Bishop Transcript 4 November 2021 pp169-170 INQY1000158
(2117) The UK lacked the ease of access to laboratory screening to check on viral inactivation. Whereas in the US the degree of viral “kill” could be demonstrated in a laboratory to 4 or 5 logs, and the Robert Koch Institute in West Germany could test there, facilities available readily to do this in the UK were lacking. If they had not been lacking, then the UK could have had greater confidence that its heat treatments were sufficient on their own to protect users of products against the risks of infection. Without them, the dual reassurance spoken of in the text was the best that could be done. Written Statement of Dr James Smith para 88 WITN3433001. Dr Peter Foster Transcript 25 March 2022 pp138-139 INQY1000198
(2118) The explanation is that PFC had a 9-month supply of Factor 8 in stock, some of this having been processed in January 1985, and the total of plasma and product was 16 months’ supply.
Minutes of SNBTS Directors meeting 10 December 1985 p2 PRSE0002258
(2119) Fax from Karen Fernandez to Marie Tatt 20 February 1986 CGRA0000601
(2120) Minutes of SNBTS directors meeting 25 June 1986 p3 PRSE0002641
(2121) Memo from Brian Dyos and L Frith to Jack Wood 9 July 1986 CGRA0000608
(2122) Hansard written answer on blood products: screening 29 July 1986 CBLA0002320_001
(2123) Emphasis added. Letter from Dr Rizza to Dr Smithies 30 July 1986 OXUH0003771_003. His perspective was that of the clinician in England for whom this presented a dilemma: what did he see as the risk of using NHS product, half of which might have come from unscreened plasma, but from voluntary donors, as against commercial product which he was told by the pharmaceutical company had been made from screened plasma, but from donors who sold their plasma. He would have to factor in, too, the extent to which reliance could be placed on the assurances given, and the effectiveness of the viral inactivation processes adopted, in so far as there was reliable information about them. He recorded in the letter that the decision to use or not use the untested 8Y would ultimately depend on each director’s clinical judgement, but that he was prepared to use it in preference to heated commercial preparations that still transmitted NANBH.
(2124) Analysis of Parliamentary Question 466 6 February 1990 p3 BPLL0011217_001, Written Statement of Dr Terence Snape 8 February 2022 para 109 WITN3431001. Dr Geoffrey Scott, writing to Dr Helena Daly in 2000 did remember some product being recalled. Letter from Dr Scott to Dr Daly 29 June 2000 p2 WITN4685002. This is probably more likely to have been a batch recall than evidence of a general recall, particularly given the reasons Dr Snape has for saying one was unlikely.
(2125) Letter from BPL to Haemophilia Centre Directors and Regional Transfusion Directors 24 July 1985 CBLA0002224
(2126) Smith et al Interim Results of Surveillance for NANBH in Patients Receiving Heated Concentrates Produced in England Developments in Biological Standardization 1987 PRSE0004378 and Surveillance of Previously Untreated Patients for Possible Virus Transmission 30 September 1986 CBLA0002348
(2127) Smith et al Interim Results of Surveillance for NANBH in Patients Receiving Heated Concentrates Produced in England 1986 p3 WITN6914063. The commercial products were those produced by Hyland and Armour.
(2128) Minutes of CBLA meeting 9 July 1985 p5 BPLL0004117. Neither Dr Forrester of the Scottish Home and Health Department (“SHHD”), nor Dr McClelland of SNBTS were present, but would have received the minutes.
(2129) Dr Peter Foster Transcript 25 March 2022 pp89-90 INQY1000198
(2130) Dr Peter Foster Transcript 25 March 2022 p104 INQY1000198
(2131) Dr Peter Foster Transcript 25 March 2022 pp104-105 INQY1000198
(2132) Written Statement of Dr Peter Foster pp91-92 WITN6914001
(2133) Written Statement of Dr Peter Foster pp117-118 WITN6914001, Written Statement of Professor Christopher Ludlam para 350 WITN3428001
(2134) The Scottish Executive Report which asked whether there had been a culpable delay in Scotland providing a concentrate which did not transmit Hepatitis C was concerned centrally with this comparison of English achievement well before Scottish achievement. Though it did not actually answer the questions remitted to it, and it is not clear that it understood the explanation Dr Foster was to give, its conclusion that there was in this respect no blameworthy failure is correct. The Report, and the way it was handled, is considered later, in the chapter on Scotland.
(2135) Internal Cutter Memo 20 May 1985 BAYP0000024_230
(2136) This memo provides evidence that suggests there was no general shortage of heat-treated commercial concentrates in the UK, for why else would a commercial company be worried about losing market share? It also reveals that some haemophilia centre directors were taking the approach that it was unethical to use products more likely to transmit hepatitis, yet most such doctors had used such products rather than using single donor cryoprecipitate or small pool concentrates, or insisting on batch dedication, throughout the 1970s and early 1980s, as described in the chapter on Haemophilia Centres: Policies and Practice.
(2137) Not all commercial products were referenced in the memo. Thus, Behringwerke’s Haemate P was not. The first article reporting claims that it was free from HIV, hepatitis and herpes was published in April 1986: Hilfenhaus and Weidmann Pasteurization as an Efficient Method to Inactivate Blood Borne Viruses in Factor VIII Concentrates Arzneimittel-Forschung Drug Research 1986 MHRA0033407_006
(2138) Later in the memo a figure of 22% is given, though, for the same study (4 out of 18 patients in Kernoff et al Wet Heating for Safer Factor VIII Concentrate? The Lancet 28 September 1985 RLIT0000186).
(2139) Internal Cutter Memo 20 January 1986 p1, p3 CGRA0000578
(2140) To be joined in this hierarchy by Z8 when it was produced in Scotland during and after 1987.
(2141) Letter from Peter Coombes to Dr Otto Schwarz 7 July 1988 SHPL0000141_097
(2142) Recommendations on choice of therapeutic products for the treatment of non-inhibitor patients with Haemophilia A, Haemophilia B or von Willebrand’s disease 22 May 1988 NHBT0000037_014
(2143) The letter went on to state: “For patients in Scotland and Northern Ireland with haemophilia A, NHS 8Y is not available and we recommend either Z8 or the commercial products mentioned … For patients with haemophilia B: NHS 9A (Elstree) or in Scotland DEFIX (Edinburgh) should be used. For mildly or moderately affected patients with haemophilia A and von Willebrand’s Disease, desmopressin (DDAVP) should always be considered before use of blood products.” Recommendations on choice of therapeutic products for the treatment of non-inhibitor patients with Haemophilia A, Haemophilia B or von Willebrand’s disease 22 May 1988 p6 NHBT0000037_014
(2144) FEIBA stands for Factor 8 Inhibitor Bypass Activity: a product used where it appeared that the patient had developed inhibitors to Factor 8.
(2145) Haemophilia Society The Bulletin No4 1988 p1 HSOC0022932
(2146) Counsel Presentation on the Overview Chronology of the Licensing of Commercial Blood Products in the United Kingdom during the 1970s and 1980s 6 December 2022 p39 INQY0000411
(2147) Counsel Presentation on Domestic Production and Self-Sufficiency 15 March 2022 p88 INQY0000333
(2148) Volume 6, chapter 6.12
(2149) The evidence of Dr Foster, reviewed above, emphasises the extent to which commercial secrecy was important. See footnote 1928.
(2150) Or in the case of Immuno, probably chemically inactivated.
(2151) There is a cost to this, but it is a minor expense to provide or to resource a laboratory to carry out research into reduction of a known risk. It bears no comparison with, for instance, the outlay needed to rebuild BPL.
(2152) The word “donation” is Orwellian where it is used to describe the sale of a person’s plasma to a pharmaceutical company. It is in truth a purchase/sale, but in no conventional sense is it a “donation”/gift. Hence the use of the word “true” here.
(2153) The growth is demonstrated by the graphs in the chapter on Pool Sizes.
(2154) “The time” should be clear from the context, but for clarity as used here it means during the 1970s.
(2155) In the sense of undetectable because it had not yet been isolated, a test for its presence had thus not yet been developed, and it could not easily be known if any treatment could be effective.
(2156) A reasonably full list of risk reduction measures is: (a) the careful selection of donors, (b) the screening of donors, (c) the testing of donations for viruses or biochemical markers which might well be associated with the infection, (d) reducing the number of individual donations to the pools from which blood products were derived, (e) keeping a careful record which might show that a donor had fallen ill since making the donation (perhaps by using a “quarantine” period before the product was released, and withdrawing that product if any donor could in that period be shown to have succumbed to infection), (f) being prepared to recall any batch where it appeared that an infected person had contributed to it within a timescale which showed a risk that they might at the time have been infectious, even though they were unaware of it, or (g) inactivating the virus.
(2157) One piece of contemporaneous evidence to this effect is from 26 April 1978, making it clear that Hyland had a research project aimed at eliminating NANBH in factor concentrates that was being hindered by a lack of manpower and adequate funding. Internal Hyland Memo 26 April 1978 p3 CGRA0000215. See also the report by the Committee to Study HIV Transmission Through Blood and Blood Products, Institute of Medicine, Leveton et al HIV and the Blood Supply: An Analysis of Crisis Decisionmaking 1995 p109 JREE0000019, Expert Witness Report of Professor William Robinson 16 February 2001 p13 CGRA0000621, Deposition of Professor Frank Putnam in Re: Factor VIII or IX Concentrate Blood Products Litigation 15 April 1997 p64 CGRA0000616
(2158) Professor Edward Tuddenham Transcript 22 October 2020 pp66-71 INQY1000067. I have no hesitation in accepting this evidence from a witness whose contributions were clear, careful, thoughtful and balanced, and who gave no indication that he was pursuing a personal agenda.
(2159) Professor Michael Makris, of Sheffield, echoed it in his written evidence to the Inquiry. Especially paragraphs 34, 37 and 38. Written Statement of Professor Michael Makris WITN4033001
(2160) Written Statement of Dr Peter Foster para 33.1 WITN6914001
(2161) Horowitz et al Inactivation of viruses in labile blood derivatives Transfusion 4 February 1985 BAYP0000024_063
(2162) In the course of his evidence, Dr Foster pointed to several discoveries which had enabled PFC to produce a pasteurised heat-treated product by 1986/7.
(2163) Dr Peter Foster Transcript 25 March 2022 pp96-102 INQY1000198
(2164) ie unstable in heat; easily degraded. Written Statement of Dr Peter Foster for the Penrose Inquiry 29 June 2011 p11 PRSE0003349
(2165) A large protein, present in substantial quantities in the substrate being filtered. By comparison, Factor 8 is present in trace quantities.
(2166) Dr Foster concluded: “These observations confirmed that factor VIII activity could be destroyed by even a modest increase in temperature and it seemed inconceivable that factor VIII could be heat treated at a temperature high enough to eliminate the risk of hepatitis transmission.” SNBTS Briefing Paper on the Development of Heat Treatment and Coagulation Factors November 2010 p31 PRSE0002291
(2167) ie it was not started in response to the threat of AIDS. Leveton et al HIV and the Blood Supply: An Analysis of Crisis Decisionmaking 1995 p107 JREE0000019
(2168) Leveton et al HIV and the Blood Supply: An Analysis of Crisis Decisionmaking 1995 p109 JREE0000019
(2169) In the mid to late 1970s, when research most probably began in earnest.
(2170) Leveton et al HIV and the Blood Supply: An Analysis of Crisis Decisionmaking 1995 p240 JREE0000019
(2171) Leveton et al HIV and the Blood Supply: An Analysis of Crisis Decisionmaking 1995 p110 JREE0000019
(2172) Indeed, it took only a matter of months after starting intensive development of what was to become 8Y for there to be a first pilot batch: see Draft Proof of Evidence of Dr Richard Lane for HIV Haemophilia Litigation 10 December 1990 p431 CBLA0000005_002 and Draft Expert Witness Statement of Dr Terence Snape for the Tribunal of Inquiry into Infection with HIV and Hepatitis C of Persons with Haemophilia and Related Matters p12 NHBT0004065_003
(2173) These words come from the Institute of Medicine Report of 1995, Leveton et al HIV and the Blood Supply: An Analysis of Crisis Decisionmaking 1995 p107 JREE0000019
(2174) In the exchange between Counsel and Dr Foster set out in the text, he placed weight on a lack of knowledge of the precise structure of Factor 8. This was not, he said, determined until Professor Tuddenham’s work in the mid 1980s. Yet this plainly did not hold any of the pharmaceutical companies back. He placed weight on the difficulty of dealing with a possible virus, the structure of which was unknown. However, both BPL and PFC managed to inactivate NANBH before the structure of Hepatitis C was known. Indeed, throughout medical history doctors have treated disease without precise knowledge of the pathogens they were defending their patients against; for instance, the protective measures against cholera introduced after Dr John Snow’s work in mid 1800s London identifying that use of water from the Broad Street pump transmitted disease did not depend upon precise knowledge of the pathogen. It could not have been known for sure whether, and what degree of, heat would inactivate HIV before it was identified, but it was a fair bet that heat would, in just the same way as a GP faced with a patient apparently suffering a bacterial infection will often prescribe a broad spectrum antibiotic without first conducting tests to determine precisely what bacteria are responsible. Finally, as to his view that successful inactivation depended upon the circumstances in just one particular company, that is belied by the facts. Dr Peter Foster Transcript 25 March 2022 pp96-102 INQY1000198
(2175) Letter from Professor Bloom to GP 10 February 1975 p2 WITN0047002
(2176) Low, that is, when compared to the rates amongst the donor population in or used by the US.
(2177) An example is that of Professor Christopher Ludlam, whose reaction to the fact that a cohort of his patients in Edinburgh had tested positive for HTLV-3 was one of stunned disbelief at first, such that he took some time to act before even beginning to tell the patients concerned. See the chapter on Haemophilia Centres: Policies and Practice. Though this example is drawn from 1984, and arises in the context of AIDS, it demonstrates an attitude of over-heavy reliance on the protective effects of the voluntary non-remunerated donor principle.
(2178) The comment here applies to the US with greater force than it does to the UK because the main reasons for the absence of research in the UK were a belief that heat could not inactivate viruses without inactivating Factor 8 activity, an acceptance that hepatitis was an inevitable risk of the use of concentrates in therapy, and the poverty of resources and facilities in which meaningful research could be done into viral inactivation, with the result that no research was done beyond seeing if the viruses responsible might be removed by physical means such as filtration.
(2179) Alter at al The Ausria Test: Critical Evaluation of Sensitivity and Specificity Blood December 1973 p11 RLIT0002022
(2180) Universal childhood Hepatitis B vaccinations began in the UK only in 2017. The reasons for this relate to the fact that although a vaccine was available from the early 1980s it required a course of vaccination to gain immunity, and immunity waned; and it was preferentially given to those who worked in the health service amongst others thought to be at particular risk. Few children with haemophilia were vaccinated in the early 1980s. Jones Living with Haemophilia (extract) 1984 p4 PRSE0004552
(2181) Too slowly.
(2182) Concerns about yield and cost probably inhibited rapid progress in inactivation technologies. Leveton et al HIV and the Blood Supply: An Analysis of Crisis Decisionmaking 1995 p108 JREE0000019. The criticism here was not directed by the Institute of Medicine Committee at the pharmaceutical companies themselves: it was centrally a failure to encourage and incentivise them to take steps towards inactivation earlier than they did.
(2183) I do not intend in saying this to make any criticism of Drs Foster, Smith and others who were engaged in fractionation in the UK. The criticism is an institutional one – a failure of collective imagination and ambition coupled with a failure to provide appropriate resources, financial and material – for research to take place. The words of Dr Snape at the end of his testimony are consistent with this – see the conclusion of the chapter on Self-Sufficiency.
(2184) Leveton et al HIV and the Blood Supply: An Analysis of Crisis Decisionmaking 1995 p110 JREE0000019
(2185) Blood Products and Plasma Fractionation Laboratories 8 September 1978 pp11-12 CBLA0000840
(2186) Dr Maycock.
(2187) Letter from Dr Biggs to Dr Godber 22 August 1967 DHSC0100025_062
(2188) Blood Donors and the Transfusion Service British Medical Journal 27 July 1974 DHSC0100024_126
(2189) At the beginning of 1982 a remedial programme under the Medicines Act began to be implemented at Elstree. This mainly concerned production (of coagulation factors and albumin), but in addition some capital projects were undertaken. These included improving the virology lab. However, Dr Smith said in his written statement that “There were never any facilities or staff for virus work at PFL, and none at BPL capable of handling highly pathogenic viruses until completion of the new R&D Dept. in the late 1980s.” He added that “my evidence to the Oral Hearings in Penrose emphasises the defining limitation on our pasteurising work – we knew that it could not be exploited at BPL until the new plant had been completed and qualified”,and he described how he had to rely on PFC to carry out “exacting virus spiking experiments on dry-heated F.VIII and F.IX before BPL had acquired its own virus lab.” Written Statement of Dr James Smith paras 88, 90, 91 WITN3433001
(2190) Oxford being, of course, traditionally a home of cutting-edge research at its university.
(2191) Written Statement of Dr James Smith para 91 WITN3433001
(2192) Written Statement of Professor Geoffrey Savidge for the Archer Inquiry 17 September 2007 p9 ARCH0002508_002. He had a third reason too: a failure to restructure the Blood Transfusion Service. He expressed this as: “inferior reactive management to restructure the Blood Transfusion Service to introduce greater safety aspects with donor selection and improved productivity and efficiency to achieve self sufficiency.”
(2193) If not directly, then through other agencies.
(2194) World Health Organization Expert Committee on Hepatitis March 1952 pp4-5, p21 RLIT0000215
(2195) Murray Viral Hepatitis Bulletin of the New York Academy of Medicine May 1955 p6 MHRA0023509. Roderick Murray was the assistant chief at the Laboratory of Biologics Control in the National Microbiological Institute of the National Institutes of Health at Bethesda, Maryland. The high infectivity of hepatitis is echoed in Barker et al Transmission of Serum Hepatitis Journal of the American Medical Association 2 March 1970 MULL0002819, Gocke The Australia Antigen and Blood Transfusion Vox Sanguinis 1970 PRSE0004544 and Murray’s work is cited along with those two references by Dr Rosemary Biggs in a chapter on Complications of Treatment in her The Treatment of Haemophilia A and B and von Willebrand’s Disease 1978 p7 HSCO0000001
(2196) ie from human beings.
(2197) Ministry of Health paper on Prevention of Homologous Serum Jaundice for MRC Jaundice Committee on Administration and Field Aspects pp1-3 20 June 1944 DHSC0100008_051
(2198) Ministry of Health paper on Prevention of Homologous Serum Jaundice for MRC Jaundice Committee on Administration and Field Aspects 20 June 1944 p7 DHSC0100008_051
(2199) Minutes of MRC Jaundice Committee and Ministry of Health meeting 26 February 1945 DHSC0100008_091. The Cambridge drying plant was the unit which transferred to Elstree to become the Blood Products Laboratory (“BPL”). This was effectively deciding that the pool size used at the Cambridge drying plant for plasma should be reduced to a size of no more than 10 donors.
(2200) Minutes of Blood Transfusion Officers meeting 5 April 1945 p1 DHSC0100008_120
(2201) Spurling et al The Incidence, Incubation Period, and Symptomatology of Homologous Serum Jaundice British Medical Journal 21 September 1946 p3 RLIT0000052
(2202) Letter from Dr Maycock to Dr Dermot Lehane 27 September 1946 DHSC0100008_205
(2203) Truelove and Hogden A Documentary Study of Jaundice associated with Syphilis Treatment and Blood Transfusion British Journal of Preventive and Social Medicine 1947 pp9-10 RLIT0000211
(2204) Mollison Blood Transfusion in Clinical Medicine September1951 p179 RLIT0001567
(2205) Letter from Dr Drummond to Dr Maycock 6 January 1950 DHSC0100010_405
(2206) Mollison Blood Transfusion in Clinical Medicine September 1951 p179 RLIT0001567
(2207) World Health Organization Expert Committee on Hepatitis March 1952 p19 RLIT0000215
(2208) Drummond et al Homologous Serum Jaundice after transfusion of whole blood, dried small-pool plasma, dried irradiated plasma, and kaolin-treated filtered liquid plasma The Lancet 26 June 1954 p2 RLIT0000058
(2209) See the chapter on Viral Inactivation.
(2210) This assumes 200ml of plasma recovered from each donation of a pint of blood. A pint (568 ml) contains just over 310ml of plasma, but not all can be recovered. Biggs et al The Preparation and Assay of a Christmas-Factor (Factor IX) Concentrate and its Use in the Treatment of Two Patients British Journal of Haematology 1961 pp1-2 RLIT0000043_018
(2211) Maycock et al Further Experience with a Concentrate Containing Human Antihaemophilic Factor
British Journal of Haematology April 1963 p3, p23 BPLL0008150
(2212) Approximately 15 donors.
(2213) The authors also comment: “Being convinced that it had become possible to keep most of our haemophiliacs reasonably well and at school or at work instead of at home or in hospital, we realised that we wanted more concentrate than we could expect to receive. We could not accept the view that the production of adequate supplies for general treatment was impossible.” Holman and Wolf Human Antihaemophilic Factor: the preparation in a hospital of a concentrate for clinical use The Lancet 6 July 1963p2, p7, p8 HSOC0022517
(2214) Minutes of Working Party on Human Antihaemophilic Globulin meeting February 1964 p4 DHSC0100006_100
(2215) Minutes of Working Party on Human Antihaemophilic Globulin meeting 16 March 1964 p4 CBLA0009173. This working party was chaired by Professor Mollison (who wrote the leading textbook) and was attended by Drs Robert Macfarlane, Rosemary Biggs, Roger Hardisty, Ralph Kekwick and Dr Maycock and Leon Vallet among others.
(2216) Maycock Transmission of Hepatitis by Blood and Blood Products Proceedings of the Royal Society of Medicine November 1964 p3 RLIT0000065. It should be noted that at this stage the production of large-pool plasma from more than 300 donors had been abandoned: it was thought that above that level the risk of conveying serum hepatitis increased too much.
(2217) Grant Complications of blood transfusion The Practitioner August 1965 p6 PRSE0003897. It is important to note that she is probably describing dried plasma, rather than the pools to be used in fractionation to make blood products, where it appears that slightly larger pools were being suggested. However, in principle there can be little difference between the relative infectivity of a large pool to produce dried plasma and a large pool to produce a blood product, unless there is something intrinsic in the manufacturing process which begins to eliminate viral infection. None has been reliably suggested.
(2218) Cumming et al Red Cell Banking and the Production of a Factor VIII Concentrate Vox Sanguinis 1965 p3, p10 PRSE0003381
(2219) Letter from Dr Biggs to Dr Sheila Howarth 15 September 1967 MRCO0005072_011
(2220) Letter from Dr Biggs to Dr Sheila Howarth 15 September 1967 MRCO0005072_011
(2221) For reasons explained in the chapter on Pharmaceutical Companies, the minimum pool size used in the US was 1,000 donations, and frequently pools of this size were often combined to make concentrates.
(2222) Minutes of Edinburgh Regional Blood Transfusion Centre meeting 9 May 1968 p2 WITN3530076
(2223) Biggs Jaundice and Antibodies Directed against Factors VIII and IX in Patients Treated for Haemophilia or Christmas Disease in the United Kingdom British Journal of Haematology 1974 p6 HCDO0000581
(2224) Biggs Jaundice and Antibodies Directed against Factors VIII and IX in Patients Treated for Haemophilia or Christmas Disease in the United Kingdom British Journal of Haematology 1974 p6 HCDO0000581
(2225) Garrott Allen Post-Transfusion Hepatitis: A Serious Clinical Problem California Medicine1 April 1966 p1 MULL0002814
(2226) Kasper and Kipnis Hepatitis and Clotting-Factor Concentrates Journal of the American Medical Association 31 July 1972 PRSE0003913
(2227) Dr Biggs was an enthusiast for the development and use of factor concentrates, which she had been using to a limited extent in Oxford. Factor VIII Concentrates and the treatment of Haemophilia 1969 p10 PRSE0002553
(2228) This is not to be interpreted as meaning there was no increased risk – because the paragraph has just said there was a higher risk with freeze-dried preparation. It was just “not very much higher”. It is to be interpreted as saying that the increase in risk was not as great as theory might suggest. Again, there is a judgement to be made as to what counts as “not very much”.
(2229) Minutes of Expert Group on the Treatment of Haemophilia meeting 20 March 1973 p3 PRSE0004706
(2230) Letter from John Watt to Dr Iain Macdonald 16 March 1973 p1 SBTS0000309_023
(2231) Notes on a scheme to increase the preparation of Factor VIII Concentrate 1 June 1973 SBTS0000284_085, Minutes of Joint Steering Committee on Blood Products Production meeting 20 June 1973 PRSE0004359
(2232) Application for product licence 1 December 1972 p14 DHSC0105593_006
(2233) Memo from Dr Maycock to Dr Ethel Bidwell 8 December 1975 BPLL0003721. Dr Maycock thought that “the large pool size can be defended on the ground that starting plasma and concentrate are tested by RIA.”
(2234) Craske et al An Outbreak of Hepatitis Associated with Intravenous Injection of Factor-VIII Concentrate The Lancet 1975 PRSE0001794
(2235) Minutes of Haemophilia Centre Directors meeting 21 June 1976 pp4-5 OXUH0003735. It was recorded that commercial Factor 8 being derived from pools of 2,000 to 6,000 litres of plasma (equivalent, therefore to 10,000 to 30,000 donations) had a greater probability of including an infected donation.
(2236) See the chapter on Treloar’s and the knowledge of hepatitis linked to the pool size from which concentrates were made.
(2237) Lord David Owen Transcript 22 September 2020 p32 INQY1000055
(2238) Biggs Jaundice and Antibodies Directed against Factors VIII and IX in Patients Treated for Haemophilia or Christmas Disease in the United Kingdom British Journal of Haematology 1974 p14 HCDO0000581. This included the following: “The use of freeze dried concentrate (in comparison to cryoprecipitate) did not cause a dangerous increase in episodes of jaundice ... The evidence about the incidence of jaundice and antibodies in patients with haemophilia and Christmas disease does not suggest that either of these complications is clearly related to the type of human material used. Thus there would seem to be no disadvantage to the patient in greatly increasing the amount of freeze-dried concentrate and planning ultimately to replace cryoprecipitate by concentrate.” Biggs Jaundice and Antibodies Directed against Factors VIII and IX in Patients Treated for Haemophilia or Christmas Disease in the United Kingdom British Journal of Haematology 1974 p1, p14 HCDO0000581. What would constitute a “dangerous increase” was left undefined, and as pointed out in the text the article extrapolated from the results in respect of a product made from a mean pool size of 190 donors (for Factor 8) or one-sixth of the size of the pools which she was planning should be used.
(2239) Dr Biggs wrote: “the pooling of blood from many donors will increase the probability of including a sample containing some virus. It is obvious that volunteer donors and small pool fractionation methods will result in the safest plasma fractions. While these conclusions are not disputed it must be said that small pools of volunteer donor plasma cannot easily be reconciled with commercial fractionation practice and that the voluntary and national organisations, which can work with small pools of volunteer donor plasma, have not so far developed efficient fractionation programmes from which sufficient amounts of fractions are prepared.” Complications of Treatment in Biggs The Treatment of Haemophilia A and B and von Willebrand’s Disease 1978 p6 HSCO0000001
(2240) In effect the DHSS: see the chapter on Regulation of Commercial Factor Concentrates.
(2241) Minutes of Haemophilia Centre Directors meeting 21 June 1976 pp1-7 OXUH0003735
(2242) Dr Biggs did suggest, in an article in the British Journal of Haematology accepted in 1976, that it was well reported that commercial concentrates carried some ten times the risk of preparations made from voluntary donors, but this was not so much because of the larger pool size but the nature of the populations from which the blood was taken. In this article, bringing the survey of the UK experience of treatment up to date, hepatitis was mentioned neither in the summary nor the discussion – but there was a section on it. In this Dr Biggs repeated the comments she had made in her earlier article, mentioned in the text. She did not bring this up to date, though interestingly the raw data set out in Table X shows that in 1974 there had been a considerable rise in the number and proportion of incidents of hepatitis (by which was meant actual acute clinical illness). A number of cases of raised liver function tests were mentioned in passing, and not included, since many haemophilia centre directors had not recorded them: there had been no jaundice as such. It is a pity the article did not consider this more closely, since by now it was well appreciated that non-A, non-B Hepatitis might develop and it could well be chronic with little overt disease; however, the main purpose of the article was to encourage greater self-sufficiency, and to promote the idea that the future of treatment lay in producing more NHS concentrates, so no criticism attaches to this. The article, therefore, does not determine if the rise in the number and proportion of cases of hepatitis was linked to an increase in pool size, though it is certainly consistent with this. Biggs Haemophilia Treatment in the United Kingdom from 1969 to 1974 British Journal of Haematology 1977 pp11-14 PRSE0004645
(2243) Written Statement of Dr Terence Snape para 220 WITN3431001. See also: Dr Terence Snape Transcript 30 March 2022 pp19-23 INQY1000200
(2244) As Dr Diana Walford said: see the chapter on Regulation of Commercial Factor Concentrates.
(2245) Human Antihaemophilic Fraction Label 1 March 1976 CBLA0009269
(2246) Human Antihemophilic Fraction Label BPLL0001692_008
(2247) Dried Factor VIII Fraction Final Evaluation Form BPLL0001692_009
(2248) Dried Factor VIII Fraction Final Evaluation Form BPLL0001692_009: this was in respect of heat-treated 8Y.
(2249) Biggs Jaundice and Antibodies Directed against Factors VIII and IX in Patients Treated for Haemophilia or Christmas Disease in the United Kingdom British Journal of Haematology 1974 p6 HCDO0000581
(2250) Memo from Dr James Smith to Dr Richard Lane 13 January 1982 CBLA0001533, Memo from Dr Lane to Dr Smith 25 January 1982 BPLL0002070
(2251) Memo from Dr Snape to Peter Prince and Dr Smith 20 June 1986 CBLA0004791
(2252) Memo from Dr Lane to Dr Snape 29 January 1990 p3 BPLL0009120. He used a rough equivalent of five donations per litre ie 200ml donations apiece, assuming that the weight of the batch in kilograms equated to the number of litres. One litre of water at 4°C weighs 1kg. However, plasma is thicker than water, and therefore slightly heavier per litre; and the batch will not necessarily have been made at 4°C, so there is a margin of error around the figures though it is small.
(2253) Biggs Jaundice and Antibodies Directed against Factors VIII and IX in Patients Treated for Haemophilia or Christmas Disease in the United Kingdom British Journal of Haematology1974p6 HCDO0000581
(2254) Generic List of Documents of the Central Blood Laboratories Authority 17 May 1990 pp168-189 CBLA0014475
(2255) The basis for assuming that 1 litre equals approximately 5.55 donations, by assuming 180ml per donation, rests on: (a) Plasma needed for the preparation of anti-haemophilic concentrate 1973
CBLA0000154, (b) Minutes of Regional Transfusion Directors meeting 20 July 1973 p3 CBLA0000153, (c) conversions in a memorandum from Dr Maycock of 8 December 1975 in which a pool size is expressed in terms of both volume and donations, and it is plain that he has used a rate of 5.55 donations per litre Memo from Dr Maycock to Dr Bidwell 8 December 1975 BPLL0003721, (d) Therapeutic Materials used in Treatment of Coagulation Defects p5 CBLA0015427 and (e) Gunson Trends in blood transfusion practice in England and Wales Health Trends November 1986 p2 NHBT0017097
(2256) Written Statement of Dr Terence Snape para 213 WITN3431001, Value of SAG M systems in the provision of plasma products p1 CBLA0001779
(2257) Human Antihaemophilic Fraction Label 1 March 1976 CBLA0009269, Human Antihaemophilic Fraction Label 29 September 1976 BPLL0004430_001, Human Antihaemophilic Fraction Label 26 October 1976 BPLL0004429_001, Human Antihaemophilic Fraction Label BPLL0001692_008, Dried Factor VIII Fraction Final Evaluation Form BPLL0001692_009, Dried Factor VIII Fraction Label 12 February 1983 BPLL0010430_001, List of Factor 8 Labels 1985-1987 BPLL0002039, Factor VIII Batch Release Authorisation Dried High Purity Factor VIII 6 September 1988 BPLL0016009_161, 8Y Dried Factor VIII Fraction Label JPAC0000197_025, Blood Products Laboratory Background and Current Information for Members of the Central Blood Laboratories Authority June 1985 CBLA0002201, Human Antihaemophilic Fraction Label 26 October 1976 CBLA0009762, Human Antihaemophilic Fraction Label March 1976 CBLA0000046_017, Memo from Dr Maycock to Dr Bidwell 8 December 1975 BPLL0003721, Letter from Dr Lane to Thomas Dutton 11 January 1978 p4 CBLA0000711, Note on RIA Testing at the Blood Products Laboratory 18 January 1978 CBLA0000715, Letter from Dr Lane to Professor Mollison 28 July 1978 p7 CBLA0000801, Report to Advisory Sub-committee on Blood Products and Blood Group Reference Laboratories of the Central Committee of National Blood Transfusion Service 8 September 1978 p11 CBLA0000840, Letter from Dr Lane to Dr T Jones 20 November 1979 BPLL0002121, Report on Protein Fractionation Technology Working Party 18 August 1980 p13 CBLA0001152, Draft Third Report of the Advisory Group on Testing For the Presence of Hepatitis B Surface Antigen and Its Antibody September 1980 p7 CBLA0005371, Minutes of UK Haemophilia Centre Directors Hepatitis Working Party meeting 3 September 1980 pp2-3 HCDO0000553, Second Annual Report on Project Number J/S240/78/7 p4 HCDO0000135_021, Letter from Dr Craske to Dr Diana Walford 10 January 1983 DHSC0001104, A Comparison of Freeze-Dried Cryoprecipitate and Intermediate Purity Concentrates As Major Products For National Cell Sufficiency in Factor VIII 27 April 1981 p3 CBLA0001342_001, Memo from Dr Bidwell to Dr Lane 27 October 1980 CBLA0001192, Memo from Dr Smith to Dr Lane 13 January 1982 CBLA0001533, Memo from Dr Lane to Dr Smith 25 January 1982 BPLL0002070, Memo from Dr Snape to Peter Prince 10 June 1985 CBLA0002190, Memo from Dr Snape to Peter Prince and Dr Smith 20 June 1986 CBLA0004791, Memo from Dr Lane to Dr Snape 29 January 1990 BPLL0009120
(2258) Whilst Lord Owen told the Inquiry that he had some recollection of discussions about the relationship between the size of donor pools and the risks of hepatitis, there is no evidence of any later ministerial briefing on this issue. Lord David Owen Transcript 22 September 2020 p32 INQY1000055
(2259) He was director of BPL as well as consultant adviser on issues of blood transfusion; Drs Tovey and Gunson were the latter but not the former. Dr Lane succeeded Dr Maycock as director of BPL.
(2260) See Garrott Allen Post-transfusion hepatitis, a serious clinical problem California Medicine 1966 RLIT0000217, citing Mirick et al Modification of post-transfusion hepatitis by gamma globulin New England Journal of Medicine 1965 RLIT0002410 and Mosley The surveillance of transfusion-associated viral hepatitis Journal of the American Medical Association 1965 RLIT0000066 as supporting his striking “ten times” finding. Professor Garrott Allen repeatedly drew attention to the dangers of commercially obtained blood in causing serum hepatitis. Professor Richard Titmuss had also said as much in the widely read book The Gift Relationship. Titmuss The Gift Relationship 1970 pp113-114, pp144-154 HSOC0019917
(2261) World in Action Blood Money Part 2 Transcript 8 December 1975 p20 PRSE0004591, Letter from Dr Garrott Allen to Dr Maycock 13 February 1975 p1 MGIL0000001_003
(2262) Dr Owen participated in the World in Action Blood Money documentary in which the letter from Professor Garrott Allen was shown. A DHSS minute that referred to the documentary did not specifically mention the letter but recorded: “The Minister of State had been briefed and was concerned about the supply of the Factor and about the hazards of using it.” Minutes of Divisional Management Group meeting 25 November 1975 p3 MHRA0004180
(2263) Craske et al An Outbreak of Hepatitis associated with Intravenous Injection of Factor-VIII Concentrate The Lancet 1975 p2 PRSE0001794. Dr Craske also featured in the World in Action Blood Money documentary. World in Action Blood Money Part 1 Transcript 1 December 1975 p3 PRSE0004591. Dr Craske had explained the risk of larger pools to the reporter on the documentary, Michael Gillard, whose notes of the interview read: “1000 litres smallest profitable pool. Smallest 450 donors. 150 BTS [National Blood Transfusion Service] recommended … One donor can affect a pool … Difficult to know cut off point for numbers of donors in pool … F8 should only be used in emergencies and by qualified staff.” Blood Money interview notes 3 October 1975 MGIL0000058
(2264) In his written statement Dr Owen said “I had the Lancet and the BMJ on my personal reading so almost certainly I would have read the Craske article.” Written Statement of Lord David Owen para 10 WITN0663001
(2265) International Forum What is the Importance of the ‘Small Pool Concept’ in the Preparation of Fraction 1 and Cryoprecipitates for the Prevention of Post-transfusion Hepatitis? Vox Sanguinis 1980 p5 RLIT0000178. The size of a “small” pool is not defined, but many contributors to the forum were looking at limiting the number of donors to any one batch of product, or reducing the likely proportion of donors who would be infected by seeking to rely on voluntary rather than paid donations. Some expressed a reluctance to go back to small pools.
(2266) The phrase used is “all concerned in haemophilia therapy”. There is no evidence that people in the UK with bleeding disorders were told, despite this recommendation. Memo from Advisory Committee on the NBTS November 1980 p2 DHSC0000705
(2267) Memo from Advisory Committee on the NBTS November 1980 pp2-3 DHSC0000705
(2268) Agenda for Advisory Committee on the NBTS meeting November 1980 CBLA0003328
(2269) Memo from Dr Smith to Dr Lane 2 September 1980 CBLA0001157, Memo from Dr Lane to Dr Smith 29 September 1980 CBLA0001173
(2270) Memo from Dr Lane to Dr Smith 29 September 1980 CBLA0001173. According to Dr Snape: “regulatory approval was always sought when there were logistical reasons to increase pool size”. Written Statement of Dr Terence Snape para 220 WITN3431001. See also: Dr Terence Snape Transcript 30 March 2022 pp19-23 INQY1000200
(2271) Draft minutes of UK Haemophilia Centre meeting 30 September 1980 p1, pp9-10 HCDO0000248_003. Dr Smith represented Dr Lane at the meeting.
(2272) Memo from Dr Smith to Dr Lane 15 October 1980 p1 CBLA0001186
(2273) Approximately 800 donors using the figure PFC used for conversion of approximately 250ml per donation. Letter from John Watt to Dr Iain Macdonald 16 March 1973 pp1-2 SBTS0000309_023
(2274) A Review of Factor-VIII Recovery at PFC From April 1975 to August 1979 January 1980 p17 SBTS0003269_230
(2275) A litre of water at 4°C weighs 1kg. The approximate conversion is thus very close to 1kg plasma = 1 litre; and each plasma donation in Scotland was taken to be in the region of 250ml. Memo from Dr Foster to John Watt and others 29 December 1980 p3 PRSE0002177
(2276) Approximately 2,325 donations. Counsel Presentation on the size of pools of plasma used in domestic production of blood products in Scotland March 2022 para 18 INQY0000346
(2277) Counsel Presentation on the size of pools of plasma used in domestic production of blood products in Scotland March 2022 para 19 INQY0000346
(2278) Memo from Dr Brian McClelland to Dr Robert Perry and Dr Cash regarding events leading up to the recall of Factor VIII 20 November 1984 PRSE0000828, Letter from Dr Brian McClelland to Dr Cash regarding seroconversion in the Edinburgh cohort 15 November 1984 LOTH0000005_052, Memo from Dr Robert Perry to all PFC staff regarding AIDS in Scotland 31 January 1985 PRSE0000965
(2279) 3,300-5,500 donations. Foster and Dickson Control of large-scale plasma thawing Developments in Haematology and Immunology 1985 p4 PRSE0000232, Progress Report for Factor VIII Study Group February 1985 p4 PRSE0000927
(2280) Written Statement of Dr Robert Perry paras 271-281, paras 298-300 WITN6920001, Protein Fractionation Centre A Review of Factor VIII Recovery at PFC from April 1980 to September 1983 April 1984 pp8-9 SBTS0000238_009, Letter from Dr Cash to Anthony Deas 29 November 1990 SBTS0000041_126
(2281) Dr Smith recalled Dr Charles Rizza reporting that this product still resulted in some hepatitis transmission, “consistent with ‘one or two’ of even these highly-selected donors being infective.” Written Statement of Dr James Smith paras 120, 123, 129 WITN3433001
(2282) If Dr Biggs’ view were to be accepted as a reflection of the risks from pool sizes of fewer than 200 voluntary UK donations.
(2283) A paper by Dr Peter Kernoff, Dr Christine Lee and others published in 1985, recording patients followed up from April 1978 to March 1983, showed that it was close to 100% after first exposure, even though the crude figures could be interpreted as showing that those using NHS concentrates fared slightly – but only slightly – better than those using commercial concentrates. Kernoff et al High risk of non-A non-B hepatitis after a first exposure to volunteer or commercial clotting factor concentrates: effects of prophylactic immune serum globulin British Journal of Haematology 1985 HHFT0000221
(2284) By that time too, because self-sufficiency had not been achieved, and treatment policies were (broadly) centred on using more and more concentrates and less and less cryoprecipitate, there was a legitimate concern that changing to smaller pools would lead to less domestic production still, and the effect would then be to cause a greater use of commercial concentrates which posed their own, greater, risks to patients. Dr Foster, for instance, said that a reduction in pool size at that stage would have led to “an increase in importation of USA-donor derived Factor VIII concentrate which, in my opinion, carried a greater risk of HIV infection.” Written Statement of Dr Peter Foster para 61.6(ii) WITN6914001. His views were echoed by Dr Perry. Dr Robert Perry Transcript 31 March 2022 p117 INQY1000201
(2285) Trip Report of Meeting of Blood Products Advisory Committee on the Safety and Purity of Plasma Derivatives 19 July 1983 pp7-8 CBLA0000056_215, Minutes of Blood Products Advisory Committee meeting 19 July 1983 p3 BAYP0004674
(2286) Trip Report of Meeting of Blood Products Advisory Committee on the Safety and Purity of Plasma Derivatives 19 July 1983 pp7-8 CBLA0000056_215
(2287) This was Dr Rodell’s view, representing Armour and the US Pharmaceutical Manufacturers Association, and it was echoed in many of the discussions in the UK about the effects of suspending the import of commercial concentrates. However, as pointed out in this Report, the choice was not the binary one as he presented it – it was not a case of “treat with concentrate or not at all”. Cryoprecipitate was available (at least in the UK), for instance; and NHS concentrates though not wholly free from risk of transmitting the cause of AIDS were based on plasma donated by a population, which by comparison with those who sold their plasma in the US was relatively free of that risk at the time.
(2288) See the chapter on Haemophilia Centres: Policies and Practice.
(2289) Dr Terence Snape Transcript 30 March 2022 p59 INQY1000200
(2290) Dr Terence Snape Transcript 30 March 2022 pp61-62 INQY1000200. Dr Snape worked at PFL and BPL from 1970 to 2000 and was the scientist in charge of quality control at PFL from 1975 to 1981 and became head of quality control at PFL and BPL in 1982. Written Statement of Dr Terence Snape paras 5-15 WITN3431001
(2291) From the label of unheated Factor 8 issued before June 1985. List of Factor 8 Labels 1985-1987 BPLL0002039
(2292) The specific warning is: “the preparation is of human origin (less than 10,000 plasma donations used per batch). It has been subjected to heat treatment, in the vial, to reduce the risk of infection by viral agents (including hepatitis and AIDS viruses) but cannot be assumed to be free of the risk of infection.” List of Factor 8 Labels 1985-1987 BPLL0002039
(2293) See the label of Factor 8 issued from February 1987 onwards. List of Factor 8 Labels 1985-1987 BPLL0002039. Dr Terence Snape Transcript 30 March 2022 p69 INQY1000200
(2294) Dr Robert Perry Transcript 31 March 2022 pp172-177 INQY1000201
(2295) Response from SNBTS to Penrose Inquiry regarding Hepatitis Risk Warnings 8 June 2010 p11 PRSE0002726
(2296) Response from SNBTS to Penrose Inquiry regarding Hepatitis Risk Warnings 8 June 2010 p18 PRSE0002726
(2297) Response from SNBTS to Penrose Inquiry regarding Hepatitis Risk Warnings 8 June 2010 p4 PRSE0002726
(2298) Dr Robert Perry Transcript 1 April 2022 pp40-60 INQY1000202
(2299) Response from SNBTS to Penrose Inquiry regarding Hepatitis Risk Warnings 8 June 2010 p25 PRSE0002726
(2300) Dr Robert Perry Transcript 1 April 2022 p19 INQY1000202. By way of comment, if that is the case then what (in the case of these products) was the necessity of requiring a warning? The answer given by Dr Perry was because that was what the regulation and reference documents required. Dr Robert Perry Transcript 1 April 2022 p34 INQY1000202
(2301) British Pharmacopoeia 1973 to 1991: Dried Factor VIII Fraction p3 SBTS0002189
(2302) British Pharmacopoeia 1973 to 1991: Dried Factor VIII Fraction p6 SBTS0002189, Dr Robert Perry Transcript 1 April 2022 p24 INQY1000202
(2303) This is the way I interpreted his answers, though the passage is somewhat opaque:
“Q. Did PFC essentially assume that PFC, as the product manufacturer, did not need to spell out risks relating to non-A, non-B hepatitis because PFC assumed that clinicians would be spelling out those risks to their patients?
A. I think clinicians, as I understand it, would be trained in their requirement to have a sufficient knowledge of the risks associated with treatment, so that they could convey that to patients. And, like all other manufacturers, we were quite limited in the amount of information that it was appropriate to give to doctors or -- and certainly to patients. So I think your assumption is -- it is an assumption but it’s one based on a good knowledge of the people that we were working with and providing the products to.” Dr Robert Perry Transcript 1 April 2022 p36 INQY1000202
(2304) Dr Robert Perry Transcript 1 April 2022 pp42-44 INQY1000202
(2305) Effectively the licensing authority: see the chapter on Regulation of Commercial Factor Concentrates.
(2306) Mauser-Bunschoten et al Hepatitis C Infection and Viremia in Dutch Hemophilia Patients Journal of Medical Virology 1995 p1 PRSE0001143. Further, it cannot be argued that the paper which showed there was a near 100% risk of hepatitis for first treatment with factor concentrates and that NHS concentrates fared little better than commercial concentrates in this regard demonstrates that whatever the pool size infection was inevitable: that study was performed by following patients during 1978-1983 when pool sizes used in the NHS were growing exponentially. Kernoff et al High risk of non-A non-B hepatitis after a first exposure to volunteer or commercial clotting factor concentrates: effects of prophylactic immune serum globulin British Journal of Haematology 1985 PRSE0003439. Earlier studies, when pool sizes were smaller, did suggest a difference in infectivity: some are summarised in the introduction to the Report: Fletcher et al Non-A non-B hepatitis after transfusion of factor VIII in infrequently treated patients British Medical Journal 10 December 1983 p1 CBLA0001772. (Which also showed that by that time most patients receiving concentrate could expect to be infected). Indeed, the difference in infectivity had led for some 20 years to pools of more than 300 donations being avoided because of the increased risk. In the 1980s the pools were an order of magnitude greater.
(2307) Rollag et al Prevalence of Antibodies against Hepatitis C Virus in Norwegians with Congenital Coagulation Factor Defects Treated with Plasma Products from Small Pools European Journal of Clinical Microbiology and Infectious Diseases 1990 p1 RLIT0000286
(2308) Colvin et al A prospective study of cryoprecipitate administration: absence of evidence of virus infection Clinical and Laboratory Haematology 1987 NHBT0000095_003
(2309) Memo from Marietta Carr to members of Alpha Operations Committee 23 February 1984 p3 CGRA0000610. Attendees at the meeting chaired by Dr John Smith (NIBSC) included Dr John Petricianni of the Food and Drug Administration, representatives of the major pharmaceutical companies, Dr Thomas (NIBSC), Dr Craske, Dr Richard Tedder, Dr Cash, Dr Lane, Dr Snape and Dr Brian McClelland (SNBTS). The draft minutes of the meeting record that there “was much discussion about the optimal size of plasma pools, but no agreement that reduction of pool size would be either a practicable or a successful way to reduce the transmission of either hepatitis or AIDS”, suggesting a range of views on this topic. Draft Minutes of NIBSC Infectious Hazards of Blood Products meeting 9 February 1984 p10 PRSE0003071
(2310) Fletcher et al Non-A non-B hepatitis after transfusion of factor VIII in infrequently treated patients British Medical Journal 10 December 1983 CBLA0001772, Kernoff et al High risk of non-A non-B hepatitis after a first exposure to volunteer or commercial clotting factor concentrates: effects of prophylactic immune serum globulin British Journal of Haematology 1985 PRSE0003439